
Abstract
Introduction and hypothesis
A subset of neurologically normal females void by efficient Valsalva, not detrusor contraction. We determined the incidence of urinary retention following midurethral sling (MUS) placement in women that void by detrusor contraction versus Valsalva.
Methods
Review of patients undergoing MUS insertion between 2002 and 2009 for urodynamic stress incontinence was performed. Women with concomitant pelvic surgery, previous incontinence surgery, or preoperative incomplete bladder emptying were excluded. Patients were divided into two cohorts based on preoperative urodynamic findings—those that voided with a detrusor contraction >10 cm of water and those that voided by Valsalva.
Results
One hundred seven patients were available for analysis. The postoperative urinary retention rate was 22% and 5% in the Valsalva and non-Valsalva groups, respectively (p < 0.05). Mean retention duration was 3 weeks for each cohort (range 1–6).
Conclusions
Women voiding by Valsalva are at increased risk of urinary retention following MUS placement.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Since its introduction in 1995 [1], the midurethra sling (MUS) has emerged as a standard surgical treatment for female stress urinary incontinence (SUI). Cure rates for SUI following the procedure approach 90% [2–4]. While complications associated with MUS placement are relatively low [5], the development of postoperative urinary retention is commonly encountered. Urinary retention after MUS surgery has been reported in 2% to 40% of patients depending on the definition used, duration of urinary retention, technique of MUS placement utilized, and whether or not concomitant pelvic surgery was performed [6–8].
Previously published literature reported that a significant minority of neurologically normal women empty their bladder by Valsalva and not with a detrusor contraction [9]. Limited data exist which specifically examine the risk of urinary retention following MUS placement in women who void by Valsalva versus those who void by detrusor contraction. As a result, we retrospectively compared the rates of postoperative urinary retention following MUS surgery for treatment of urodynamic SUI in women that void by detrusor contraction versus Valsalva.
Materials and methods
Following local institutional review board approval, we retrospectively reviewed the medical records of all women who underwent MUS placement for urodynamic SUI from 2002 to 2009. Prior to surgery, each patient received a thorough urologic history and physical examination. Additionally, all patients underwent preoperative video urodynamic studies to confirm the diagnosis of SUI and to determine voiding characteristics. Urodynamics consisted of medium-fill cystometry with dilute contrast (30–50 mL/min) via a 6-Fr double-lumen urethral catheter. A 6-Fr rectal catheter was utilized to measure abdominal pressure. Valsalva leak point pressure (VLPP) testing was performed in seated and standing positions at incremental volumes of 150 mL and then at capacity. The lowest VLPP (absolute pressure) was recorded. Study exclusion criteria included previous SUI surgery, concomitant pelvic surgery, and/or a preoperative post void residual (PVR) urine volume >75 mL.
Patients were divided into two cohorts based on preoperative urodynamically measured voiding characteristics—those that voided with a detrusor contraction >10 cm of water and those that voided by Valsalva. Similar to previously published studies, we defined Valsalva voiding as generating a urine stream via abdominal strain with a detrusor contraction ≤10 cm of water [10, 11].
All patients underwent MUS placement under general anesthesia on an outpatient basis. Postoperative urinary retention was defined as either the inability to void prior to discharge from the day surgery recovery room or a PVR urine volume >150 mL as measured by either bladder ultrasound or straight catheterization. Retention patients were given the choice of either performing clean intermittent catheterization or having a Foley catheter placed. Symptom updates and postvoid bladder ultrasounds were performed on all patients at 1 and 6 weeks postoperatively. Urinary retention patients were followed weekly until resolution.
Information abstracted from medical records included method of MUS placement (retropubic or transobturator), previous or concomitant pelvic surgery, VLPP, voiding detrusor pressure at maximum urine flow (PdetQmax), preoperative and postoperative PVR urine volumes, and surgical complications. Both cohorts were then evaluated and compared with regards to the development of urinary retention following MUS placement. Fisher’s exact test was used to determine statistical significance.
Results
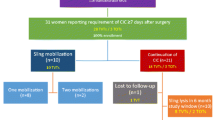
Three-hundred and fifty-four women underwent MUS placement for the management of urodynamic SUI by one of four specialty trained pelvic surgeons (RCO, MG, SK, or JN). Two-hundred and forty-seven patients were excluded, mostly secondary to concomitant pelvic surgery or a history of previous SUI procedures. Of the 107 remaining women, 75 (70%) voided by detrusor contraction and 32 (30%) emptied their bladder by efficient Valsalva. Preoperative characteristics of the two cohorts are listed in Table 1. No significant differences were noted between the two groups with the exception, as expected, of PdetQmax.
