
Abstract
Purpose
Given the increasing incidence of arthroscopic anterior cruciate ligament reconstruction (ACLR), mid- to long-term rates of reoperations were investigated on the ipsilateral knee following ACLR.
Methods
New York Statewide Planning and Research Cooperative Systems (SPARCS) database was queried from 2003 to 2012 to identify patients with a primary ICD-9 diagnosis for ACL tear and concomitant CPT code for ACLR. Patients were longitudinally followed for at least 2 years to determine incidence and nature of subsequent ipsilateral knee procedures.
Results
The inclusion criteria were met by 45,231 patients who had undergone ACLR between 2003 and 2012. Mean age was found to be 29.7 years (SD 11.6). Subsequent ipsilateral outpatient knee surgery after a mean of 25.7 ± 24.5 months was performed in 10.7% of patients. Revision ACLR was performed for nearly one-third of reoperations. Meniscal pathology was addressed in 58% of subsequent procedures. Age 19 or younger, female gender, worker’s compensation (WC) insurance, and Caucasian race were identified as independent risk factors for any ipsilateral reoperation. An initial isolated ACLR and initial ACLR performed by a high-volume surgeon were found to be independently associated with lower reoperation rates. Tobacco use was not significant. Survival rates of 93.4%, 89.8% and 86.7% at 2-, 5- and 10 years, respectively, were found for any ipsilateral reoperation.
Conclusion
A 10.7% ipsilateral reoperation rate at an average of 25.9 (SD 24.5) months after ACLR and an overall ACLR revision rate of 3.1% were demonstrated by the analysis. Meniscal pathology was addressed in the majority of subsequent interventions. Age 19 or younger, female gender, Caucasian race, and WC claim were associated with reoperation. Initial isolated ACLR and procedure performed by high-volume surgeon were associated with reduced reoperation.
Level of evidence
Level III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anterior cruciate ligament (ACL) injuries are among the most common sports-related injuries in the United States, with reported estimates ranging up to 200,000 annually [31, 36, 51]. Arthroscopic-assisted anterior cruciate ligament reconstruction (ACLR) is the most common surgical technique to manage this condition and has led to favorable long-term outcomes [6, 9,10,11, 21, 34].
Reoperation rates following ACLR range between 6.5 and 34% [16, 26, 36, 54, 59]. However, small numbers or short-term follow-up, inclusion of contralateral procedures, or lack clinical detail for procedures performed during reoperation were reported by many of these studies. Additionally, revision ACLR rates without comment on all ipsilateral reoperations were reported by most large database studies [40, 57, 62]. The purpose of this study was to report mid- to long-term rates of all reoperations on the ipsilateral knee following arthroscopic ACLR. The authors aim to use a large, heterogeneous sample to determine whether a variety of captured demographic and surgeon factors are independent risks for requiring further ipsilateral surgical procedures after initial ACLR. Based on findings from previous large registry studies conducted on reoperation rates following ACLR, the hypothesis was that reoperation rates would be low, high-volume surgeons would have lower reoperation rates, and risk factors for reoperation would include female gender and young age.
Materials and methods
The SPARCS database was established by the New York State Department of Health in 1979, and reporting discharges from all nonfederal, licensed hospitals in New York State was mandated by the New York State Public Health Law in 1986. Emergency rooms and freestanding, licensed ambulatory surgery facilities were included in the subsequent expansion of these requirements. Patient level data on patient characteristics, diagnoses and treatments, and charges are now included for each hospital inpatient and outpatient visit. All New York State Hospitals are required to be 100% compliant with submission of SPARCS data. The SPARCS database has been used to examine trends in numerous peer-reviewed orthopaedic publications [5, 20, 29, 44]. Of note, real numbers of all included meniscus and cartilage reoperations are included in the SPARCS database.
