
Abstract
The purpose of this study was to compare the surgical outcome and attendant complications of the suprapubic arc (SPARC) sling and tension-free vaginal tape (TVT) procedures. Sixty-two women with genuine stress incontinence (GSI) alone or combined with pelvic prolapse less than International Continence Society (ICS) stage II were randomly allocated to either SPARC or TVT groups. A routine suprapubic ultrasonography was performed for all patients 1 day after the anti-incontinence operation. A comparison of the peri- and postoperative results comprising surgical outcomes and complications revealed no significant differences between the two groups. Although the difference in the rates of bladder injury was not statistically significant (SPARC 12.9 vs TVT 0.0%, p=0.112), it was clinically significant. Routine suprapubic ultrasonography revealed eight subjects had retropubic hematomas greater than 5 cm. The cure rate for SPARC was not significantly different from TVT (80.7 vs 87.1%, p=0.706). We concluded that the SPARC sling and TVT procedures proved to be equally effective. Subsequent suprapubic ultrasonography, in particular for the symptomatic patients, was found to be of clinical merit.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The tension-free vaginal tape (TVT) procedure for the treatment of genuine stress incontinence (GSI) in women was first reported in 1996 by Ulmsten et al. [1]. This procedure has been shown to be a safe and effective treatment for GSI, offering the benefits of a minimally invasive technique, with good long-term results [2].
In this newly designed continence taping procedure, TVT which is supposed to be placed under the midurethra, is introduced paraurethrally and retropubically using a 5×100-mm cone tip trocar. Those organs and tissues near the passage of the trocar are vulnerable to injury. Recently, the suprapubic arc (SPARC) sling procedure was developed to utilize the posterior surface of the symphysis as a boundary for needle passage in an effort to decrease the bowel, lower urinary tract, and vascular injury that sometimes occurs with the upward passage of the TVT trocar [3, 4, 5].
Although the mechanism of continence, a type of sling utilized in a specific manner, is similar for these two procedures, the design of the delivery system and sling mesh as well as the technique of sling positioning are different.
The objectives of this prospective randomized trial were to compare the surgical outcomes of these two continence taping procedures and to determine whether a finer and downward pass SPARC needle caused less iatrogenic injury.
Materials and methods
Women were eligible for the trial if they had GSI alone or combined with pelvic prolapse. Exclusion criteria were pelvic prolapse greater than stage II of the International Continence Society (ICS) grading system [6] or previous anti-incontinence surgery. The devices used were manufactured either by Gynecare, a division of Ethicon (Somerville, N.J., USA) (TVT) or American Medical Systems (Minnetonka, Minn., USA) (SPARC). Urodynamic studies including free flowmetry urethral pressure profilometry, filling (provocative) and voiding cystometry, and a 1-h pad test were performed preoperatively and 2 years after the operation [7]. Institutional Review Board approval was obtained.
Sample size calculation and randomization
Since one of the objectives of this study was to determine the difference in the iatrogenic injury rate between these two procedures, the cystotomy rate was used to calculate the sample size required. Two (20%) bladder perforations occurred in a pilot study of ten SPARC procedures conducted in our unit before the present study. In contrast, the perforation rate for the TVT procedure was only 0.8% in a series of 600 cases [4]. To detect a 19.2% (20–0.8) difference in rate based on the information indicated above, we conducted a test with a significance level of 0.05 and power of 0.8 and anticipated that groups of equal size would be required. At least 28 subjects in each group were required to test the hypothesis.
During outpatient consultation, women were informed of the study and asked to participate. By using a predetermined computer-generated randomization code, those subjects who acquiesced and satisfied the inclusion criteria were assigned randomly by the authors (except LHT) to the SPARC or TVT procedure at the outpatient clinic. The patients were blinded to the procedure, but the principle based on the integral theory was briefly explained to them.
