
Abstract
Purpose
To evaluate the kinematics/kinetics of the ankle, knee, hip in the sagittal plane in adolescents with recurrent patellar dislocation in comparison to a healthy control.
Methods
Case–control study. Eighty-eight knees (67 patients) with recurrent patellar dislocation (mean age 14.8 years ± 2.8 SD) were compared to 54 healthy knees (27 individuals, 14.9 years ± 2.4 SD). Kinematics/kinetics of ankle, knee, hip, and pelvis were captured using 3D-gait analysis (VICON, 12 cameras, 200 Hz, Plug-in-Gait, two force plates). One cycle (100%) consisted of 51 data-points. The mean of six trials was computed.
Results
The loading-response increased by 0.02 s ± 0.01SE (10.8%) with dislocations (0.98% of total gait, P < 0.01). The mid-stance-phase decreased equally (P < 0.01). Dislocation decreased knee flexion during the entire gait cycle (P < 0.01), with the largest difference during mid-stance (9.0° ± 7.2 SD vs. 18.5° ± 6.7 SD). Dislocation increased plantar-flexion during loading response 4.1° ± 0.4 SE with (P < 0.01), afterward, the dorsal-extension decreased 3.2° ± 0.3 SE, (P < 0.01). Dislocation decreased hip flexion during all phases (P < 0.01). Maximal difference: 7.5° ± 0.5 SE during mid-stance. 80% of all patients developed this gait pattern.
Internal moments of the ankle increased, of the knee and hip decreased during the first part of stance.
Conclusion
Recurrent patellar dislocation decreases knee flexion during the loading-response and mid-stance phase. A decreased hip flexion and increased plantar-flexion, while adjusting internal moments, indicate a compensation mechanism.
Level of evidence
III.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Patellar dislocation is a frequent problem in adolescents [10, 18, 32]. After the first event, as many as 15–44% experience another dislocation [13, 18, 21]. In between dislocations there are intervals of full, pain-free knee function and subjective patella stabilisation of considerable duration. Nonetheless, patients tend to reduce their level of sports participation, or even fear rough terrain. This behavioural change might reflect a coping mechanism for patellar instability.
Surgically, risk factors for patella dislocation can be mitigated. Anatomical abnormalities, such as trochlear or patellar dysplasia, patella alta, can be corrected [2, 5, 9, 10, 12, 14, 15, 23]. Ligamentous insufficiency can be reconstructed [34, 39, 40, 44]. However, a patient has limited ways to adapt to the fear of recurrent patellar dislocation; by working on the imbalanced muscles or changing gait patterns. The former is typically done consciously while the latter is mostly unconsciously developed.
In a normal gait pattern, the knee flexes during the loading response and mid-stance phase to almost 30°. However, the most vulnerable point for a patella dislocation is right around this level of knee flexion, as the primary restraint of the patella switches from the MPFL to the trochlea [3, 15, 17, 20, 40]. This conflict raises the question, if patients with recurrent patellar dislocations avoid, i.e., fear, this critical range and, therefore, adapt their gait. Given this question, we conducted a case–control study with the purpose to evaluate the flexion/extension kinematics and kinetics in the sagittal plane of the ankle, knee, hip and pelvis in adolescents with recurrent patellar dislocation in comparison to a healthy control group. The hypothesis was that adolescents with recurrent patellar dislocations decrease their knee flexion, notably during the critical phase of weight take over in comparison to a control group.
So far, research was focused on different clinical aspects rather than on the dynamic function. To our knowledge, patients with patellar instability have never been investigated in terms of how their gait is affected.
Materials and methods
The responsible IRB (University of Basel, No. 2013/104) approved the study protocol.
This study was conducted at a tertiary care paediatric orthopaedic hospital as a case–control study. Within a timeframe of four years, the patients were collected.