Urinary retention was observed in four out of 75 (5%) and seven out of 32 (22%) of detrusor contraction and Valsalva voiding cohorts, respectively (p < 0.05). Surgical outcomes for the two cohorts stratified by surgical technique are listed in Table 2. The mean duration of urinary retention was 3 weeks (range 1–6) in both cohorts. Sling lysis was required for two patients in each group. All four lysed MUS were placed retropubically. No women who voided to completion immediately after surgery developed subsequent incomplete bladder emptying.
Reported surgical complications included de novo urge incontinence (six out of 107, 6%), trochar bladder perforation (five out of 107, 5%), and femoral nerve injury (one out of 107, 1%). All patients with de novo urge incontinence were in the detrusor contraction cohort. All cases resolved with either observation or anticholinergic medication.
Discussion
MUS placement is a safe and efficacious treatment for women with SUI [12]. The procedure may be complicated by postoperative voiding dysfunction such as urinary retention or incomplete bladder emptying. Our study specifically examined the rates of postoperative urinary retention in women that void by either detrusor contraction or Valsalva.
Several previously published studies suggested an association between inadequate detrusor contraction and postoperative urinary retention after anti-incontinence surgery. Bhatia and Bergman found that women with poor detrusor contractility and Valsalva voiding that underwent Burch retropubic urethropexy were at 12 times greater risk of requiring prolonged postoperative catheterization when compared to patients who demonstrated adequate preoperative bladder contractions [10]. Weinberger and Ostergard noted similar findings in women following polytetrafluoroethylene suburethral sling placement [13]. Miller et al. reported a 19% rate of urinary retention in women undergoing pubovaginal sling placement who voided without a detrusor contraction [11]. Lemack et al. evaluated women who underwent either Burch colposuspension or pubovaginal sling for SUI management. The results did not suggest that abdominal straining was associated with postoperative urinary retention. However, in this study, postoperative voiding dysfunction was defined as the need for a catheter at any time beyond 6 weeks after surgery or the need for sling/suspension takedown [14]. It is conceivable that their conclusions would have been different if the authors chose a less conservative definition of postoperative voiding dysfunction. To our knowledge, no other study has specifically evaluated the rate of incomplete bladder emptying following synthetic MUS placement in patients that void with or without detrusor contraction. Our findings demonstrated that females who voided by detrusor contraction had a 5% rate of urinary retention after MUS placement as compared to 22% in the Valsalva group (p < 0.05).
The literature supports a direct correlation between the preoperative uroflowmetry and postoperative voiding dysfunction. Duckett et al. found that a pressure flow rate less than 15 mL/s, in addition to general anesthesia and voiding without a detrusor contraction, were associated with early postoperative incomplete bladder empting following sling placement [15]. Wheeler and colleagues similarly reported maximum preoperative pressure flow rates are a successful predictor of passing an initial voiding trial after MUS surgery [16]. Salin et al. published that a flow rate less than 15 mL/s, as well as increasing age, are independent predictors of postoperative voiding dysfunction following MUS surgery. Interestingly, of the patients in their study who developed incomplete bladder emptying, 70% did not exhibit any clinical symptoms [17]. This report differed from most other studies, including ours, in that voiding dysfunction was not based upon clinical symptoms but rather on changes in postoperative urodynamic parameters. Miller et al., however, reported findings contrary, noting that preoperative peak flow rates were not associated with developing urinary retention [11]. Our findings did not suggest that preoperative peak flow rates were predictive of postprocedural urinary retention.
The duration of retention in both the detrusor contraction and Valsalva voiding groups was short—mean of 3 weeks (range 1–6 weeks). Most of the cases of incomplete bladder emptying were self-limited and did not require further operative intervention. Two patients in each cohort underwent sling lysis. All four patients undergoing sling lysis had retropubically placed slings. The number of women in our study is not sufficient enough to determine if Valsalva voiding patients have better outcomes with regards to bladder emptying following transobturator rather than retropubic MUS. We have recently started recommending that Valsalva voiding patients undergo pelvic floor physical therapy/biofeedback prior to MUS placement in an attempt to minimize the risk of postoperative urinary retention. Further follow-up is warranted to determine if this intervention is effective in preventing postoperative incomplete bladder emptying.