Surgical treatment and postoperative management
Under either regional or local anesthesia with sedation, TVT was performed as described by Ulmsten [1] and SPARC as by Plzak and Staskin [3]. Anterior colporrhaphy with or without posterior colporrhaphy was simultaneously performed for those women with symptomatic vaginal prolapse. Vaginal total hysterectomy with or without sacrospinous ligament fixation was performed for those with pelvic prolapse greater than ICS stage II. The senior author (ACW) performed all of the procedures for these 62 patients. All patients underwent a routine suprapubic ultrasonography for detecting unrecognized subcutaneous or retropubic hematoma on the day immediately after the operation. The examination was performed with no limitation of bladder volume, using a 3.5-MHz linear array transducer (Aloka SSD 1200, Aloka, Tokyo, Japan). The ultrasonographer was blinded to the procedure used for GSI.
In general, no catheterization for urine was instituted postoperatively except in those patients for whom a concurrent vaginal repair was undertaken. In these patients usually the catheters were removed on the 3rd postoperative day. Sterile, intermittent catheterization was offered every 4 h for women without an indwelling catheter when they left the operating room. The patient was discharged from the hospital once the amount of postvoid residuals was less than 20% of that from self-voiding consecutively four times. Follow-up visits were scheduled each at 1 month, 6 months, and 12 months and then annually after hospital discharge. Follow-up ranged from 24 to 30 months (median: 25 months). A 4-day, 24-h voiding diary (for urinary symptomatic outcome only) was recorded by the patient before the last follow-up visit. Objective cure was defined as pad weight 1 g or less; patients whose loss decreased to less than half of the preoperative value were considered improved.
Nomenclature
Defective vaginal wound healing was defined as presentation of granulation background on the site of the polypropylene tape implantation in the anterior vaginal wall. Rejection of tape was considered as including persistent defective healing of the vaginal wound despite debridement, exposure of the suburethral portion of the tape, spontaneous healing of the vaginal wound after removal of the exposed tape, and evidence of prosthesis-rejection reaction demonstrated by immunohistochemical evaluation (data will be reported in another article). Protrusion of the tape edge was defined as healing of the vaginal wound without any visible granulation background, with part of the unbound selvage edge of the tape being visible on the suburethral implantation site. All terminology conform to that established by the ICS unless specifically noted [8].
Statistical analyses
Data was analyzed using Statistical Package for the Social Sciences (version 10.0) and presented as either mean±SD or frequency (percentage). A general level of p<0.05 was considered significant in this study. The difference between the SPARC and TVT groups, in peri- and postoperative results including surgical outcomes was compared using the two-sample t-test, Mann-Whitney test, chi-square test, Fisher’s exact test, or paired t-test. Wilcoxon’s signed rank test was used to compare the difference in the urodynamic evaluation.
Results
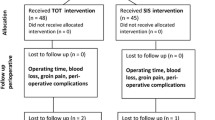
Between October 2001 and April 2002, 62 of 72 consecutive women who had GSI with or without pelvic prolapse were randomized to receive either the SPARC sling or TVT procedures. Of the 72 women, 10 (13.9%) were excluded before randomization including 5 who had previous anti-incontinence surgery and 5 who had pelvic prolapse of greater than ICS stage II. The remaining 62, aged 51±11.73 years and parity 3 (range: 0–7), were evenly distributed to either the SPARC or TVT groups. All of the patients completed follow-up. Thus, our study was based on the analysis of data from the 62 subjects, obtained preoperatively and at the 2-year follow-up visit. An independent nurse continence adviser (YTK) who was blinded to the procedures conducted all of the follow-up examinations. The author (LHT) who assessed the outcomes was blinded to the procedures and all examinations.
A comparison of the demographic characteristics revealed no significant differences between the SPARC and TVT groups: age (50.43±11.15 vs 51.57±12.45, p=0.712), parity (3.0±3.0 vs 4±2, p=0.2006), and menopausal women [22 (70.9%) vs 23 (74.2%), p=0.808]. For both the TVT and SPARC groups, the differences between pre- and postoperative pad tests were statistically significant (33.6±31.8 vs 9.0±22.3, paired t-test, p<0.001 and 35.1±31.2 vs 7.2±22.1, paired t-test, p<0.001, respectively). The postoperative pad test for the two groups was not significantly different (9.0±22.3 vs 7.2±22.1, paired t-test, p=0.12). According to the described criteria for objective surgical outcome, the success rates each for the TVT and SPARC procedures were accordingly registered as 87.1 cured vs 12.9% improved and 80.7 cured vs 19.3% improved, respectively.