Eighty-eight knees (45 left) in 67 patients (21 patients with bilateral dislocations, 42 females, mean age 14.8 years ± 2.8 standard deviation SD) with recurrent patellar dislocation (dislocation group) were compared to a control group of 54 healthy knees (27 left) in 27 healthy volunteers (14 females, mean age 14.9 years ± 2.4 SD). Only one knee per volunteer in the healthy group was assessed. Randomisation within the statistical programme picked 27 knees out of 27 volunteers. The control group did not differ in age, sex, weight, height, and Body Mass Index (BMI) to the patient group (Table 1). All included patients reported a history of at least three or more patellar dislocations in the affected knee. Patients were excluded in case of previous lower limb surgeries, systemic diseases, other ligamentous traumas than the medial patella-femoral ligament (MPFL), permanent knee pain after patellar dislocation, or pain as the leading symptom, abnormal femoral torsion > 25° (assessed with radiographs according to Dunn [16]), abnormal tibial torsion > 25° (assessed clinically), valgus or varus of the knee (deviation of mechanical axis > 1 cm from midline as evaluated on a standing whole-leg radiograph), leg length discrepancy of more than 0.5 cm, cerebral palsy, infection in the knee.
3-Dimensional gait analysis
A standardised 3D-gait analysis was performed in both groups (dislocation group and control) the same way. Reflective markers (14-mm diameter) were attached bilaterally on the skin of bony landmarks on legs and pelvis. The participants were walking barefoot on level ground on a 10 m walkway at a self-selected speed. The movements of the ankle, knee, hip, and pelvis were captured with a VICON motion analysis system (Oxford Metrics Ltd, Oxford, UK), including 12 infrared cameras (recording at 200 Hz), and transformed the data into a Plug-in-Gait model [24]. 3D ground reaction forces (kinetic data) were assessed with two force plates (Kistler Instrumente AG, Winterthur, Switzerland, recording at 2400 Hz). Values were normalised to kg bodyweight and moments were calculated as internal moments of the knee, hip, and ankle.
Within the VICON software (Nexus and Polygon) a gait cycle was defined visually as the time between two foot strikes of the same leg, corresponding 100% of a gait cycle. This gait circle consisted of 51 data points. Also, toe-off during the gait cycle was set visually to distinguish between stance and swing phase, according to the force plate measurements. All measured joints were normalised to this 100% gait cycle. All participants completed six trials. Out of these six trials, an average gait cycle per participant was computed with all appending variables like joint angles, moments, or temporospatial values. The average gait cycles were compared from the dislocation group to the control group.
Variables
Temporospatial values were compared: walking speed (m/s), cadence (steps/min), step time (s), stride length (m). The duration of the stance phase (the time of the toe-off of index leg), the time of the opposite toe-off and the time of the opposite foot-contact were recorded in the percentage of the gait cycle. The 100% of the gait cycle of the index leg were divided into smaller sub-phases according to the definitions followed (Fig. 1). The “initial contact” was defined as the first contact of the index foot to the floor, corresponding to the first data point (out of 51) during the gait cycle. The “loading-response” was defined as the time (in % of one gait cycle) between the initial contact of the index leg and the toe-off of the opposite side. This portion of the gait cycle corresponds to the first part of the double support time when both feet are on the ground. The “mid-stance phase” was defined as the time (in % of one gait cycle) between the toe-off of the opposite side and initial contact on the opposite side. This portion corresponds to the single-support time when only the index leg is on the ground. The mid-stance phase was divided equally into two halves, namely “initial mid-stance phase” for the first, and “terminal mid-stance phase” for the second part. This step indicates an arbitrary partition of the stance phase.

Gait cycle with different sub-phases. Sub phases are defined as followed: red indicates the index foot, blue indicates the opposite foot. Initial contact: index foot touches the ground (red). Loading-response: time between initial contact of the index foot (red) and the toe off of the opposite foot (blue). This part corresponds to the first part of the double-support. Mid-stance phase: time between the toe off of the opposite foot (blue) and the initial contact of the opposite foot (blue). For the kinematics the mid-stance phase was divided equally in two additional sub phases. This part corresponds to the single-support. Pre-swing phase: time between the initial contact of the opposite foot (blue) and the toe off of the index foot (red). This part corresponds to the second part of the double-support. Swing phase: time between the toe off of the index foot (red) and the initial contact of the index foot (red). For the kinematics the swing phase was divided equally in three additional sub phases. One stride corresponds to one gait cycle of 100%
The “pre-swing phase” was defined as the time (in % of the gait cycle) between the initial contact of the opposite foot and the toe-off of the index side. This portion of the gait cycle corresponds to the terminal part of the double-support time when both feet are on the ground.
