
Abstract
Purpose
The aim of this study was to investigate the clinical and radiological results of the MAKO CT-based robotic-assisted system for total knee arthroplasty (TKA).
Methods
A PRISMA systematic review was conducted using four databases (MEDLINE, EMBASE, Pubmed, GOOGLE SCHOLAR) to identify all clinical and radiological studies reporting information regarding the use and results of the CT-based robotic-assisted system to perform TKA between 2016 and 2020. The main investigated outcome criteria were postoperative pain, analgesia requirements, clinical scores, knee range of motion, implant positioning and the revision rate. The ROBINS-I tool (Risk Of Bias In Non-randomized Studies of Interventions) was used to evaluate the quality of included studies and the risk of bias.
Results
A total of 36 studies were identified, of which 26 met inclusion criteria. Of these 26 studies, 14 were comparative. The follow-up varied from 30 days to 17 months. This CT-based, saw cutting Robotic TKA is associated with a significantly lower postoperative pain score (2.6 versus 4.5) and with significantly reduced time to hospital discharge (77 h versus 105), compared with conventional TKA. The two comparative studies assessing functional outcomes at 1 year reported significantly better functional scores with CT-based robotic TKA compared with conventional TKA (WOMAC score: 6 ± 6 versus 9 ± 8 (p < 0.05); KSS function score: 80 versus 73 (p = 0.005)). Only three comparative studies assessed implant positioning, and these reported better implant positioning with CT-based robotic-assisted TKA.
Conclusion
The CT-based robotic-assisted system for TKA reduced postoperative pain and improved implant positioning with equal or slightly superior improvement of the functional outcomes at one year, compared to conventional TKA.
Level of evidence
Systematic review level IV.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) is an effective surgery providing pain relief and improved quality of life. However, patient satisfaction following TKA ranges from just 75 to 89% using different patient-reported clinical outcome measures [2, 7, 38]. Up to 6% of patients who undergo a primary TKA may require a revision within 5 years from the index procedure according to a large meta-analysis from worldwide arthroplasty registries on 689,608 primary surgeries [21]. Different approaches have been considered to improve TKA clinical and radiological outcomes, such as the use of computer-assisted surgery with navigation, image based and image-less robotic system assistance [1, 51], accelerometer or other sensor use [34, 50], and different surgical alignment techniques [12, 26].
The current motivations behind robotic-assisted TKA are improved surgical implant positioning, alignment accuracy, advancing articular surface design that allows for independent intercompartmental resurfacing, optimizing component positioning based on normal soft tissue balancing and tension, and ultimately improving patient clinical and functional outcomes. Several systematic reviews reported the clinical and radiological outcomes of robotic-assisted TKA in general, including different types of robotic-assisted systems [1, 8, 39, 41]. They reported satisfying outcomes, particularly an improvement in implant positioning with robotic-assisted systems compared with a conventional technique. The various robotic-assisted systems are quite different (image-based, image-free, different cut systems, different methods for planning) and therefore, are not equivalent. During this early phase of robotic-assisted surgery development, it is important to distinguish the differences between each system and to assess them independently. The CT-based robotic-assisted system (MAKO system) adapted for TKA has been available since 2016. There is no systematic review summarizing the main results of this specific CT-based robotic arm system, such as implant position, knee alignment accuracy, clinical and functional advantages and disadvantages. CT-based arm-assisted robotic technology might be a valuable tool that can reduce surgical complications and decrease the risk of implant failure. But a focused assessment is necessary to improve individual practice.
The aim of this systematic review was to summarize all the relevant surgical and clinical results of the MAKO CT-based robotic arm-assisted system for TKA.
Materials and methods
Article identification and selection process
A search in August 2020 was performed to identify all available literature that described the results of TKA performed with the image-based robotic-assisted system. The search was performed through PubMed, EMBASE, MEDLINE, GOOGLE SCHOLAR, and the COCHRANE LIBRARY databases from 2016 to 2020 inclusive, using the 2009 Preferred Reporting Items for Systematic Reviews and Meta-Analyses protocol (PRISMA).