Patients were identified utilizing Current Procedural Terminology (CPT) and International Classification of Diseases (ICD-9) codes. Patients between the ages of 10 and 60 years with a primary diagnosis of ACL tear (717.83 or 844.2) and CPT code 29,888 (arthroscopic ACL reconstruction) were identified with methodology similar to previous ACLR database studies [12, 41]. Patients with prior arthroscopic ipsilateral knee surgery were excluded.
Patients who underwent ACLR were tracked using an encrypted unique patient identifier and followed for a minimum of 2 years for the incidence of additional knee surgery. All ACLR identified between 2003 and 2012 were followed through 2014, thus ensuring minimal 2-year follow-up (maximal 11-year follow-up). For patients who had multiple subsequent surgeries, only the first surgery immediately after the initial ACLR was used for the purposes of data analysis. Similar to previous literature, subsequent open and arthroscopic procedures were identified by common CPT codes [12, 24, 27, 36, 45]. All initial procedures were performed arthroscopically.
The study was exempted by the New York University School of Medicine Institutional Review Board as non-human subject research.
Statistical analysis
Statistical analysis using SAS® 9.3 (SAS Institute, Cary NC) was performed to compare those undergoing additional surgery to those that did not. Differences in continuous variables were evaluated with a Student’s t test, while Fisher Exact test and Chi-squared analysis were used for categorical variables. Age was examined as both a continuous and binary variable. Similar to previous methodology, the number of ACLRs performed in New York State 12 months prior to the index ACLR was used to stratify surgeon volume into high, medium, or low [16, 36]. 52 or more ACLR per year were performed by high-volume surgeons, between 6 and 51 ACLR per year were performed by mid-volume surgeons, and those who performed less than 6 ACLR per year were low-volume surgeons. To explore the impact of concomitant procedures on ACLR reoperation rates, patients were collapsed into four groups based on the nature of their index surgery: isolated ACLR, ACLR with concomitant meniscal procedure, ACLR with concomitant meniscal procedure and another procedure, ACLR with concomitant procedure not involving meniscus [16]. Patients with tobacco-use disorder were identified using ICD-9 code 305.1 [12, 56].
Subgroup analysis was performed on patients who had subsequent surgery to determine if subsequent procedures were correlated with mean age at time of initial ACLR. For this analysis, a one-way ANOVA was performed, and subsequent pairwise comparison was performed for each specific subsequent procedure using “overall mean age at reoperation” for comparison. The same method was used to determine whether significant differences occurred in mean time until reoperation for specific procedures. Kaplan–Meier analysis was performed to determine reoperation-free survival, and survival probabilities were provided for 2-, 5-, and 10-year intervals. Reoperation or final follow-up through the year 2014 for all patients was censored. Multivariate logistic regression that controlled for age, gender, race, insurance, surgeon experience, and nature of initial ACLR was performed to determine independent risk factors for subsequent surgery and for revision ACLR. p values < 0.05 were considered statistically significant for all analyses.
Results
45,231 patients met the inclusion criteria and underwent arthroscopic ACLR between 2003 and 2012. Baseline demographic characteristics for the sample and complete distributions for each covariate can be found in Table 1.
Patients requiring ipsilateral surgery and those who did not are compared in Table 2. After a minimum follow-up of 2 years, subsequent outpatient ipsilateral knee surgery at a mean of 25.9 ± 24.5 months after index ACLR was performed in 10.7% of patients (4,830/45,231). Overall rates of subsequent ipsilateral surgery were found to be higher in females than males (11.2% vs 10.3%, p < 0.002). Higher rates of reoperation were associated with concomitant procedures at the time of index surgery compared to isolated ACLR (11.2% vs 10%, p < 0.001).
The distribution of subsequent procedures and most common diagnoses at first reoperation are detailed in Table 3. In patients undergoing a subsequent procedure, 28.3% had a revision arthroscopic ACLR and 0.8% underwent open ACLR. An overall 3.1% rate of ACLR revisions was represented by these patients (1406/45,231). Patients who had a meniscal repair with initial ACLR were 2.5 times more likely to have a subsequent meniscectomy than those who did not (odds ratio 2.50, confidence interval 2.25–2.77).