Several limitations exist with regards to our study. First, MUS placement was performed by four different surgeons. All surgeons saw patients from the same referral pool and performed the same preoperative evaluations. Despite these similarities, different surgical techniques and styles may have introduced bias to the results. Secondly, our study was retrospective in design. A randomized, prospective trial would be beneficial in determining the true rate of incomplete bladder emptying in women who void by Valsalva following MUS placement.
Conclusions
MUS placement is a widely successful treatment modality for female SUI. Our findings suggest that Valsalva voiders are at significantly increased risk of urinary retention following MUS surgery when compared to women who void by detrusor contraction (22% versus 5%, p < 0.05). Most cases are self-limited and do not require further surgical intervention. Women that void by Valsalva should be counseled about the increased risk of postoperative incomplete bladder emptying prior to undergoing MUS surgery.
Abbreviations
- MUS:
-
Midurethral sling
- SUI:
-
Stress urinary incontinence
- PVR:
-
Postvoid residual
- VLPP:
-
Valsalva leak point pressure
- PdetQmax:
-
Voiding detrusor pressure at maximum urine flow
- PTFE:
-
Polytetrafluoroethylene
References
Petros P, Ulmsten U (1995) Intravaginal slingplasty. An ambulatory surgical procedure for treatment of female urinary stress incontinence. Scand J Urol Nephrol 29:75–82
Morey AF, Medendorp AR, Noller MW et al (2006) Transobturator versus transabdominal mid urethral slings: a multi-institutional comparison of obstructive voiding complications. J Urol 175:1014–1017
Paick J, Cho MC, Oh S et al (2007) Factors influencing the outcome of mid urethral sling procedures for female urinary incontinence. J Urol 178:985–989
Charalambous S, Touloupidis S, Fatles G et al (2008) Transvaginal versus transobturator approach for synthetic sling placement in patients with stress urinary incontinence. Int Urogynecol J 19:357–360
Jones R, Abrams P, Hilton P et al (2010) Risk of tape-related complications after TVT is at least 4%. Neurourol Urodyn 29:40–41
Klutke C, Siegel S, Carlin B et al (2001) Urinary retention after tension-free vaginal tape procedure: incidence and treatment. Urology 58:697–701
Barron KI, Savageau JA, Young SB et al (2006) Prediction of successful voiding immediately after outpatient mid-urethral sling. Int Urogynecol J 17:570–575
Meschia M, Bertozzi R, Pifarotti P et al (2007) Peri-operative morbidity and early results of a randomized trial comparing TVT and TVT-O. Int Urogynecol J 18:1257–1261
Miller ER (1996) Physiology of the lower urinary tract. Urol Clin N Am 23:171–176
Bhatia NN, Bergman A (1984) Urodynamic predictability of voiding following incontinence surgery. Obstet Gynecol 63:85–91
Miller EA, Amundsen CL, Toh KL et al (2003) Preoperative urodynamic evaluation may predict voiding dysfunction in women undergoing pubovaginal sling. J Urol 169:2234–2237
Debodinance P, Delporte P, Engrand JB et al (2002) Tension-free vaginal tape (TVT) in the treatment of urinary stress incontinence: 3 years experience involving 256 operations. Eur J Obstet Gynecol Reprod Biol 105:49–58
Weinberger MW, Ostergard DR (1996) Postoperative catheterization, urinary retention, and permanent voiding dysfunction after polytetrafluoroethylene suburethral sling placement. Obstet Gynecol 87:50–54
Lemack GE, Krauss S, Litman H et al (2008) Normal preoperative urodynamic testing does not predict voiding dysfunction after Burch colposuspension versus pubovaginal sling. J Urol 189:2076–2080
Duckett JR, Patil A, Papanikolaou NS (2008) Predicting early voiding dysfunction after tension-free vaginal tape. J Obstet Gynaecol 28:89–92
Wheeler TL, Richter HE, Greer WJ et al (2008) Predictors of success with postoperative voiding trials after a mid urethral sling procedure. J Urol 179:600–604
Salin A, Conquy S, Elie C et al (2007) Identification of risk factors for voiding dysfunction following TVT placement. Eur Urol 51:782–787
Acknowledgments
None
Funding
None
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pham, K.N., Topp, N., Guralnick, M.L. et al. Preoperative Valsalva voiding increases the risk of urinary retention after midurethral sling placement. Int Urogynecol J 21, 1243–1246 (2010). https://doi.org/10.1007/s00192-010-1177-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-010-1177-2