Inclusion criteria for the search strategy included all English and French language studies reporting information regarding the use and results of the image-based robotic-assisted system to perform TKA. The types of included articles were randomized controlled studies, cohort studies, case-controlled studies, and cadaveric studies. The following terms were used: “total knee arthroplasty” or “total knee replacement”; “MAKO” or “image-based robotic-assisted” or “robotic-arm assisted”. Exclusion criteria consisted of (1) editorial articles, (2) systematic reviews or meta-analyses, (3) case reports, (4) articles on revision unicompartmental knee arthroplasty (UKA), and (5) articles evaluating joints other than the knee. The abstracts from all identified articles were independently reviewed by two investigators. Articles were excluded on the basis of the title and abstract if they did not assess TKA performed by the image-based robotic-assisted system (MAKO system). Full-text articles were obtained for review to allow further assessment of inclusion and exclusion criteria where necessary.
Additionally, all references from the included studies were reviewed and reconciled to verify that no relevant articles were missing from this systematic review that met inclusion criteria.
The main investigated outcome criteria were postoperative pain and analgesia requirements during the hospitalization, the short-term clinical scores and knee range of motion, implant positioning, and the short-term revision and complication rates.
Quality assessment
The ROBINS-I tool (Risk Of Bias In Non-Randomized Studies of Interventions) [48] was used to evaluate the quality of the included studies and their relative risk of bias (Table 1). This included bias due to confounding, selection of participants classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of reported result. The categories for risk of bias judgements are “Low risk”, “Moderate risk”, “Serious risk” and “Critical risk”. The worst judgement bias assigned within any one domain gives the judgement score of the complete study.
Results
Included articles and study characteristics
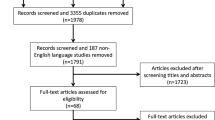
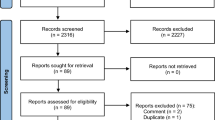
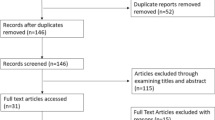
The PRISMA flow diagram for study selection is shown in Fig. 1. A total of 36 potential full-text articles were identified by the search strategy. Of the 36 articles, 4 were excluded as not relevant, 6 were excluded, because they were reviews and three were case reports. Of these, 1 study presented a low risk of bias according to the ROBINS-I [48], 17 studies presented a moderate risk (Table 1). The reported follow-up periods ranged from a minimum of 30 days to a maximum of 17 months. Fourteen studies were controlled with a TKA group performed by image-based robotic-assisted system and a TKA group performed by conventional technique (Table 2).

Flowchart from the initial literature search through to data extraction from the final list of included studies
Functional outcomes
The majority of the controlled studies assessed early functional outcomes after TKA performed with the image-based robotic-assisted system (Table 3). Marchand et al., in a comparative study of 20 consecutive robotic arm-assisted TKAs, described a lower mean pain score at 6 months in the robotic group (p < 0.05) [32]. This difference in pain score is not significant at 1 year [30]. In a prospective comparative study, robotic arm-assisted TKA was associated with reduced postoperative pain (3.6 in the robotic group versus 6.3), decreased analgesia requirements during initial hospitalization, and also decreased length of stay in hospital (mean 77 h in robotic group versus 105 h in the conventional group) compared with conventional jig-based TKA (p < 0.001) [18]. Other studies reported similar short-term results (low pain scores, low opioid usage, shorter length of stay) [5, 37].
Some authors described better satisfaction after robotic-assisted TKA compared with conventional TKA in the short term [32, 44], whereas other studies did not report a significant difference [20].
Several case-controlled studies assessed the short-term functional postoperative scores, with a maximum follow-up of 17 months, between robotic-assisted and conventional TKA, with inconclusive results [20, 30, 37, 44].
The mean knee flexion at discharge was also higher in the robotic group (104.1°) compared to the conventional group (93.3°) (p < 0.001) [18]. The mean knee flexion at 90 postoperative days appears superior in the robotic group, with a better improvement compared to preoperative flexion [37].