A subgroup analysis was performed on those 4830 patients who underwent reoperation. Average time in months until reoperation was widely varied based upon nature of subsequent procedure (Fig. 1). As was outlined in the “Methods” section, the reference value for statistical comparisons in this analysis was the mean time to reoperation for the sample (25.9 months; SD 24.9). Stiffness-related procedures (8.9 months; SD 14.9) were performed significantly earlier than reference value (p < 0.05). By comparison, subsequent revision ACLR (27.4 months; SD 23.7), meniscectomy (32.1 months; SD 26.5), and meniscal repair (27.6 months, SD 26.5) were performed on patients after the reference value of 25.9 months (p < 0.01 for all values).

Mean time until reoperation by procedure
Mean age at time of initial ACLR was associated with the type of reoperation that patients underwent, as depicted in Fig. 2. Similar to above, the mean age at initial ACLR for all patients undergoing reoperation (28.3 SD 11.4) was used as the reference value for statistical significance. Those undergoing revision ACLR (25.4, SD 10.4) and meniscal repair (22.5, SD, 9.4) were younger at time of initial ACLR when compared to the reference value (p < 0.01). Patients who had only one reoperation were 28.5 years old (11.4) at initial ACLR. By comparison, those having two subsequent reoperations were 27.6 (10.9) and those having three or more reoperations were 26.9 (11.3) at initial ACLR, respectively (p < 0.01 for both).

Mean age at initial ACLR for specific reoperation procedures
Female gender was associated with a higher overall reoperation rate (11.2% vs 10.3%, p < 0.002). The differences with regard to specific reoperation procedure existing across genders were revealed by subgroup analysis (Fig. 3). Most notably, revision ACLR (3.41% vs 2.65%, p < 0.001) and meniscectomy (5.77% vs 5.34%, p < 0.05) were found to be significantly more likely in males than females. By comparison, a greater incidence of subsequent cartilage procedures (2.33% vs 1.95%, p < 0.05) and nearly twice the rate of stiffness-related interventions (1.42% vs 0.75%, p < 0.001) were identified in females.

Rates of specific reoperation procedures by gender
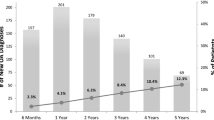
Results from the Kaplan–Meier survival analyses can be found in Fig. 4. Similar survival probabilities, with 2-, 5-, and 10-year probabilities of 98.4%, 96.7%, and 95.6%, respectively, were demonstrated by contralateral ACLR.

Event-free survival analysis after ACLR
Age younger than 19 years (OR 1.41, 1.32–1.51, p < 0.001), female gender (OR 1.09, 1.03–1.16, p = 0.004), worker’s compensation insurance (OR 1.70, 1.54–1.88, p < 0.001), and Caucasian race (OR 1.32, 1.23–1.42, p < 0.001) were suggested to be independent risk factors for any ipsilateral knee reoperation after ACLR by multivariate analysis (Fig. 5). An initial isolated ACLR (OR 0.85, 0.80–0.90, p < 0.001) and having initial ACLR performed by a high-volume surgeon (OR 0.90, 0.83–0.97, p = 0.021) were independently associated with lower rates of reoperation, while tobacco use was not significant (OR 0.89, 0.74–1.10, n.s.).

Risk Factors for reoperation after ACLR
A separate multivariate analysis (Fig. 6) was performed to identify risk factors specific for revision ACLR. Age younger than 19 years (OR 2.11, 1.89–2.36, p < 0.001), male gender (OR 1.42, 1.27–1.60, p < 0.001), worker’s compensation insurance (OR 1.36, 1.11–1.66, p = 0.002), and Caucasian race (OR 1.29, 1.14–1.46, p < 0.001) were determined to be independent risk factors for revision surgery. High surgeon volume (OR 1.08, 0.95–1.25, n.s.), initial isolated ACLR (OR 1.03, 0.92–1.15, n.s.), and tobacco use (OR 0.93, 0.64–1.34, n.s.) were not independently associated with revision ACLR.

