
Abstract
Introduction and hypothesis
This study was conducted to assess national rates in stress urinary incontinence (SUI) surgery in the USA from 1998 to 2007.
Methods
We utilized the 1998–2007 Nationwide Inpatient Sample and assessed women aged 20 years and older who underwent SUI surgery based on the International Classification of Diseases, 9th Revision (ICD-9) procedure and diagnosis codes.
Results
The total number of SUI surgeries performed during this 10-year period was 759,821. The annual number of procedures increased from 37,953 in 1998 to 94,910 in 2007. The type of SUI surgery performed also changed (p < 0.001). In 1998, retropubic suspensions represented 52.3%, decreasing to 13.8% in 2007. “Other repair of SUI” (ICD-9 59.79) comprised 22.4% in 1998, increasing to 75.2% in 2007, likely representing midurethral slings.
Conclusions
The total number and incidence rates of SUI surgeries have increased from 1998 to 2007. The type of SUI surgery performed has also changed significantly, likely secondary to adoption of midurethral slings.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Urinary incontinence is a prevalent condition with 16% of women suffering from bothersome leakage of urine [1]. This prevalence increases dramatically with age, and by 80 years, one third of all women will have significant symptoms. Urinary incontinence will become an even greater public health concern in the future, as the elderly population is expected to more than double from 38.7 million in 2008 to 88.5 million by 2050 [2].
Treatment for stress urinary incontinence (SUI) includes both nonsurgical and surgical options. Although numerous incontinence surgeries have been variably popular in recent decades, retropubic colposuspensions and traditional bladder neck slings have proven long-term efficacy [3]. However, these two procedures are not minimally invasive and require an abdominal incision. The midurethral mesh sling, a minimally invasive procedure that can be performed quickly with comparable outcomes to the Burch colposuspension [4], is now considered by many in the USA to be the new gold standard since its introduction in the USA 10 years ago [5].
Surgery for SUI has become more widely utilized [6, 7]. Two studies of US trends using the National Hospital Discharge Survey (NHDS) found that the total number of urinary incontinence procedures increased from 33,000 in 1979 to 84,000 in 1997 [6] and then to 103,467 in 2004 [8]. Furthermore, outpatient SUI surgery has increased from 34,968 in 1996 to 105,656 in 2006 [9]. While the NHDS provides national data, it is not as comprehensive as the Nationwide Inpatient Sample (NIS). For example, the 2004 NDHS includes 370,785 discharges from 439 hospitals [10] versus 8,004,571 discharges from 1,044 hospitals in the 2004 NIS [11]. Thus, evaluating trends through 2007 using the NIS may offer additional and more accurate insight into national practices. Furthermore, we will be able to assess whether or not the increasing number of outpatient procedures was reflected as a decrease in inpatient procedures.
Accurate information about the current numbers and types of SUI surgery in the USA will enable our field to assess the demand for skilled surgeons or understand the priority of training future gynecologists and urogynecologists. Without data regarding the type of surgeries being performed, we do not have nationally representative data to support the anecdotal impression that evidence-based surgeries like the midurethral sling have become widely adopted and ineffective surgeries such as Kelly plications and needle suspensions are no longer being performed. Lastly, given the higher prevalence of SUI in the elderly and more readily available minimally invasive techniques, we wanted to evaluate whether contemporary surgeons are performing surgical therapy on older women (despite the fact that they may have more comorbidities) than they have in previous years. Thus, the objectives of this study were to assess the national trends in inpatient surgical procedures for stress urinary incontinence from 1998 to 2007 and to evaluate whether the rates of surgery differ by demographic factors such as age using the Nationwide Inpatient Sample.
Materials and methods
We used the NIS as source data regarding inpatient surgeries for SUI [11]. The NIS is the largest publicly available database of hospital discharges in the USA. It contains data on five to eight million hospital discharges from approximately 1,000 hospitals, which are sampled randomly to yield a 20% stratified sample of US community hospital discharges. We elected to analyze the NIS dataset from 1998 to 2007 because the sampling and weighting strategy for the NIS changed in 1998.