Accuracy of implant positioning
Two comparative studies assessed implant positioning. Robotic arm-assisted TKA improved accuracy in achieving the planned implant position compared to conventional jig-based TKA (Table 4) [16, 49]. Kayani et al. demonstrated that the robotic-assisted system improved the accuracy of femoral coronal and sagittal alignment, tibial coronal and sagittal alignment, joint line restoration, tibial slope and limb alignment, compared to a conventional technique [16]. Sires et al. performed postoperative CT scans to assess the accuracy of the CT-based robotic-assisted TKA [43]. They reported that 93% of the reported intraoperative measurements were ≤ 3 degrees of the postoperative CT measurements. The results were also similar for coronal limb alignment.
Complications and implant survivorship
The rate of early complications was not significantly different between robotic-assisted TKA and conventional TKA [11, 18] (Table 5). The main short-term complication reported was manipulation under anesthesia, without a difference between robotic-assisted and conventional TKA [11, 37, 44]. Malkan et al. found less manipulation under anesthesia in the group of robotic-assisted TKA compared than conventional TKA [27]. Kayani et al. reported a minor wound dehiscence over the incision for the proximal tibial registration pins [18]. There were no other specific complications of the image-based robotic-assisted system. Short-term revisions were rare and the majority of the studies did not report revisions after robotic-assisted TKA [11]. Malkani et al. reported 4 revisions on 188 patients: 2 aseptic revisions (for unexplained pains and tibial fracture) and 2 septic revisions [28]. No study found a higher rate of infection after robotic-assisted TKA compared than conventional TKA.
Soft tissue and bone preservation
In a comparative study, Kayani et al. reported that robotic-assisted TKA was associated with reduced bone and periarticular soft tissue injury compared with conventional TKA, without assessment of the clinical outcomes [17]. With a new score that classified bone and soft tissue injuries (MASTI classification system), they demonstrated superior accuracy of the robotic-assisted system during knee preparation. In a cadaver study, Hampp et al. then Khlopas et al. showed that less soft-tissue damage occurs utilizing robotic-assisted TKA, particularly regarding the posterior cruciate ligament [14, 19].
The learning curve for robotic TKA
Kayani et al. described an improvement of the operative time of robotic arm-assisted TKA (89.2 vs. 66.8 min, p = 0.01) and of the surgical team stress levels after seven robotic cases [16]. But there was no learning curve effect of robotic arm-assisted TKA on accuracy of achieving the planned implant position and limb alignment. In a comparative study of 240 robotic-assisted TKAs, a significant difference was found in mean operative times for the first robotic-assisted cohort and the conventional cohort (81 vs. 68 min, p < 0.05) [45]. However, no significant differences in mean operative times were found between the last robotic-assisted cohort and the conventional cohort (70 vs. 68 min, p > 0.05).
Cost
Cool et al. showed that robotic-assisted TKA patients had statistically significantly lower 90-day episode-of-care (EOC) costs [10]. A study of Medicare Fee-For-Service (FFS) members, that included 519 CT-based robotic-assisted TKAs, assessed the utilization and payer costs for postoperative services [36]. It reported that the robotic-assisted TKA versus conventional TKA cohort average total episode payment was US $17,768 versus US$19,899 (p < 0.0001) at 30 days, US$18,174 versus US$20,492 (p < 0.0001) at 60 days, and US$18,568 versus US$20,960 (p < 0.0001) at 90 days. There was a trend towards increased operative time in robotic arm-assisted TKA, but overall time to hospital discharge was reduced in the robotic group (p < 0.001) [18].
Recently, Cotter et al. performed an interesting study associating intraoperative costs and inpatient costs in a comparative study [11]. Total intraoperative costs were higher ($10,295 vs. $9998, respectively, p < 0.001) and inpatient costs were lower ($3893 vs. $5587, respectively, p < 0.001) comparing robotic-assisted TKA and conventional TKA. Length of stay was reduced by 25% (p < 0.0001) and prescribed opioids were reduced by 57% (p < 0.0001) comparing robotic-assisted TKA and conventional TKA. Ninety-day EOC costs were $2,090 lower for robotic-assisted TKA (p < 0.001).
Discussion
The key findings of this systematic review are:
-
1.
reduction of postoperative pain and decreased analgesia requirements during the hospitalization with the robotic-assisted system;
-
2.
more accurate and reproducible implant positioning with robotic-assisted TKA;
-
3.
similar risk of short-term complications or revision for robotic-assisted TKA and conventional TKA [17];
-
4.
lower 90-day EOC costs with robotic-assisted TKA.