Swing-phase was defined as the time (in % of the gait cycle) between the toe-off and initial contact on the index side. The index foot is in the air. The swing phase was divided equally into three sub-phases: initial, mid and terminal swing. This step indicates an arbitrary partition of the swing phase. The 51 data points were distributed according to the percentage of the particular phases, resulting in a different amount of data points per sub-phase. In each sub-phase, the maximum and minimum, as well as the mean of the data points were calculated. Kinematic (angles in °) and kinetic values (Nm/kg) were compared to the control group for the hip, knee, ankle, and the anterior tilt of the pelvis in the sagittal plane. Gait analysis has a good test–retest reliability for lower limb kinematics and kinetics [25, 30, 41].
The responsible IRB (University of Basel, No. 2013/104) approved the study protocol.
Statistical analysis
Data were analysed using a standard statistical software package (JMP version 10, SAS Institute, Cary, USA). A Shapiro–Wilk normality test was performed to verify whether data met the assumption of a parametric test. Normally and not normally distributed continuous data were compared using t test and Wilcoxon signed-rank test, respectively. Ordinal and nominal data were analysed using Wilcoxon signed-rank test and Chi2-Test, correspondingly.
The measured knee flexion and the amount plantar-flexion as well the hip flexion were correlated in each sub-phase. To measure the correlation (linear dependence) between these variables, we used the Pearson correlation coefficient for normally distributed data and Spearman’s rho coefficient for not normally distributed data. A multiple regression model for the knee flexion was computed using the ankle and hip flexion as variables. A P value of less than 0.05 was considered to be statistically significant. Tukey HSD correction for multiple comparisons was applied. Additionally, based on a standard deviation of the normal population (control group) a power analysis to detect a difference of minimum 5° in kinematic between the preoperative and postoperative values was performed. With an α of 0.05, a β of 0.8 and we calculated an effect size of 0.5 resulting in a total sample size of 134 (asymmetrical calculation with 80 pathological knees and 54 healthy knees).
Results
The groups did not differ in age, weight, height, BMI, or sex (Table 1).
Temporospatial parameters
Patients with dislocations decreased their walking speed and stride length (Table 2).
The loading response in the dislocation group increased. The midstance phase (initial and terminal together) decreased its duration, consecutively. Consequently, the time for double support increased (Table 2).
Kinematics
Knee
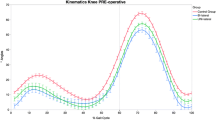
The dislocation group decreased flexion during the entire gait cycle compared to the control (P < 0.01). The most substantial difference of 9.5° ± 0.4 SE occurred during the initial mid-stance phase. The knee flexed maximally during the initial mid-stance phase in both groups.
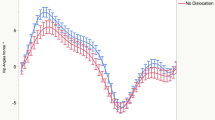
Likewise, the minimal peak occurred during the same phase in both groups, but significantly lower and earlier in the dislocation group Patients reduced their flexion under 15° during loading-response and initial mid-stance in over 80% of all cases, under 10° in 49% and 54%, respectively. Three knees (outliers) in three patients increased their flexion significantly 28° during the loading-response and to 32° during initial mid-stance phase (P < 0.01) (Fig. 2b, Table 3).

a–f Sagittal kinematic angles of the knee. Positive values indicate flexion, negative extension of the knee. Each error bar is constructed using a 95% confidence interval of the mean
Ankle
The plantar-flexion increased during initial contact and loading-response with dislocations, and likewise, the dorsal-extension decreased during the initial and terminal midstance phase (Fig. 2a, Table 3).
Hip
The hip flexion decreased significantly with dislocations during all eight sub-phases with a maximal difference during mid-stance phase (Fig. 2c, Table 3).