Risk Factors for revision ACLR
Discussion
The most important finding in this study was a 10.7% rate of subsequent surgical intervention on the ipsilateral knee at an average of 25.9 (24.5) months. Overall ACLR revision rate in the sample was found to be 3.1%. Independent risk factors for any reoperation were: age under 19 years, female gender, Caucasian race, index ACLR with concomitant procedure, and worker’s compensation claim. Having the index ACLR performed by a high-volume surgeon was associated with reduced incidence of reoperation.
Age under 19 years as an independent risk factor for reoperation was found in the study (OR 1.41, 1.32–1.51) and has been consistently reported in previous studies [19, 23, 40, 62]. Reasons for this finding were likely due to a combination of younger patients demonstrating the highest participation in athletic activities that had predisposed them to initial ACL injuries, a greater willingness to undergo subsequent surgery to be able to return to play, and predisposition for injury or reinjury due to factors such as alignment [35, 37, 38].
Cartilage procedures and stiffness-related interventions were performed in females in the cohort at a greater rate than males (Fig. 3). Interestingly, similar gender-related differences regarding cartilage damage after ACLR were found in a recent animal study by Kiapour et al. In their animal model, statistically significant greater cartilage damage after ACLR was observed in females, potentially due to decreased vascularity in females as compared to males [30]. Future studies addressing gender-related differences are warranted, particularly when considering that over 75% of young individuals had developed post-traumatic osteoarthritis after ACL injury [30, 61].
Nearly twice the reoperation rate for stiffness-related interventions was found in females, a finding which has been previously reported. A study of 933 knees by Nwachukwu et al. found that females were 2.8 times more likely to develop arthrofibrosis than males [43]. Reasons for this gender difference remain unclear, with some authors attributing differences to variations in hormone expression [18, 32, 53], while others had suggested that females may be more likely than males to seek intervention to restore range of motion (ROM) after ACLR [48]. Stiffness-related interventions were performed at a mean of 8.9 months in this study (Fig. 1), and is in agreement with a mean of 9 months described by Nwachukwu et al. [43].
Caucasian race as an independent risk factor for reoperation was identified (OR 1.32, 1.23–1.42), a finding that has been previously reported [38, 58]. Although insurance status was accounted for in the multivariate analysis, socioeconomic status and access to care were unable to be controlled for and are factors that previous authors have suggested may be responsible for observed race-related differences [13]. Worker’s compensation claims as an independent risk factor for reoperation (OR 1.7, 1.54–1.88) is relatively novel in such a large cohort registry study and is in line with previous authors’ reports that workers’ compensation is associated with lower subjective outcomes after ACLR [8], mirroring reports across other orthopaedic subspecialties [3, 4, 60].
Initial ACLR performed by a high-volume surgeon (> 52 ACLR/year) was associated with lower risk of any reoperation (OR 0.90, 0.83–0.97, p = 0.021), but was not associated with reduced risk for revision ACLR (OR 1.08, 0.95–1.25, n.s.). The second part of the results are similar to a study by Wasserstein et al. that found that surgeon volume was not associated with revision rates after ACLR [62]. Future studies detailing how practice patterns and intraoperative decision-making differ based on surgeon experience could shed greater light on the current findings, particularly when considering recent studies that have found high-volume surgeons provided a greater economic benefit than all other providers while having fewer adverse events [49].
In the present cohort, a decreased risk for future reoperation was found in patients who had undergone an initial isolated ACLR (0.85, 0.80–0.90). These results add to the existing literature that had reported worse long-term outcome scores and higher failure rates in patients undergoing ACLR with meniscal or cartilage injuries as compared to those without concomitant pathology [7, 28, 33, 47, 50]. Additionally, the fact that nearly 58% reoperations in the cohort occurred due to meniscal pathology could represent that surgeons are more agreeable to surgical re-intervention due to the recognition of the role that untreated meniscal damage has in development of knee osteoarthritis [22, 55]. The finding that initial isolated ACLR was not associated with reduced need for revision ACLR (OR 1.03, 0.92–1.15, p = 0.605) could be influenced by nature and high degree of athletic involvement in patients typically requiring revision ACL reconstruction.
