
Abstract
We report a case of vesicovaginal fistula associated to a vaginal foreign body. A 72-year-old woman consulted our clinic complaining of severe urinary incontinence. The leakage was continuous and significant and she was feeling a “vaginal mass”. Pelvic examination was suspicious for an advanced vaginal cancer, but further investigations showed the presence of a retained vaginal foreign body complicated by perforation of the bladder.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vesicovaginal fistulas are usually a complication of obstructed childbirth or pelvic surgery, most commonly hysterectomy [1, 2]. A more rare, and difficult to treat, cause of fistula is the retention of a foreign body. Most cases report about neglected vaginal pessaries [3], but fistulas due to the insertion of foreign bodies during masturbation, sexual intercourse, or with contraceptive purposes are also described [16]. Surgical treatment of vesicovaginal fistulas caused by foreign bodies is made difficult by the associated chronic inflammatory reaction.
Case report
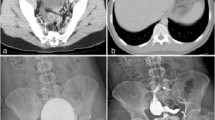
C.D., a 72-year-old woman, consulted our clinic on April 2007 complaining of a recent onset of urinary incontinence. She was nulliparous, but there were several illegal abortions in her clinical history. The urinary leakage was continuous and significant and she was feeling a “vaginal mass”. Two years before, she had been examined by another gynecologist who described a 2-cm vaginal nodule and did not prescribe further investigations. Pelvic examination was difficult due to the patient’s pain and evidenced a hard obstructing vaginal mass, strongly suspicious for an advanced vaginal cancer. We observed a continuous urine leakage from the vagina but we were not able to locate the fistula. Rectal examination did not reveal any parametrial involvement. A punch biopsy was taken, but in the sample there were only necrosis and angioblastic reactive tissue. The patient was then admitted to be examined under anesthesia in order to obtain an excisional biopsy. During the examination, a plastic foreign body was found, incorporated in the above described mass; a rigid cystoscopy located the foreign body proximally the bladder neck, among the ureteral orifices; the distension of the bladder was impossible due to the leakage of the irrigation fluid through the vagina. The CT scan was not able to provide more precise information about shape and size of the foreign body, but it showed some fluid inside the uterus and a left ovarian cyst; transvaginal ultrasound identified a tubular-shaped object positioned between bladder and vagina, and confirmed the suspicion of a pyometra and the ovarian cyst. The patient denied any knowledge of a vaginal foreign body. She was discharged with a bladder catheter and then re-admitted for laparotomy. The pre-operative blood tests did not show any sign of infection. After 1 week, TAH + BSO was performed; thereafter, the bladder was incised and opened at the dome longitudinally, two ureteral stents were placed after identifying the ureteral orifices, and the foreign body extracted (Fig. 1). It was roughly fixed to the adjacent structures due to the inflammatory reaction. At the end of this procedure, a very large defect extended from the trigone to the bladder neck and then to the ventral portion of the posterior urethra; luckily, the anterior urethra was intact. The trigone and the bladder neck were sutured with polyglactin 3/0 until urethra was reached. Thereafter, a Foley catheter was passed under direct vision from outside to inside the bladder that was closed with a running suture in polyglactin 1/0. Bladder was filled with 200 ml of saline solution without evidence of leakage. The catheter was then identified in the vagina; the urethral margins were dissected bluntly from the anterior vaginal wall and sutured with polyglactin 3/0, then the vaginal defect was sutured over the urethra. Again, the injection of saline solution among catheter and urethra did not evidence any leakage. No one of us was able to identify the object that caused the fistula (Fig. 1); it was similar to a Gellhorn pessary, but made of hard plastic, with a metallic tip. Moreover, Gellhorn pessaries are not used in Italy. The patient was discharged 12 days later and she kept a Foley’s catheter for 1 month. After it was removed together with the ureteral stents, the fistula was healed, but the vagina was completely sealed and the patient experienced a severe stress urinary incontinence. After 8 months, she was treated with urethral injections of a bulking agent and she is now dry. The patient has given her written informed consent to the publication of this case report.