Table 1 compares the peri- and postoperative clinical results including various urinary symptoms registered in the voiding diary and the complications, revealing no statistically significant differences between the two groups. Seven (22.6%) of the 31 women in the TVT group and 5 (16.1%) of the other 31 in the SPARC group underwent simultaneous repair of vaginal prolapse (p=0.748, Fisher’s exact test). Table 2 compares the postoperative urodynamic results of the two procedures. All variables revealed no statistically significant difference. The preoperative urodynamic evaluation of the two groups did not reveal a statistically significant difference in any variable listed in Table 2.
Of the eight women who had retropubic hematoma(s) larger than 5 cm, seven were discharged uneventfully from the hospital within 7 days after the operation. Ultrasonography performed at the 1-month follow-up visit revealed complete resolution of the hematoma for every patient. No retropubic hematoma larger than 5 cm occurred simultaneously with bladder perforation and no subcutaneous hematoma was incurred in this study.
The patient who had a 9-cm retropubic hematoma (Fig. 1) had been on aspirin for years due to a heart condition. Although aspirin was discontinued 16 h before the TVT procedure, and platelet count as well as bleeding time were normal, 300 ml of intraoperative blood loss and postoperative suprapubic wound ecchymosis were experienced. A ruptured blood vessel (a branch of the left obturator artery) was noted while laparotomy was performed to evacuate the retropubic hematoma. A Penrose drain was inserted subsequently in the space for postoperative drainage. The patient was discharged uneventfully from the hospital 7 days after the initial operation (TVT). She complained of wound pain and urge incontinence during follow-up, but these complaints were resolved at the 6-month follow-up visit.

A retropubic hematoma measuring 9.0×8.9 cm, originating in the TVT procedure
Discussion
Although the difference in incidence was not statistically different, the most striking finding in this study was that the incidence of bladder injury by the SPARC needle was even higher than that caused by the TVT trocar (Fig. 2). In contrast to a 700-case experience with the TVT procedure, these 31 cases comprised the present author’s (ACW) first experience with the SPARC procedure. Therefore, the experience level may have biased the present study. Compared to the trocar of the TVT device, the SPARC needle is finer (3 vs 5 mm); thus, the incidence of bladder injury should theoretically be lower. A plausible reason for the nonetheless higher perforation rate was that the SPARC needle, being finer, curved and longer (3×220 mm), was therefore difficult to handle when passed downward. Moreover, a small cephalad deviation at the point of insertion will lead to a magnified deviation and injury of the bladder. The treatment of bladder injury caused by the SPARC needle was straightforward. The surgeon simply inserted a 16 F Foley catheter transurethrally and drained the bladder continuously for 48 h. For those patients who had bladder injury in this study, the SPARC sling procedure proceeded as originally scheduled.

Bladder perforation by a SPARC needle
To the authors’ knowledge, this is the first report in the English literature of suprapubic ultrasonography performed routinely after continence taping procedures for detecting any concealed hematoma incurred. The technique is noninvasive, without any radiation hazard, and easy to apply. It is valuable to detect those subcutaneous or retropubic hematoma which were often not otherwise recognized by the surgeon. However, seven of eight women with retropubic hematoma larger than 5 cm were asymptomatic and it was resolved spontaneously 1 month after the operation. Thus, in view of the cost effectiveness aspect of medical economics, it seems just as clinically useful to perform the examination only in symptomatic subjects.
The recovery (healing) of the anterior vaginal wall is intriguing. The author has been observing for years the healing process of the wound of the anterior vaginal wall in which the polypropylene tape was implanted. As mentioned earlier in this communication, three different abnormal findings on the anterior vaginal wall were seen at the follow-up visits. We suspected that a certain percentage of our patients had a prosthesis-rejection reaction after implantation because the defectively healing vaginal wound healed automatically after removal of the suburethral portion of the tape. In addition, the histological and immunohistochemical analysis of the wound biopsies suggested evidence of immunologic reaction of the implanted tape to the vaginal tissue [9].