Procedures and diagnoses were based on the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) codes. Each discharge in the NIS contains up to 15 procedure and 15 diagnosis codes. For this analysis, we included any discharge with both a urinary incontinence diagnosis and any SUI surgery procedure code. SUI procedure codes included the following: 59.3 plication of the urethrovesical junction, 59.4 suprapubic sling operation, 59.5 retropubic urethral suspension, 59.6 paraurethral suspension, 59.70 or 59.79 other repair of SUI, 59.71 levator muscle operation for urethrovesical suspension, or 59.72 injection of implant. The following ICD-9 diagnosis codes were used to confirm a diagnosis of urinary incontinence: 625.6 stress urinary incontinence, 599.82 intrinsic sphincter deficiency, 788.30 or 788.39 other urinary incontinence, 788.33 mixed incontinence, 788.34 incontinence without sensory awareness, or 788.37 continuous leakage.
We included female subjects who were 20 years or older and excluded women with a diagnosis of gynecologic, colorectal, or urologic malignancy. We abstracted data regarding age, race, primary payor, and length of stay. Hospital characteristics included geographic region (Northeast, Midwest, South, or West), location and teaching status (rural, urban non-teaching, or urban teaching), and hospital bed size (small, medium, and large).
Given the complex sampling design of the NIS, we used STATA 9.1 (StataCorp, College Station, TX, USA) to account for sampling weights, strata, and clusters. In addition, our research questions were formulated using the question diagram templates developed by Pietrobon et al. [12]. For each year from 1998 to 2007, we used the sampling weights provided in the NIS database to estimate and examine the total number and the type of SUI surgery performed. Crude and age-adjusted incidence rates were then calculated based on population data from the US Census Bureau [13]. For crude rates, the total number of SUI surgeries in a particular year was divided by the number of women aged 20 years or older in the same year. For age-adjusted rates, women were divided into 20-year age cohorts (ages 20–39, 40–59, 60–79, and ≥80 years), and age-adjusted rates were calculated using a direct method of standardization based on the published 2000 US Census adjustment weights by age [14]. By standardizing the data in this fashion, we adjusted for the potential impact of different age distributions during the study period. Rates of SUI surgeries over the study period were assessed using chi-square test for linear trends. We also assessed the crude incidence rate of surgery between elderly (age ≥65) and non-elderly. This study was exempt from institutional review board review because only publicly available data were analyzed.
Results
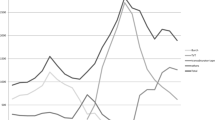
From 1998 to 2007, a total of 759,821 women underwent inpatient surgery for SUI. The total number of procedures per year increased from 37,953 in 1998 to 94,910 in 2007 (Table 1 and Fig. 1). A dramatic increase was seen from 2001 to 2002 with surgeries increasing from 34,584 to 117,235 annually. The crude incidence rates of inpatient SUI surgeries also increased during the entire study period from 37.2 to 84.3 per 100,000 women (p < 0.0001) with a similar marked increase from 2001 to 2002 (Table 1). The age-adjusted rates are also presented in Table 1.

Total number of stress urinary incontinence inpatient surgeries and different types of SUI surgeries in the USA based on the Nationwide Inpatient Sample data from 1998 to 2007
In 1998, the most common procedure was retropubic urethral suspension (52.3%) followed by “other repair of SUI” (22.4%) (Table 2). This finding had reversed by 2007, when the most common procedure was “other repair of SUI” (75.2%) followed by retropubic procedures (13.8%) (“other repair of SUI” represents the ICD-9 procedure code 59.79) (Table 2 and Fig. 1). Suprapubic slings remained the third most common procedure at 15.8% in 1998 and 8.2% in 2007. Notably, both paraurethral (needle) suspensions and plication of the urethrovesical junction (Kelly plication) decreased to 1.1% and 0.7% cases in 2007.