Pelvis
The pelvis’ anterior tilt did not vary between the groups during all phases.
Kinetics
Knee
The dislocation group decreased internal moments during the initial midstance phase. Highest moments were noted during the same phase in both groups. Likewise, the minimal peak occurred during the midstance phase in both groups, but without a significant difference (Fig. 2e, Table 4).
Ankle
The plantar-flexion moments increased in the dislocation group during initial contact and loading-response, respectively (P < 0.001) (Fig. 2d, Table 4).
Hip
Hip flexion moments decreased significantly from initial contact to terminal midstance phase with dislocations. (Fig. 2f, Table 4).
The correlation between knee flexion and plantar-flexion was high and statistically significant, in particular during the initial midstance phase. Likewise, the relationship between knee flexion and hip flexion was also strong and statistically significant, most substantially during initial midstance phase (Table 5).
The multiple regression revealed a robust model for the loading response and initial mid-stance phase to predict the knee flexion with the variables ankle flexion and hip flexion.
Prediction expression for loading-response:
-
Knee angle° = 1.82 + 0.96 × Ankle angle° + 0.47 × Hip angle°
-
(R2 = 0.65, Mallow’s Cp = 3, P < 0.0001)
Prediction expression for initial mid-stance phase:
-
Knee angle° = 1.52 + 1.22 × Ankle angle° + 0.48 × Hip angle°
-
(R2 = 0.77, Mallow’s Cp = 3, P < 0.0001)
The residuals were normally distributed.
All other phases expressed regressions below an R2 = 0.55.
Discussion
The most important findings in this study were:
First, knee flexion decreased during the entire gait cycle compared to a control group. Over 80% of our patients developed a gait pattern with less than 15° of knee flexion during loading-response or initial mid-stance phase; 55% were under 10° of flexion. In addition, the time for the loading-response extended, a part of the double support, what shortened the following mid-stance phase for the same amount.
Second, the ankle’s plantar-flexion increased during loading-response, and dorsal-extension decreased afterward, whereas the hip flexion decreased during the entire gait cycle.
Third, internal moments of the ankle and the hip changed predominately during the first part of the stance phase (ankle increased, hip decreased), whereas in the knee moments decreased only in the initial midstance phase.
Evidence of a possible linkage between a decreased knee flexion during the stance phase and pathology of the knee comes from different studies dealing with anterior cruciate ligament deficiencies (ACL) or a patellofemoral pain syndrome (PFPS) [6, 7, 19, 22, 27, 31, 37, 45, 46]. Berchuck et al. describes this decrease as a quadriceps avoidance gait seen in 75% of all ACL knees. It is thought that a quadriceps avoidance protects the knee against the anterior drawer of the tibia, i.e., an instability or a pivoting, as the quadriceps tends to displace the tibia between 0° and 45° of flexion [7]. While this principle is controversially discussed [35, 36], it can be used to identify copers or non-copers in a conservative treatment, whereas copers do not develop a quadriceps avoidance [1, 11, 28, 37, 43]. PFPS, as well as osteoarthritis, can have an identical effect [29]. However, patients of this study did not complain of any pain or other discomforts during level walking; thus it is highly unlikely that PFPS or OA had precipitated the changes observed. Furthermore, patients with recurrent patellar dislocations have a more pronounced decrease of knee flexion than in an ACL or PFPS [7, 11, 28, 31, 37, 42, 46]. This reduced flexion could be an effective factor avoiding the patella to enter the trochlear groove and, therefore, creating instability.
In this patient series, instead of reducing, three cases (3.4%) increased their flexion over 28° during the loading-response and even over 31° during the midstance phase. These outliers drew our attention, explaining a possible second compensation mechanism. The trochlear groove normalises its shape during flexion and the patella has more contact pressure in it. These patients could as well avoid the least stable area, making a dislocation less probable [39]. After all, this gait pattern is less energy preserving than the quadriceps avoidance, a reason, why it could be rare. Certainly, it is debatable if a sample size of three is already enough to announce a new compensatory mechanism.