The vaginal foreign body (3 × 5 cm)
Discussion
In a recent review, a series of vaginal fistulas due to neglected vaginal pessaries is presented [3]. It is undoubtedly a rare clinical problem. An even more uncommon clinical situation is a fistula secondary to a foreign body, inserted for sexual gratification or contraceptive purpose. Table 1 summarizes a review of the literature about vesicovaginal fistulas secondary to neglected vaginal foreign bodies [4–16]. There are many similarities in those case reports. The majority of the patients were middle-aged or young women. Anamnestic investigation was often unsuccessful because usually patients deny any knowledge of vaginal retained objects. Most items were incorporated in reactive fibrous tissue with or without calcification and were identified only after extraction. They were mainly plastic aerosol caps. A delayed abdominovaginal correction was the most common treatment of the fistula and it was successful in all cases. To our knowledge, our patient is the oldest one presenting with such an uncommon clinical problem. In our case, clinical and radiological pre-surgical investigations were also unable to show us the exact shape of an item that we could only partially see in the vaginal reactive tissue. We were unable to identify that object even after the extraction. We performed an immediate correction of the fistula using a combined abdominovaginal approach to reconstruct bladder neck, posterior urethra and anterior vaginal wall. We decided to repair the fistula in one step because of the large size of the defect we created extracting the foreign body. Our feeling is that the real incidence of major complications of vaginal foreign bodies is underestimated. Probably in our case, an earlier diagnosis (2 years before?) could have avoided such an invasive surgical procedure.
Abbreviations
- TAH:
-
Total abdominal hysterectomy
- BSO:
-
Bilateral salpingo-oophorectomy
References
Meyer L, Ascher-Walsh CJ, Norman R, Idrissa A, Herbert H, Kimso O, Wilkinson J (2007) Commonalities among women who experienced vesicovaginal fistulae as a result of obstetric trauma in Niger: results from a survey given at the National Hospital Fistula Center, Niamey, Niger. Am J Obst Gynecol 197:1 90.e1–90.e4
Vakili B, Chesson RR, Kyle BL, Shobeiri SA, Echols KT, Gist R, Zheng YT, Nolan TE (2005) The incidence of urinary tract injury during hysterectomy: a prospective analysis based on universal cystoscopy. Am J Obst Gynecol 192(5):1599–1604
Arias EB, Ridgeway B, Barber M (2008) Complications of neglected vaginal pessaries: case presentation and literature review. Int Urogynecol J 19:1173–1178
Sinha A, Olah KS (2005) Vesicovaginal fistula caused by a foreign body: delayed presentation and repair with Martius graft. J Obstet Gynaecol 25(2):223–224
Fourie T, Ramphal S (2001) Aerosol caps and vesicovaginal fistulas. Int J Gynaecol Obstet 73:275–276
Siddiqui NY, Paraiso MF (2007) Vesicovaginal fistula due to an unreported foreign body in an adolescent. J Pediatr Adolesc Gynecol 20:253–255
Hirai K, Kita K, Mikata K, Fujikawa N, Kitami K (2005) Vesicovaginal fistula associated with a vaginal foreign body: a case report. Hinyokika Kiyo 51:283–286
Arikan N, Türkölmez K, Aytaç S, Gögüs O (2000) Vesicovaginal fistula associated with a vaginal foreign body. BJU Int 85:375–376
Hanai T, Miyatake R, Kato Y, Iguchi M (2000) Vesicovaginal fistula due to a vaginal foreign body: a case report. Hinyokika Kiyo 46:141–143
Dalela D, Agarwal R, Mishra VK (1994) Giant vaginolith around an unusual foreign body—an uncommon cause of urinary incontinence in a girl. Br J Urol 74:673–674
Binstock MA, Semrad N, Dubow L, Watring W (1990) Combined vesicovaginal–ureterovaginal fistulas associated with a vaginal foreign body. Obstet Gynecol 76:918–921
Unda Urzaiz M, Prieto Ugidos N, Iriarte Soldevilla I, De Soto Arranz C, Flores Corral N (1989) Vesicovaginal fistula in an 8-year-old girl. Arch Esp Urol 42:473–475
Mhiri MN, Amous A, Mezghanni M, Rekik S, Smida ML (1988) Vesico-vaginal fistula induced by an intravesical foreign body. Br J Urol 62:271
Methfessel HD (1987) Rare foreign body fistulas of the female bladder. Z Urol Nephrologie 80:545–549
Stumpf PG (1985) Stenosis and fistulae with neglected vaginal foreign bodies. A case report. J Reprod Med 30:559–560
Sacco F, Benedetti-Panici P, Villani L, Bompiani A (1980) A case of vesicovaginal fistula caused by a foreign body. Minerva Ginecol 32(1–2):49–52
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Puppo, A., Naselli, A. & Centurioni, M.G. Vesicovaginal fistula caused by a vaginal foreign body in a 72-year-old woman: case report and literature review. Int Urogynecol J 20, 1387–1389 (2009). https://doi.org/10.1007/s00192-009-0877-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-009-0877-y