Functional outcomes
Several studies suggested that the implementation of robotic arm-assisted surgery may help to further improve early functional recovery and reduce time to hospital discharge in patients undergoing TKA [18, 30, 44]. However, at 6 months and at 1 year, the functional results are similar for both surgical techniques in several studies [20, 37].
Operative and cadaveric studies assessed the soft tissue injuries in robotic-assisted TKA and in conventional TKA, with less damage in robotic TKA. This system allowed better soft tissue protection around the knee and facilitated knee exposure [14, 17, 19]. It would be interesting to assess the clinical outcomes after TKA according to the soft tissue injury. The learning curve and improvement in surgical time was short (only seven cases to improve the surgical time by 22 min) [16]). Longer surgical times did not negatively impact upon postoperative outcomes, because there was no significant difference in functional outcomes between groups of longer and shorter operating durations. The difference in functional outcomes disappeared over time. Currently, at mid-term, the use of the robotic-assisted system is at least equivalent to the conventional technique for functional outcomes, but not superior. This lack of significant difference at mid-term between robotic-assisted TKA and conventional TKA is also reported with other robotic-assisted systems such as ROBODOC [22, 23], or for other surgeries such as unicompartmental knee arthroplasty (UKA) [3].
Complications and revisions
This review of image-based robotic-assisted TKA did not find any specific complications for the robotic-assisted system. The complication and revision rates were low in both robotic-assisted and in conventional technique cohorts at short-term follow-up. Other studies of the robotic-assisted system for knee replacements found some specific complications of this system, such as infection or fracture at the pin insertion site or pin breakage [25, 52]. In 2014, Hansen et al. [15] and Blyth et al. [6] did not find complications related to the MAKO system in UKA cohorts. In the literature, possible complications indirectly related to the use of a robotic-assisted system, such as stiffness or infection, were comparable between robotic and conventional groups [25, 35]. In contrast to robotic-assisted UKA in the Australian Orthopaedic Association National Joint Arthroplasty Registry, the studies about CT-based robotic-assisted TKA did not find higher rates of infection in the robotic group [47].
To assess revision rates according to the use of a robotic-assisted system, a long-term study is needed. Indeed, most revisions occur in the mid- to long-term, and rarely in the short-term, even for surgical mistakes. The robotic-assisted system for UKA was effective in decreasing revision rates, but UKA is a technically demanding surgery with a higher risk of revision compared with TKA.
Implant positioning
A few studies assessed implant positioning after robotic-assisted TKA with the MAKO system. All these studies demonstrated the efficacy of robotic-assisted TKA in restoring the mechanical axis alignment in fairly common clinical scenarios where mild deformity was successfully corrected. The technique was also more accurate than the conventional method in restoring mechanical alignment and decreasing the number of outliers. No learning curve has been identified for accuracy of implant positioning or limb alignment [16]. An image-based robotic-assisted system allows for good accuracy, even without system experience. This robotic-assisted system is based on a CT scan, with the preoperative planning being very accurate [43]. If the preoperative planning is not appropriate, it is likely due to poor surgical planning. The robotic-assisted system is ultimately a tool to improve surgical accuracy [13, 16, 43, 49]. Other robotic-assisted systems have reported similar results. In one randomized controlled study, the authors found no statistical difference in the absolute mechanical axis, but did obtain significant differences in the rate of outliers between the robotic-assisted group (ROBODOC) (0%) and the conventional group (19.4%) (p = 0.049) [22]. Furthermore, Song et al. performed a randomized study of 100 patients and found no outliers in the robotic-assisted group compared with 24% in the conventional group [46].
Several robotic systems have also demonstrated improved accuracy of implant positioning in UKA, such as the Acrobot [9], the Navio [3, 40] and the MAKO systems [4, 24]. These robotic-assisted systems can be more accurate for several reasons: more accurate preoperative planning, particularly for image-based robotic-assisted systems and a robotic arm which improves the precision of the surgeon. It would be interesting to compare implant positioning between different types of robotic-assisted systems to assess the effect on accuracy of the use of image-based and image-free robotic-assisted systems, a robotic arm or burr and a conventional computer navigation system.