Women undergoing SUI surgery were similarly aged in 1998 and 2007 (Table 3). When age was dichotomized between non-elderly (≤65 years) and elderly (>65 years), a similar proportion of elderly women underwent surgery during these two periods. We assessed crude incidence rates in the non-elderly and elderly over the study period and noted that the rates in the elderly remained consistently higher than those in the non-elderly (Fig. 2). By 2007, the crude rates in non-elderly and elderly were 74.8 and 123.4 per 100,000 women, respectively. In terms of the types of SUI surgeries performed in the non-elderly versus the elderly, similar overall trends were seen in women ≥65 compared to the national trends, with an increase of “other repair of SUI” from 27.5% to 81.4% of procedures and a decrease of retropubic procedures from 40.2% to 7.5% when comparing 1998 to 2007. Caucasians were the most common racial group undergoing inpatient SUI surgery throughout the study period, whereas Hispanic women comprised 6.3% in 1998 and increased to 12.4% of inpatient SUI surgeries in 2007 (Table 3). Because some states do not collect race data for the NIS, race is shown as “missing” for 21.0–26.5% of the study cohort. We found that SUI procedures were performed in similar hospital settings in 1998 and 2007. A majority of surgeries were performed in hospitals with a large number of beds and in urban non-teaching and urban teaching hospitals (Table 3). The highest number of surgeries was performed in the South and the fewest in the Northeast, with little change over the study period.

Crude rates for SUI inpatient surgery in non-elderly (age <65) versus elderly (age ≥65) from 1998 to 2007
Discussion
Based on the Nationwide Inpatient Sample database, the number and rates of inpatient surgeries for urinary incontinence in women have increased during the time period from 1998 to 2007. In the last several years prior to this report, the annual number of women who underwent inpatient SUI surgery is over 90,000. We found that the type of SUI surgery most frequently performed has changed dramatically, with a pronounced shift toward “other repair of SUI” in 75% of cases and that the surgical rate in the elderly is higher than that in the non-elderly.
These estimates are fairly similar to those of prior studies of urogynecologic procedures using national databases. Using the NHDS data, Shah et al. [6, 15] found that 130,000 women had inpatient SUI surgery in 2003 and Oliphant et al. [8] reported that this estimate was 103,467 in 2004. As the NIS reflects over twice the number of hospitals as the NHDS (1,044 versus 439 in 2004) and over 20 times the number of discharges (8,004,571 versus 370,785 in 2004), we believe that evaluating national trends using the NIS is particularly valuable [16].
Regarding differences in the type of SUI surgery performed in 1998 versus 2007, it was encouraging to see that the proportion of paraurethral/needle suspensions and Kelly plications (urethrovesical plications) were low in 1998 and still lower by 2007, as studies have shown that these two procedures are not effective for long-term treatment of SUI [17–19]. In contrast, retropubic colposuspensions, traditional bladder neck slings, and midurethral slings are effective procedures for urinary incontinence [4, 20, 21]. While effective, Burch colposuspensions declined from 52.3% of procedures in 1998 to 13.8% of procedures in 2007, likely because of the wide adoption of the midurethral sling by clinicians. Unfortunately, there is no specific ICD-9 procedure code for a midurethral sling; midurethral slings can be coded as ICD-9 59.79 (“other repair of SUI”) or 59.4 (suprapubic sling). Given the fact that the proportion of “other repair of SUI” increased dramatically to 75.2% of all procedures in 2007 and suprapubic slings remained relatively low at 8.2%, we strongly suspect that this shift can be attributed to the adoption of midurethral slings in the USA and that midurethral slings are being coded as 59.79.
We noted a dramatic increase from 2001 to 2002 in both the total number of SUI surgeries and the number of “other repair of SUI” (Fig. 1). We postulate that characteristics of a midurethral sling (minimally invasive, short operating time, reasonable adverse event profile, and promising effectiveness data) may have encouraged providers who were not previously performing SUI surgeries to start performing this anti-incontinence procedure. We have attributed this increase to midurethral slings because of the timing of the following events: (1) in 1998, the FDA approved of the first midurethral sling, the tension-free vaginal tape (TVT) [5]; (2) in 2001, long-term 5-year data for the TVT were published that reported 84.7% subjective and objective cure rates with an additional 10.6% with significant improvement [22]; and (3) in 2002, the Ward and Hilton [23] randomized trial of Burch colposuspension and TVT found no significant differences in cure rates at 6 months. The timing of these events correlates well with the increase in “other repair of SUI” surgery, which shows a dramatic increase from 2001 to 2002 and then a more gradual increase after 2002. Interestingly, the trend of a dramatic increase in SUI surgeries after the introduction of the midurethral slings has been documented in other countries. In Australia, SUI surgeries almost doubled during the 3-year period after the introduction of midurethral sling [24], and in Belgium, there was a fourfold increase in the rate of surgery from 1997 to 2004, with this increase coinciding with the introduction of the TVT [25]. In contrast, there has not been a dramatic increase in SUI surgeries in Taiwan, and in 2005, slightly more retropubic procedures were performed compared to midurethral slings, 993 versus 819, respectively [26]. Given the growing elderly population in the USA, we wanted to compare surgery rates in the non-elderly versus elderly. Although the elderly population is at higher risk for morbidity and mortality from urogynecologic surgery [27], the rate of SUI surgery has been and remains higher in the elderly. This higher rate is likely secondary to a higher prevalence of urinary incontinence in older women [1]. With the changing demographics in the USA, it is likely that the total number of SUI surgeries will continue to increase in the future unless improved preventative strategies are developed.