The overall ACLR revision rate in this study population was 3.1%, similar to other large registry studies that have reported revision rates ranging from 1.8 to 3.0% [2, 37, 46]. Results from the survival analyses indicate 5-year ACLR revision free rates of 96.5%, or failure rate of 3.5%. (Fig. 4). This is comparable to results from Swedish and Danish ACLR registries reporting 5-year revision rates of 4.1% [1, 35]. Due to difference in cohorts and significantly limited sample sizes in previous studies, it is more difficult to make direct comparisons to the 10-year survival rate of 95.4% found in this study. A systematic review of 14 studies by Crawford et al. had reported 10-year ACL re-rupture rates of 6.2% (93.8% survivorship) [15].
Risk of revision between patellar tendon and hamstring autografts was examined by a registry study performed by Gifstad et al., which included 45,998 primary ACL reconstructions in Scandinavia. At 2 years following primary ACLR, 1.0% in the patellar group and 2.3% in the hamstring group were expected to undergo revision. Additionally, younger patients were found to have worse outcomes, and female gender was associated with increased time without revision [25]. These reports were consistent with this study; however, direct comparison was limited because graft source and activity levels were unknown in this study, and any reoperation was included.
To the best of the authors’ knowledge, there are only two similar studies that use a large registry to determine rates of all subsequent reoperations, not just revision ACLR. In 2009, Lyman et al. performed a study utilizing the SPARCS database identifying 70,547 patients in a 9-year period from 1997 to 2006 [36]. They reported subsequent surgery was performed on either knee within 1 year in 6.5% of cases with a subsequent ACLR on either knee in 1.9% of cases. The most common subsequent procedures were ACLR (28.7%), lysis of adhesions (28%), and meniscectomy (24.5%). They reported higher rates of subsequent surgery and revision ACLR in females. Patients who had index ACLR that was performed by a low-volume surgeon (< 52 ACL per year) had significantly more subsequent knee procedures. Younger age (less than 20) was associated with a significantly increased rate of revision ACLR. Despite their findings, the most significant limitation of their results was an inability to differentiate laterality of subsequent surgery. Their data reported on procedures performed on “either knee”, making direct correlations difficult to ascertain, particularly when considering that a significant percentage of patients may eventually injure the contralateral ACL [40].
The second study by Csintalan et al. had identified 14,522 patients with mean age of 29 years followed over the short to mid-term (mean follow-up of 1.9 years) [16]. Their overall reoperation rate was 3.9%, with the majority of reoperations addressing meniscal pathology (41%). Although the majority of reoperations in both studies involved the meniscus (58%), the reoperation rate presented in this study was significantly higher at 10.7%. The reason for the significantly higher reoperation observed in this study was likely threefold. First, they did not include revision ACLR in their results—thus reducing reoperation rates, as nearly 1/3rd of reoperations in this study involved revision procedures. Second, their mean follow-up was 1.9 years ± 1.5 (range 0–6.7) as compared to the mean follow-up of 5.6 ± 2.9 (range 0–12) in this study. Finally, their patient population consisted of only 48.3% Caucasians, as compared to a proportion of 68.6% Caucasian, which is a potentially confounding factor as Caucasian race has been implicated in higher reoperation rates [39, 40].
This study was subject to several limitations. As with any large-scale registry analysis, there was inherent reliance on the accuracy of the database being analysed [42]. However, the current analysis utilized a source with previously accepted standards of accuracy for evaluation [14, 17, 44, 52]. Additionally, the type of graft (allograft vs autograft) used during ACLR, radiographic findings, or the nature and degree of athletic involvement were unable to be accounted for. While ICD-9 diagnosis codes were used to identify tobacco use, longevity and intensity (packs per day) of tobacco use were not available. Additionally, patients who may have had reoperations outside of New York State could not be identified. Finally, it is important to keep in mind that subjective outcome scores were independent of the results, and thus patient satisfaction, quality of life improvements, or return-to-sport could not be commented upon.