Cost
The evaluation of the robotic-assisted system cost must take into account the system cost, the cost of the hospitalization and the cost of complications and surgical revisions. Cool et al. and Mont et al. reported that robotic-assisted TKA patients had statistically significantly lower 90-day EOC costs [10, 36]. Nevertheless, several parameters should also consider the cost of the robotic-assisted system, the cost of the consumable products for each surgery, and the cost of mid-term or long-term complications and revisions. Recently, Cotter et al. performed a comparative study about the intraoperative and inpatient costs for robotic-assisted TKA compared with conventional TKA [11]. They described that 90-day EOC costs were $2,090 lower for robotic-assisted TKA compared with conventional TKA. Nevertheless, some parameters were not considered in this study (for example, the reimbursement system), so it is difficult to make conclusions about the robotic-assisted system’s cost.
Our findings should be considered with an understanding of the key limitations of the data set. First, the inclusion criteria, such as English language or the requirement of full text access, may have excluded relevant studies. Second, the methodology score has known limitations with regard to the type of studies included (cohort and cadaveric studies) and the difficulties in assessing the validity of the analyses conducted without having access to the raw data. Third, there was an important variability between the studies with respect to the type of outcome measurement parameters used, the follow-up period, the patient population and cohorts evaluated, and the analyses performed. This heterogeneity limits the possibility of performing a true meta-analysis of the results. Moreover, there are not yet any published randomized controlled trials. These randomized studies are currently in progress. The studies on robotic arm-assisted TKA with the MAKO image-based robotic-assisted system are few in number and mainly have short-term follow-up (< 2 years). Furthermore, the follow-up period for these studies remains short, principally because this system is so new. Future studies with longer term follow-up will be more conclusive in assessing the outcomes and benefits. Furthermore, this systematic review was only about one robotic-assisted system. There are a lot of studies reporting the results of TKA using various robotic-assisted systems with interesting results. Nevertheless, the aim of this study was to target this particular robotic-assisted system. Indeed, all robotic-assisted systems are not equivalent and use different planning data (CT-based, image-free). It is important to assess each specific system.
The main strength of this study, compared to previous systematic reviews, was the assessment of only one image-based robotic-assisted system for TKA. The aim was to assess all knowledge about this specific system to improve our understanding of the positives and negative aspects. There are no studies specifically evaluating each robotic-assisted system. Distinguishing between these different systems remains important, as surgeons use a specific system and need expertise in that particular system.
Conclusion
Robotic-assisted TKA demonstrated satisfying short-term clinical and radiological outcomes. The postoperative outcomes during hospitalization were equal or slightly superior for the robotic-assisted group compared to conventional TKA, without significant differences in clinical and functional results at short and mid-term. Current evidence shows advantages of image-based robotic-assisted TKA in mechanical knee alignment, implant positioning, ligamentous balance and soft tissue protection. However, powerful studies at longer term follow-up are critical to assess the long-term advantages of this robotic system, particularly for TKA survivorship or potential benefits of alternate alignment philosophies.
References
Agarwal N, To K, McDonnell S, Khan W (2020) Clinical and radiological outcomes in robotic-assisted total knee arthroplasty: a systematic review and meta-analysis. J Arthroplasty. https://doi.org/10.1016/j.arth.2020.03.005