The strengths of this study include the fact that we used a national US database, which is more representative and generalizable than local or regional data. In addition, we chose the Nationwide Inpatient Sample over the National Hospital Discharge Survey database which represents a greater number of hospitals and discharges and thus likely provides more accurate national estimates. Furthermore, we assessed trends in SUI surgery over 10 years instead of evaluating surgeries in just 1 year.
One of the limitations of this study is that by using the NIS, we are only able to account for inpatient procedures. The NIS does not include any outpatient procedural data. As of August 2009, the 2006 National Survey of Ambulatory Surgery was released, and Erekson et al. reported that 105,656 (95% CI 79,033–132,279) were performed in 2006 compared to 34,968 in 1996 [9]. They did not discuss the different types of SUI surgeries performed, but these data suggest that the number of SUI surgeries, both inpatient and outpatient in 2006, was 203,495 (97,839 inpatient + 105,656 outpatient). Thus, the total number of SUI surgeries performed in the USA is likely almost double those presented in this study when outpatient procedures are considered. Although there has been a dramatic increase in the number of outpatient SUI surgeries, the number of inpatient procedures has only decreased slightly from a high of 117,235 in 2002 to 94,910 in 2007.
Another limitation of our study is that the NIS uses ICD-9 codes, and there is not a specific code for midurethral slings. Although we suspect that these slings are the most common procedure currently performed, we cannot definitively prove this based solely on ICD-9 codes. However, our conclusion is based on the significant increase in “other repair of SUI” and the timing of this increase, which occurred after several key events regarding the TVT. Because the two largest national discharge databases, NHDS and NIS, both utilize ICD-9 codes, one important consideration will be to develop specific codes that reflect specific procedures such as the midurethral sling.
This study of the National Inpatient Sample demonstrates dramatic trends in inpatient SUI surgery in the USA, with over 90,000 procedures annually, and an incidence rate which has increased from 37.2 to 84.3 per 100,000 women. An increase in the rate of surgery was demonstrated both in the non-elderly as well as the elderly. Given the growing proportion of the elderly in the USA, it will be critical to train sufficient numbers of gynecologists and urogynecologists to care for women of all ages who suffer from stress urinary incontinence.
References
Nygaard I, Barber MD, Burgio KL, Kenton K, Meikle S, Schaffer J, Spino C, Whitehead WE, Wu J, Brody DJ (2008) Prevalence of symptomatic pelvic floor disorders in US women. JAMA 300:1311–6
Vincent GK, Velkoff VA (2010) The next four decades, the older population in the United States: 2010 to 2050. Current population reports. U.S. Census Bureau, Washington
ACOG (2005) Practice bulletin: urinary incontinence in women. Obstet Gynecol 105:1533–1545
Ward KL, Hilton P (2008) Tension-free vaginal tape versus colposuspension for primary urodynamic stress incontinence: 5-year follow up. Bjog 115:226–33
FDA. 510(K) Number K974098. Jan 28, 1998. http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMN/pmn.cfm?ID=114995. Accessed 5 Oct 2009
Boyles SH, Weber AM, Meyn L (2003) Procedures for urinary incontinence in the United States, 1979–1997. Am J Obstet Gynecol 189:70–5
Taub DA, Hollenbeck BK, Wei JT, Dunn RL, McGuire EJ, Latini JM (2005) Complications following surgical intervention for stress urinary incontinence: a national perspective. Neurourol Urodyn 24:659–65
Oliphant SS, Wang L, Bunker CH, Lowder JL (2009) Trends in stress urinary incontinence inpatient procedures in the United States, 1979–2004. Am J Obstet Gynecol 200(521):e1–6
Erekson EA, Lopes VV, Raker CA, Sung VW (2010) Ambulatory procedures for female pelvic floor disorders in the United States. Am J Obstet Gynecol 203(5):4971e.1–4971e.5
DeFrances CJ, Podgornik MN (2006) 2004 National Hospital Discharge Survey. Adv Data (371):1–19
HCUP Nationwide Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). 1998–2007. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/nisoverview.jsp
Pietrobon R, Guller U, Martins H, Menezes AP, Higgins LD, Jacobs DO (2004) A suite of web applications to streamline the interdisciplinary collaboration in secondary data analyses. BMC Med Res Methodol 4:29
U.S. Census Bureau (NP-D1-A) Annual projections of the resident population by age, sex, race, and Hispanic origin: lowest, middle, highest series and zero International Migration Series, 1999 to 2100.