Overall, the results of this study can help providers identify patients at highest risk for reoperation, predict the nature of subsequent interventions, and counsel patients accordingly.
Conclusion
A 10.7% rate of reoperation at an average of 25.9 (SD 24.5) months and an overall ACLR revision rate of 3.1% were observed in this sample of 45,231 patients, with the majority of subsequent interventions addressing meniscal pathology. Independent risk factors for both reoperation and revision ACLR were age 19 years or younger, female gender, Caucasian race, and WC claim, findings which can be used to counsel patients receiving arthroscopic ACL reconstruction.
References
Ahlden M, Samuelsson K, Sernert N, Forssblad M, Karlsson J, Kartus J (2012) The Swedish National Anterior Cruciate Ligament Register: a report on baseline variables and outcomes of surgery for almost 18,000 patients. Am J Sports Med 40:2230–2235
Andernord D, Desai N, Bjornsson H, Ylander M, Karlsson J, Samuelsson K (2015) Patient predictors of early revision surgery after anterior cruciate ligament reconstruction: a cohort study of 16,930 patients with 2-year follow-up. Am J Sports Med 43:121–127
Anderson JT, Haas AR, Percy R, Woods ST, Ahn UM, Ahn NU (2015) Clinical depression is a strong predictor of poor lumbar fusion outcomes among workers' compensation subjects. Spine 40:748–756 (Phila Pa 1976)
Anderson JT, Haas AR, Percy R, Woods ST, Ahn UM, Ahn NU (2015) Return to work after Diskogenic fusion in workers' compensation subjects. Orthopedics 38:e1065–1072
Bansal A, Khatib ON, Zuckerman JD (2014) Revision total joint arthroplasty: the epidemiology of 63,140 cases in New York State. J Arthroplasty 29:23–27
Barber SD, Noyes FR, Mangine R, DeMaio M (1992) Rehabilitation after ACL reconstruction: function testing. Orthopedics 15:969–974
Barenius B, Forssblad M, Engstrom B, Eriksson K (2013) Functional recovery after anterior cruciate ligament reconstruction, a study of health-related quality of life based on the Swedish National Knee Ligament Register. Knee Surg Sports Traumatol Arthrosc 21:914–927
Barrett GR, Rook RT, Nash CR, Coggin MR (2001) The effect of Workers' Compensation on clinical outcomes of arthroscopic-assisted autogenous patellar tendon anterior cruciate ligament reconstruction in an acute population. Arthroscopy 17:132–137
Baverel L, Demey G, Odri GA, Leroy P, Saffarini M, Dejour D (2015) Do outcomes of outpatient ACL reconstruction vary with graft type? Orthop Traumatol Surg Res 101:803–806
Brandsson S, Faxen E, Eriksson BI, Sward L, Lundin O, Karlsson J (1999) Reconstruction of the anterior cruciate ligament: comparison of outside-in and all-inside techniques. Br J Sports Med 33:42–45
Buss DD, Warren RF, Wickiewicz TL, Galinat BJ, Panariello R (1993) Arthroscopically assisted reconstruction of the anterior cruciate ligament with use of autogenous patellar-ligament grafts. Results after twenty-four to forty-two months. J Bone Jt Surg Am 75:1346–1355
Cancienne JM, Gwathmey FW, Miller MD, Werner BC (2016) Tobacco use is associated with increased complications after anterior cruciate ligament reconstruction. Am J Sports Med 44:99–104
Collins JE, Katz JN, Donnell-Fink LA, Martin SD, Losina E (2013) Cumulative incidence of ACL reconstruction after ACL injury in adults: role of age, sex, and race. Am J Sports Med 41:544–549