Barrack RL, Engh G, Rorabeck C, Sawhney J, Woolfrey M (2000) Patient satisfaction and outcome after septic versus aseptic revision total knee arthroplasty. J Arthroplasty 15:990–993
Batailler C, White N, Ranaldi FM, Neyret P, Servien E, Lustig S (2019) Improved implant position and lower revision rate with robotic-assisted unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 27:1232–1240
Bell SW, Anthony I, Jones B, MacLean A, Rowe P, Blyth M (2016) Improved accuracy of component positioning with robotic-assisted unicompartmental knee arthroplasty: data from a prospective, randomized controlled study. J Bone Joint Surg Am 98:627–635
Bhimani S, Bhimani R, Smith A, Eccles C, Smith L, Malkani A (2020) Robotic-assisted total knee arthroplasty demonstrates decreased postoperative pain and opioid usage compared to conventional total knee arthroplasty. Bone Joint Open 1–2:8–12
Blyth MJG, Anthony I, Rowe P, Banger MS, MacLean A, Jones B (2017) Robotic arm-assisted versus conventional unicompartmental knee arthroplasty: exploratory secondary analysis of a randomised controlled trial. Bone Joint Res 6:631–639
Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD (2010) Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res 468:57–63
Chin BZ, Tan SSH, Chua KCX, Budiono GR, Syn NL, O'Neill GK (2020) Robot-assisted versus conventional total and unicompartmental knee arthroplasty: a meta-analysis of radiological and functional outcomes. J Knee Surg. https://doi.org/10.1055/s-0040-1701440
Cobb J, Henckel J, Gomes P, Harris S, Jakopec M, Rodriguez F et al (2006) Hands-on robotic unicompartmental knee replacement: a prospective, randomised controlled study of the acrobot system. J Bone Joint Surg Br 88:188–197
Cool CL, Jacofsky DJ, Seeger KA, Sodhi N, Mont MA (2019) A 90-day episode-of-care cost analysis of robotic-arm assisted total knee arthroplasty. J Comp Eff Res 8:327–336
Cotter EJ, Wang J, Illgen RL (2020) Comparative cost analysis of robotic-assisted and jig-based manual primary total knee arthroplasty. J Knee Surg. https://doi.org/10.1055/s-0040-1713895
Courtney PM, Lee GC (2017) Early outcomes of kinematic alignment in primary total knee arthroplasty: a meta-analysis of the literature. J Arthroplasty 32:2028–2032
Hampp EL, Chughtai M, Scholl LY, Sodhi N, Bhowmik-Stoker M, Jacofsky DJ et al (2019) Robotic-arm assisted total knee arthroplasty demonstrated greater accuracy and precision to plan compared with manual techniques. J Knee Surg 32:239–250
Hampp EL, Sodhi N, Scholl L, Deren ME, Yenna Z, Westrich G et al (2019) Less iatrogenic soft-tissue damage utilizing robotic-assisted total knee arthroplasty when compared with a manual approach: A blinded assessment. Bone Joint Res 8:495–501
Hansen DC, Kusuma SK, Palmer RM, Harris KB (2014) Robotic guidance does not improve component position or short-term outcome in medial unicompartmental knee arthroplasty. J Arthroplasty 29:1784–1789
Kayani B, Konan S, Huq SS, Tahmassebi J, Haddad FS (2019) Robotic-arm assisted total knee arthroplasty has a learning curve of seven cases for integration into the surgical workflow but no learning curve effect for accuracy of implant positioning. Knee Surg Sports Traumatol Arthrosc 27:1132–1141
Kayani B, Konan S, Pietrzak JRT, Haddad FS (2018) Iatrogenic bone and soft tissue trauma in robotic-arm assisted total knee arthroplasty compared with conventional jig-based total knee arthroplasty: a prospective cohort study and validation of a new classification system. J Arthroplasty 33:2496–2501
Kayani B, Konan S, Tahmassebi J, Pietrzak JRT, Haddad FS (2018) Robotic-arm assisted total knee arthroplasty is associated with improved early functional recovery and reduced time to hospital discharge compared with conventional jig-based total knee arthroplasty: a prospective cohort study. Bone Joint J 100-B:930–937
Khlopas A, Chughtai M, Hampp EL, Scholl LY, Prieto M, Chang TC et al (2017) Robotic-arm assisted total knee arthroplasty demonstrated soft tissue protection. Surg Technol Int 30:441–446
Khlopas A, Sodhi N, Hozack WJ, Chen AF, Mahoney OM, Kinsey T et al (2019) Patient-reported functional and satisfaction outcomes after robotic-arm-assisted total knee arthroplasty: early results of a prospective multicenter investigation. J Knee Surg. https://doi.org/10.1055/s-0039-1684014