Data on ankle plantar-flexion revealed a significant increase during the loading-response and decrease afterward compared to the control. The plantar-flexion correlated strongly with the knee extension. At the same time, internal moments for plantar flexors increased significantly. Plantar-flexion straightens the knee during the loading-response and mid-stance phase as the Soleus muscle pulls back the tibia on a fixed foot. This principle is well established and called the plantar-flexion/knee extension-couple [8, 26, 38]. This might be a compensatory mechanism to control the knee. However, the findings of the present study are not consistent with previous studies regarding ACL or PFPS patients with no changes in the ankle kinematic [31, 37]. Moreover, from a geometrical point of view, a reduced knee flexion always causes an increased plantar-flexion. Per contra, this study’s patients extended their knees more than ACL or PFPS patients, what makes a contribution of the plantar-flexion/knee extension-couple more probable.
Regarding the hip flexion, the same issues can be discussed. Hip flexion decreased significantly during the entire gait cycle and was correlated with the knee’s range of motion. Likewise, hip flexion moments decreased significantly. Our findings are consistent with Nadeau, which reports a trend to reduced hip flexion in patients with PFPS [31]. Like the plantar-flexion/knee extension-couple, hip extensors can retract the femur during loading-response, and, therefore, extend the knee [4, 33]. Again, it is debatable at this point, whether this is a compensatory mechanism to control the knee or since knee and hip are corresponding joints, they have to adjust each other geometrically. By implication, the latter pushes the hip’s influence into a passive role.
However, the regression model emphasizes an active influence of the ankle and hip to the knee. Consequently, while postulating quadriceps avoidance, an alternative control for the knee must exist. The knee is not entirely controlled by the plantar-flexion/knee extension couple and the hip extensors; however, these mechanisms contribute substantially to compensate for the deficiency.
Facing such a deficiency, patients extended their loading-response (double support). They shortened the following mid-stance phase (single support) for the same amount. These changes in the most sensitive part of the gait are interpreted as an attempt to reduce uncertainty with spending more time on both feet.
There are several limitations to this study.
Only adolescents were included in the study. The findings cannot be adopted for adults without reservation.
The participants walked barefoot on the level ground. Therefore, the results cannot be generalised to footwear or other activities. However, the laboratory conditions given in our study allows us to compare data more reliably.
Furthermore, the gait analysis was performed at a self-selected speed. Due to the consequent individual walking velocities, we are not able to assure uniform stress to the knee joint. In that way, however, differences can be detected in the walking velocity between the two groups. Nevertheless, a significant difference in walking speed and stride length was measured. However, this difference is clinically not relevant.
Conclusion
Recurrent patellar dislocation decreases knee flexion during the loading-response and mid-stance phase. A decreased hip flexion and increased plantar-flexion, while adjusting internal moments, indicate a compensation mechanism.