Ideal design of the device is closely related to the performance (manipulation) and efficacy of the procedure. The mechanism to achieve continence is basically similar in the two different procedures and this is reflected in the postoperative urodynamic evaluation of the two groups. However, both design of the device and approach to trocar (needle) insertion are different. As most urological surgeons are familiar with the downward pass needle and they need to maintain the tip of the needle in a position directly behind the pubic bone, the SPARC needle is manufactured with a fine tip and long, curved shaft. However, one author (ACW) found it difficult to hold steady during insertion, either connected to its handle or not. Furthermore, because the shaft of the needle is thinner, the SPARC procedure was expected to cause less blood loss. However, because the size of the dilating connector attaching the mesh sling to the SPARC needle is relatively large, the paraurethral dissection had to be wider to allow the passage of the dilating connector. This may have led to increased blood loss. In addition to a thinner shaft, the SPARC needle being reflective and silver in color cannot be easily detected under water when it perforates the bladder, particularly when the cystoscopic light shines within the bladder. On the other hand, an advantage of SPARC mesh is the unique design of the tensioning suture which can facilitate either reducing or increasing the tension after sling (mesh) positioning. In regard to the TVT device, with a blind upward pass of the trocar behind the pubic bone, awareness of the trocar tip may be lost. The technical problems regarding the TVT procedure have been reported elsewhere in the literature [4].
The objective surgical outcomes and various complications of the SPARC sling and TVT procedures were not significantly different in this study with a short follow-up period. Therefore, further study including a larger number of subjects and a longer period of follow-up is warranted.
Conclusions
Based on the comparison of objective outcome measurements as well as various peri- and postoperative results, the SPARC sling and TVT procedures are equally effective in the treatment of GSI. The rates of various complications including bladder injury were not significantly different between the two groups although the cystotomy rate was higher in the SPARC group. This study also proved that a routine suprapubic ultrasonography performed 1 day after the continence taping procedures, particularly for the symptomatic patient, is of clinical merit.
References
Ulmsten U, Petros P (1995) Intravaginal sling plasty: an ambulatory surgical procedure for treatment of female urinary incontinence. Scand J Urol Nephrol 29:75–82
Nilsson CG, Kuuva N, Falconer C et al (2001) Long-term results of the tension-free vaginal tape (TVT) for surgical treatment of female stress urinary incontinence. Int Urogynecol J 12 [Suppl 2]:S5–S8
Plzak L, Staskin DR (2002) Midurethral slings work—but why? Quarterly newsletter on incontinence diagnosis, treatment and care. Spring, pp 4–8
Wang AC (2004) The technique of trocar insertion and intraoperative urethrocystoscopy in tension-free vaginal taping—an experience of 600 cases. Acta Obstet Gynecol Scand 83:293–298
Zilbert AW, Farrell SA (2001) External iliac artery laceration during tension-free vaginal tape procedure. Int Urogynecol J 12:141–143
Bump RC, Mattiasson A, Bo K et al (1996) The standardization of terminology of female pelvic floor dysfunction. Am J Obstet Gynecol 175:10–17
Wang AC, Chen MC (2003) The correlation between preoperative voiding mechanism and surgical outcome of the tension-free vaginal tape procedure, with reference to quality of life. BJU Int 91:502–506
Bates P, Bradly WE, Glen E et al (1979) The standardization of terminology of lower urinary tract function. J Urol 121:551–554
Wang AC, Lee LU, Lin CT (2004) A histological and immunohistochemical analysis of defective vaginal healing after continence taping procedures. A prospective case-controlled pilot study. Am J Obstet Gynecol, in print
Author information
Authors and Affiliations
Corresponding author
Additional information
This manuscript had no conflicts of interest with any commercial association
Rights and permissions
About this article
Cite this article
Tseng, LH., Wang, A.C., Lin, YH. et al. Randomized comparison of the suprapubic arc sling procedure vs tension-free vaginal taping for stress incontinent women. Int Urogynecol J 16, 230–235 (2005). https://doi.org/10.1007/s00192-004-1248-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-004-1248-3