Labek G, Thaler M, Janda W, Agreiter M, Stockl B (2011) Revision rates after total joint replacement: cumulative results from worldwide joint register datasets. J Bone Joint Surg Br 93:293–297
Liow MH, Xia Z, Wong MK, Tay KJ, Yeo SJ, Chin PL (2014) Robot-assisted total knee arthroplasty accurately restores the joint line and mechanical axis. A prospective randomised study. J Arthroplasty 29:2373–2377
Liow MHL, Goh GS, Wong MK, Chin PL, Tay DK, Yeo SJ (2017) Robotic-assisted total knee arthroplasty may lead to improvement in quality-of-life measures: a 2-year follow-up of a prospective randomized trial. Knee Surg Sports Traumatol Arthrosc 25:2942–2951
Lonner JH, John TK, Conditt MA (2010) Robotic arm-assisted UKA improves tibial component alignment: a pilot study. Clin Orthop Relat Res 468:141–146
Lonner JH, Kerr GJ (2019) Low rate of iatrogenic complications during unicompartmental knee arthroplasty with two semiautonomous robotic systems. Knee 26:745–749
Maderbacher G, Keshmiri A, Krieg B, Greimel F, Grifka J, Baier C (2019) Kinematic component alignment in total knee arthroplasty leads to better restoration of natural tibiofemoral kinematics compared to mechanic alignment. Knee Surg Sports Traumatol Arthrosc 27:1427–1433
Malkan AL, Roche MW, Kolisek FR, Gustke KA, Hozack WJ, Sodhi N et al (2020) Manipulation under anesthesia rates in technology-assisted versus conventional-instrumentation total knee arthroplasty. Surg Technol Int 36:336–340
Malkani AL, Roche MW, Kolisek FR, Gustke KA, Hozack WJ, Sodhi N et al (2020) New technology for total knee arthroplasty provides excellent patient-reported outcomes: a minimum two-year analysis. Surg Technol Int 36:276–280
Manning W, Ghosh M, Wilson I, Hide G, Longstaff L, Deehan D (2019) Improved mediolateral load distribution without adverse laxity pattern in robot-assisted knee arthroplasty compared to a standard manual measured resection technique. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-019-05631-y
Marchand RC, Sodhi N, Anis HK, Ehiorobo J, Newman JM, Taylor K et al (2019) One-year patient outcomes for robotic-arm-assisted versus manual total knee arthroplasty. J Knee Surg 32:1063–1068
Marchand RC, Sodhi N, Bhowmik-Stoker M, Scholl L, Condrey C, Khlopas A et al (2019) Does the robotic arm and preoperative CT planning help with 3D intraoperative total knee arthroplasty planning? J Knee Surg 32:742–749
Marchand RC, Sodhi N, Khlopas A, Sultan AA, Harwin SF, Malkani AL et al (2017) Patient satisfaction outcomes after robotic arm-assisted total knee arthroplasty: a short-term evaluation. J Knee Surg 30:849–853
Marchand RC, Sodhi N, Khlopas A, Sultan AA, Higuera CA, Stearns KL et al (2018) Coronal correction for severe deformity using robotic-assisted total knee arthroplasty. J Knee Surg 31:2–5
Matassi F, Cozzi Lepri A, Innocenti M, Zanna L, Civinini R, Innocenti M (2019) Total knee arthroplasty in patients with extra-articular deformity: restoration of mechanical alignment using accelerometer-based navigation system. J Arthroplasty 34:676–681
Mergenthaler G, Batailler C, Lording T, Servien E, Lustig S (2020) Is robotic-assisted unicompartmental knee arthroplasty a safe procedure? A case control study. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06051-z
Mont MA, Cool C, Gregory D, Coppolecchia A, Sodhi N, Jacofsky DJ (2019) Health Care Utilization and Payer Cost Analysis of Robotic Arm Assisted Total Knee Arthroplasty at 30, 60, and 90 Days. J Knee Surg. https://doi.org/10.1055/s-0039-1695741
Naziri Q, Cusson BC, Chaudhri M, Shah NV, Sastry A (2019) Making the transition from traditional to robotic-arm assisted TKA: what to expect? A single-surgeon comparative-analysis of the first-40 consecutive cases. J Orthop 16:364–368
Noble PC, Conditt MA, Cook KF, Mathis KB (2006) The John Insall Award: patient expectations affect satisfaction with total knee arthroplasty. Clin Orthop Relat Res 452:35–43
Onggo JR, Onggo JD, De Steiger R, Hau R (2020) Robotic-assisted total knee arthroplasty is comparable to conventional total knee arthroplasty: a meta-analysis and systematic review. Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-020-03512-5