References
Alkjaer T, Simonsen EB, Peter Magnusson SP, Aagaard H, Dyhre-Poulsen P (2002) Differences in the movement pattern of a forward lunge in two types of anterior cruciate ligament deficient patients: copers and non-copers. Clin Biomech (Bristol, Avon) 17:586–593
Amis AA (2007) Current concepts on anatomy and biomechanics of patellar stability. Sports Med Arthrosc 15:48–56
Amis AA, Oguz C, Bull AMJ, Senavongse W, Dejour D (2008) The effect of trochleoplasty on patellar stability and kinematics: a biomechanical study in vitro. J Bone Jt Surg Br 90:864–869
Arnold AS, Anderson FC, Pandy MG, Delp SL (2005) Muscular contributions to hip and knee extension during the single limb stance phase of normal gait: a framework for investigating the causes of crouch gait. J Biomech 38:2181–2189
Banke IJ, Kohn LM, Meidinger G, Otto A, Hensler D, Beitzel K, Imhoff AB, Schöttle PB (2014) Combined trochleoplasty and MPFL reconstruction for treatment of chronic patellofemoral instability: a prospective minimum 2-year follow-up study. Knee Surg Sports Traumatol Arthrosc 22:2591–2598
Barton CJ, Levinger P, Menz HB, Webster KE (2009) Kinematic gait characteristics associated with patellofemoral pain syndrome: a systematic review. Gait Posture 30:405–416
Berchuck M, Andriacchi TP, Bach BR, Reider B (1990) Gait adaptations by patients who have a deficient anterior cruciate ligament. J Bone Jt Surg Am 72:871–877
Brunner R, Dreher T, Romkes J, Frigo C (2008) Effects of plantar flexion on pelvis and lower limb kinematics. Gait Posture 28:150–156
Camathias C, Speth BM, Rutz E, Schlemmer T, Papp K, Vavken P, Studer K (2018) Solitary trochleoplasty for treatment of recurrent patellar dislocation. JBJS Essent Surg Tech 8(2):e11
Camathias C, Studer K, Kiapour A, Rutz E, Vavken P (2016) Trochleoplasty as a solitary treatment for recurrent patellar dislocation results in good clinical outcome in adolescents. Am J Sports Med 44:2855–2863
Chmielewski TL, Rudolph KS, Fitzgerald GK, Axe MJ, Snyder-Mackler L (2001) Biomechanical evidence supporting a differential response to acute ACL injury. Clin Biomech (Bristol, Avon) 16:586–591
Chotel F, Bérard J, Raux S (2014) Patellar instability in children and adolescents. Orthop Traumatol Surg Res 100:S125–S137
Christensen TC, Sanders TL, Pareek A, Mohan R, Dahm DL, Krych AJ (2017) Risk factors and time to recurrent ipsilateral and contralateral patellar dislocations. Am J Sports Med 45:2105–2110
Colvin AC, West RV (2008) Patellar instability. J Bone Jt Surg Am 90:2751–2762
Dejour H, Walch G, Nove-Josserand L, Guier C (1994) Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc 2:19–26
Dunn DM (1952) Anteversion of the neck of the femur; a method of measurement. J Bone Jt Surg Br 34-B:181–186
Firer P, Mountney J, Senavongse W, Thomas NP (2003) Anatomy and biomechanics of the medial patellofemoral ligament. Knee 10:215–220
Fithian DC (2004) Epidemiology and natural history of acute patellar dislocation. Am J Sports Med 32:1114–1121
Hart JM, Ko J-WK, Konold T, Pietrosimone B, Pietrosimione B (2010) Sagittal plane knee joint moments following anterior cruciate ligament injury and reconstruction: a systematic review. Clin Biomech (Bristol, Avon) 25:277–283
Hautamaa PV, Fithian DC, Kaufman KR, Daniel DM, Pohlmeyer AM (1998) Medial soft tissue restraints in lateral patellar instability and repair. Clin Orthop Relat Res 349:174–182
Hawkins RJ, Bell RH, Anisette G (1986) Acute patellar dislocations. The natural history. Am J Sports Med 14:117–120
Hurd WJ, Snyder-Mackler L (2007) Knee instability after acute ACL rupture affects movement patterns during the mid-stance phase of gait. J Orthop Res 25:1369–1377
Insall J, Goldberg V, Salvati E (1972) Recurrent dislocation and the high-riding patella. Clin Orthop Relat Res 88:67–69
Kadaba MP, Ramakrishnan HK, Wootten ME (1990) Measurement of lower extremity kinematics during level walking. J Orthop Res 8:383–392
Kainz H, Graham D, Edwards J, Walsh HPJ, Maine S, Boyd RN, Lloyd DG, Modenese L, Carty CP (2017) Reliability of four models for clinical gait analysis. Gait Posture 54:325–331