Colvin AC, Egorova N, Harrison AK, Moskowitz A, Flatow EL (2012) National trends in rotator cuff repair. J Bone Jt Surg Am 94:227–233
Crawford SN, Waterman BR, Lubowitz JH (2013) Long-term failure of anterior cruciate ligament reconstruction. Arthroscopy 29:1566–1571
Csintalan RP, Inacio MC, Funahashi TT, Maletis GB (2014) Risk factors of subsequent operations after primary anterior cruciate ligament reconstruction. Am J Sports Med 42:619–625
Dodwell ER, Lamont LE, Green DW, Pan TJ, Marx RG, Lyman S (2014) 20 years of pediatric anterior cruciate ligament reconstruction in New York State. Am J Sports Med 42:675–680
Dragoo JL, Padrez K, Workman R, Lindsey DP (2009) The effect of relaxin on the female anterior cruciate ligament: Analysis of mechanical properties in an animal model. Knee 16:69–72
Ellis HB, Matheny LM, Briggs KK, Pennock AT, Steadman JR (2012) Outcomes and revision rate after bone-patellar tendon-bone allograft versus autograft anterior cruciate ligament reconstruction in patients aged 18 years or younger with closed physes. Arthroscopy 28:1819–1825
Ensor KL, Kwon YW, Dibeneditto MR, Zuckerman JD, Rokito AS (2013) The rising incidence of rotator cuff repairs. J Shoulder Elbow Surg 22:1628–1632
Eriksson K, Anderberg P, Hamberg P, Lofgren AC, Bredenberg M, Westman I et al (2001) A comparison of quadruple semitendinosus and patellar tendon grafts in reconstruction of the anterior cruciate ligament. J Bone Jt Surg Br 83:348–354
Fairbank TJ (1948) Knee joint changes after meniscectomy. J Bone Jt Surg Br 30B:664–670
Faltstrom A, Hagglund M, Magnusson H, Forssblad M, Kvist J (2016) Predictors for additional anterior cruciate ligament reconstruction: data from the Swedish national ACL register. Knee Surg Sports Traumatol Arthrosc 24:885–894
Gaskill T, Pullen M, Bryant B, Sicignano N, Evans AM, DeMaio M (2015) The prevalence of symptomatic deep venous thrombosis and pulmonary embolism after anterior cruciate ligament reconstruction. Am J Sports Med 43:2714–2719
Gifstad T, Foss OA, Engebretsen L, Lind M, Forssblad M, Albrektsen G et al (2014) Lower risk of revision with patellar tendon autografts compared with hamstring autografts: a registry study based on 45,998 primary ACL reconstructions in Scandinavia. Am J Sports Med 42:2319–2328
Hanypsiak BT, Spindler KP, Rothrock CR, Calabrese GJ, Richmond B, Herrenbruck TM et al (2008) Twelve-year follow-up on anterior cruciate ligament reconstruction: long-term outcomes of prospectively studied osseous and articular injuries. Am J Sports Med 36:671–677
Kaeding CC, Pedroza AD, Reinke EK, Huston LJ, Consortium M, Spindler KP (2015) Risk factors and predictors of subsequent ACL injury in either knee after ACL reconstruction: prospective analysis of 2488 primary ACL reconstructions from the MOON cohort. Am J Sports Med 43:1583–1590
Kartus JT, Russell VJ, Salmon LJ, Magnusson LC, Brandsson S, Pehrsson NG et al (2002) Concomitant partial meniscectomy worsens outcome after arthroscopic anterior cruciate ligament reconstruction. Acta Orthop Scand 73:179–185
Khatib O, Onyekwelu I, Zuckerman JD (2014) The incidence of proximal humeral fractures in New York State from 1990 through 2010 with an emphasis on operative management in patients aged 65 years or older. J Shoulder Elbow Surg 23:1356–1362
Kiapour AM, Fleming BC, Proffen BL, Murray MM (2015) Sex influences the biomechanical outcomes of anterior cruciate ligament reconstruction in a preclinical large animal model. Am J Sports Med 43:1623–1631