Ponzio DY, Lonner JH (2016) robotic technology produces more conservative tibial resection than conventional techniques in UKA. Am J Orthop (Belle Mead NJ) 45:E465–E468
Ren Y, Cao S, Wu J, Weng X, Feng B (2019) Efficacy and reliability of active robotic-assisted total knee arthroplasty compared with conventional total knee arthroplasty: a systematic review and meta-analysis. Postgrad Med J 95:125–133
Sires JD, Craik JD, Wilson CJ (2019) Accuracy of bone resection in MAKO total knee robotic-assisted surgery. J Knee Surg. https://doi.org/10.1055/s-0039-1700570
Sires JD, Wilson CJ (2020) CT validation of intraoperative implant position and knee alignment as determined by the mako total knee arthroplasty system. J Knee Surg. https://doi.org/10.1055/s-0040-1701447
Smith AF, Eccles CJ, Bhimani SJ, Denehy KM, Bhimani RB, Smith LS et al (2019) Improved patient satisfaction following robotic-assisted total knee arthroplasty. J Knee Surg. https://doi.org/10.1055/s-0039-1700837
Sodhi N, Khlopas A, Piuzzi NS, Sultan AA, Marchand RC, Malkani AL et al (2018) The learning curve associated with robotic total knee arthroplasty. J Knee Surg 31:17–21
Song EK, Seon JK, Yim JH, Netravali NA, Bargar WL (2013) Robotic-assisted TKA reduces postoperative alignment outliers and improves gap balance compared to conventional TKA. Clin Orthop Relat Res 471:118–126
St Mart JP, de Steiger RN, Cuthbert A, Donnelly W (2020) The three-year survivorship of robotically assisted versus non-robotically assisted unicompartmental knee arthroplasty. Bone Joint J 102-B:319–328
Sterne JA, Hernan MA, Reeves BC, Savovic J, Berkman ND, Viswanathan M et al (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:i4919
Sultan AA, Samuel LT, Khlopas A, Sodhi N, Bhowmik-Stoker M, Chen A et al (2019) Robotic-arm assisted total knee arthroplasty more accurately restored the posterior condylar offset ratio and the insall-salvati index compared to the manual technique; a cohort-matched study. Surg Technol Int 34:409–413
Ueyama H, Minoda Y, Sugama R, Ohta Y, Yamamura K, Nakamura S et al (2019) An accelerometer-based portable navigation system improved prosthetic alignment after total knee arthroplasty in 3D measurements. Knee Surg Sports Traumatol Arthrosc 27:1580–1586
van der List JP, Chawla H, Joskowicz L, Pearle AD (2016) Current state of computer navigation and robotics in unicompartmental and total knee arthroplasty: a systematic review with meta-analysis. Knee Surg Sports Traumatol Arthrosc 24:3482–3495
Wysocki RW, Sheinkop MB, Virkus WW, Della Valle CJ (2008) Femoral fracture through a previous pin site after computer-assisted total knee arthroplasty. J Arthroplasty 23:462–465
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
CB: study design, data collection, literature review and manuscript writing. AF: literature review and manuscript writing. JS, ES: study design, literature review and manuscript editing. FH, FC: study design and manuscript editing. SL: study design, supervision, literature review and manuscript editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
CB, AF and JS declare that they have no conflict of interest. ES: consultant for Corin. FH: Royalties from Stryker, Smith & Nephew, MatOrtho, Corin, Springer; Paid presentations from Stryker, Smith & Nephew, MatOrtho, Zimmer; Consultant from Stryker, Smith & Nephew; Research support from Stryker, Smith & Nephew, MatOrtho, Corin, Zimmer; Orthopaedic publications editorial for Bone and Joint Surgery, Annals of Royal College of Surgeons, Hospital Medicine. FC: Consultancy fees, royalties, and fees for participation in review activities from Stryker and consultancy fees from Adler. SL: consultant for Stryker, institutional research support to Corin and Amplitude.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Batailler, C., Fernandez, A., Swan, J. et al. MAKO CT-based robotic arm-assisted system is a reliable procedure for total knee arthroplasty: a systematic review. Knee Surg Sports Traumatol Arthrosc 29, 3585–3598 (2021). https://doi.org/10.1007/s00167-020-06283-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-020-06283-z