Klein RJ, Schoenborn CA (2001) Age adjustment using the 2000 projected U.S. population. Healthy People 2010 Stat Notes (20):1–10
Shah AD, Kohli N, Rajan SS, Hoyte L (2008) The age distribution, rates, and types of surgery for stress urinary incontinence in the USA. Int Urogynecol J Pelvic Floor Dysfunct 19:89–96
DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A (2008) 2006 National Hospital Discharge Survey. Natl Health Stat Report (5):1–20
Nygaard IE, Heit M (2004) Stress urinary incontinence. Obstet Gynecol 104:607–20
Glazener CM, Cooper K (2004) Bladder neck needle suspension for urinary incontinence in women. Cochrane Database Syst Rev: CD003636
Bergman A, Elia G (1995) Three surgical procedures for genuine stress incontinence: five-year follow-up of a prospective randomized study. Am J Obstet Gynecol 173:66–71
Lapitan MC, Cody JD, Grant A (2009) Open retropubic colposuspension for urinary incontinence in women. Cochrane Database Syst Rev: CD002912
Albo ME, Richter HE, Brubaker L, Norton P, Kraus SR, Zimmern PE, Chai TC, Zyczynski H, Diokno AC, Tennstedt S, Nager C, Lloyd LK, FitzGerald M, Lemack GE, Johnson HW, Leng W, Mallett V, Stoddard AM, Menefee S, Varner RE, Kenton K, Moalli P, Sirls L, Dandreo KJ, Kusek JW, Nyberg LM, Steers W (2007) Burch colposuspension versus fascial sling to reduce urinary stress incontinence. N Engl J Med 356:2143–55
Nilsson CG, Kuuva N, Falconer C, Rezapour M, Ulmsten U (2001) Long-term results of the tension-free vaginal tape (TVT) procedure for surgical treatment of female stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 12(Suppl 2):S5–8
Ward K, Hilton P (2002) Prospective multicentre randomised trial of tension-free vaginal tape and colposuspension as primary treatment for stress incontinence. BMJ 325:67
Lee J, Dwyer PL (2010) Age-related trends in female stress urinary incontinence surgery in Australia—Medicare data for 1994–2009. Aust N Z J Obstet Gynaecol 50:543–9
Cammu H, Saeys F, Haentjens P (2010) Dramatic increase (1997–2007) in the number of procedures for stress urinary incontinence in Belgium. Int Urogynecol J Pelvic Floor Dysfunct 21:1511–5
Wu MP, Huang KH, Long CY, Tsai EM, Tang CH (2010) Trends in various types of surgery for hysterectomy and distribution by patient age, surgeon age, and hospital accreditation: 10-year population-based study in Taiwan. J Minim Invasive Gynecol 17:612–9
Sung VW, Weitzen S, Sokol ER, Rardin CR, Myers DL (2006) Effect of patient age on increasing morbidity and mortality following urogynecologic surgery. Am J Obstet Gynecol 194:1411–7
Acknowledgments
The authors thank Ricardo Pietrobon and “Research on Research” team, Duke University Health System (Jan 27, 2009, http://researchonresearch.org/).
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wu, J.M., Gandhi, M.P., Shah, A.D. et al. Trends in inpatient urinary incontinence surgery in the USA, 1998–2007. Int Urogynecol J 22, 1437–1443 (2011). https://doi.org/10.1007/s00192-011-1509-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-011-1509-x