Kimmel SA, Schwartz MH (2006) A baseline of dynamic muscle function during gait. Gait Posture 23:211–221
Knoll Z, Kocsis L, Kiss RM (2004) Gait patterns before and after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 12:7–14
Lindström M, Felländer-Tsai L, Wredmark T, Henriksson M (2010) Adaptations of gait and muscle activation in chronic ACL deficiency. Knee Surg Sports Traumatol Arthrosc 18:106–114
Maenpaa H, Lehto MU (1997) Patellar dislocation. The long-term results of nonoperative management in 100 patients. Am J Sports Med 25:213–217
Mentiplay BF, Clark RA (2018) Modified conventional gait model versus cluster tracking: test-retest reliability, agreement and impact of inverse kinematics with joint constraints on kinematic and kinetic data. Gait Posture 64:75–83
Nadeau S, Gravel D, Hébert LJ, Arsenault AB, Lepage Y (1997) Gait study of patients with patellofemoral pain syndrome. Gait Posture 5:21–27
Nietosvaara Y, Aalto K, Kallio PE (1994) Acute patellar dislocation in children: incidence and associated osteochondral fractures. J Pediatr Orthop 14:513–515
Perry J, Burnfield JM (2010) Gait analysis. SLACK Incorporated, New Jersey
Redler LH, Wright ML (2018) Surgical management of patellofemoral instability in the skeletally immature patient. J Am Acad Orthop Surg 26:e405–e415
Reed-Jones RJ, Vallis LA (2008) Kinematics and muscular responses to a ramp descent in the ACL deficient knee. Knee 15:117–124
Roberts CS, Rash GS, Honaker JT, Wachowiak MP, Shaw JC (1999) A deficient anterior cruciate ligament does not lead to quadriceps avoidance gait. Gait Posture Elsevier 10:189–199
Rudolph KS, Eastlack ME, Axe MJ, Snyder-Mackler L (1998) 1998 Basmajian Student Award Paper: movement patterns after anterior cruciate ligament injury: a comparison of patients who compensate well for the injury and those who require operative stabilization. J Electromyogr Kinesiol 8:349–362
Schwartz M, Lakin G (2003) The effect of tibial torsion on the dynamic function of the soleus during gait. Gait Posture 17:113–118
Senavongse W, Amis AA (2005) The effects of articular, retinacular, or muscular deficiencies on patellofemoral joint stability: a biomechanical study in vitro. J Bone Jt Surg Br 87:577–582
Senavongse W, Farahmand F, Jones J, Andersen H, Bull AMJ (2006) Quantitative measurement of patellofemoral joint stability: force–displacement behavior of the human patella in vitro. J Orthop Res 21:780–786
Stief F, Böhm H, Michel K, Schwirtz A, Döderlein L (2013) Reliability and accuracy in three-dimensional gait analysis: a comparison of two lower body protocols. J Appl Biomech 29:105–111
Torry MR, Decker MJ, Ellis HB, Shelburne KB, Sterett WI, Steadman JR (2004) Mechanisms of compensating for anterior cruciate ligament deficiency during gait. Med Sci Sports Exerc 36:1403–1412
Torry MR, Decker MJ, Viola RW, O'Connor DD, Steadman JR (2000) Intra-articular knee joint effusion induces quadriceps avoidance gait patterns. Clin Biomech (Bristol, Avon) 15:147–159
Vavken P, Wimmer MD, Camathias C, Quidde J, Valderrabano V, Pagenstert G (2013) Treating patella instability in skeletally immature patients. Arthroscopy 29:1410–1422
Werner S (2014) Anterior knee pain: an update of physical therapy. Knee Surg Sports Traumatol Arthrosc 22:2286–2294
Wexler G, Hurwitz DE, Bush-Joseph CA, Andriacchi TP, Bach BR (1998) Functional gait adaptations in patients with anterior cruciate ligament deficiency over time. Clin Orthop Relat Res 348:166–175
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
All authors have nothing to disclose that could have direct or potential influence or impart bias on the work.
Funding
No external source of funding was used.
Ethical approval
This research has been performed with the approval of the local ethics committee (ethics committee of Basel, No. 2013/104).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Camathias, C., Ammann, E., Meier, R.L. et al. Recurrent patellar dislocations in adolescents result in decreased knee flexion during the entire gait cycle. Knee Surg Sports Traumatol Arthrosc 28, 2053–2066 (2020). https://doi.org/10.1007/s00167-020-05911-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-020-05911-y