Kim S, Bosque J, Meehan JP, Jamali A, Marder R (2011) Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Jt Surg Am 93:994–1000
Komatsuda T, Sugita T, Sano H, Kusakabe T, Watanuki M, Yoshizumi Y et al (2006) Does estrogen alter the mechanical properties of the anterior cruciate ligament? An experimental study in rabbits. Acta Orthop 77:973–980
Kowalchuk DA, Harner CD, Fu FH, Irrgang JJ (2009) Prediction of patient-reported outcome after single-bundle anterior cruciate ligament reconstruction. Arthroscopy 25:457–463
Laxdal G, Kartus J, Ejerhed L, Sernert N, Magnusson L, Faxen E et al (2005) Outcome and risk factors after anterior cruciate ligament reconstruction: a follow-up study of 948 patients. Arthroscopy 21:958–964
Lind M, Menhert F, Pedersen AB (2012) Incidence and outcome after revision anterior cruciate ligament reconstruction: results from the Danish registry for knee ligament reconstructions. Am J Sports Med 40:1551–1557
Lyman S, Koulouvaris P, Sherman S, Do H, Mandl LA, Marx RG (2009) Epidemiology of anterior cruciate ligament reconstruction: trends, readmissions, and subsequent knee surgery. J Bone Jt Surg Am 91:2321–2328
Maletis GB, Chen J, Inacio MC, Funahashi TT (2016) Age-related risk factors for revision anterior cruciate ligament reconstruction: a Cohort study of 21,304 patients from the Kaiser permanente anterior cruciate ligament registry. Am J Sports Med 44:331–336
Maletis GB, Inacio MC, Desmond JL, Funahashi TT (2013) Reconstruction of the anterior cruciate ligament: association of graft choice with increased risk of early revision. Bone Jt J 95(B):623–628
Maletis GB, Inacio MC, Funahashi TT (2013) Analysis of 16,192 anterior cruciate ligament reconstructions from a community-based registry. Am J Sports Med 41:2090–2098
Maletis GB, Inacio MC, Funahashi TT (2015) Risk factors associated with revision and contralateral anterior cruciate ligament reconstructions in the Kaiser Permanente ACLR registry. Am J Sports Med 43:641–647
Mall NA, Chalmers PN, Moric M, Tanaka MJ, Cole BJ, Bach BR Jr et al (2014) Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med 42:2363–2370
Memtsoudis SG (2009) Limitations associated with the analysis of data from administrative databases. Anesthesiology 111:449 (author reply 450–441)
Nwachukwu BU, McFeely ED, Nasreddine A, Udall JH, Finlayson C, Shearer DW et al (2011) Arthrofibrosis after anterior cruciate ligament reconstruction in children and adolescents. J Pediatr Orthop 31:811–817
Onyekwelu I, Khatib O, Zuckerman JD, Rokito AS, Kwon YW (2012) The rising incidence of arthroscopic superior labrum anterior and posterior (SLAP) repairs. J Shoulder Elbow Surg 21:728–731
Owens BD, Mountcastle SB, Dunn WR, DeBerardino TM, Taylor DC (2007) Incidence of anterior cruciate ligament injury among active duty U.S. military servicemen and servicewomen. Mil Med 172:90–91
Ponce BA, Cain EL Jr, Pflugner R, Fleisig GS, Young BL, Boohaker HA et al (2016) Risk factors for revision anterior cruciate ligament reconstruction. J Knee Surg 29:329–336
Salmon LJ, Russell VJ, Refshauge K, Kader D, Connolly C, Linklater J et al (2006) Long-term outcome of endoscopic anterior cruciate ligament reconstruction with patellar tendon autograft: minimum 13-year review. Am J Sports Med 34:721–732
Sanders TL, Kremers HM, Bryan AJ, Kremers WK, Stuart MJ, Krych AJ (2017) Procedural intervention for arthrofibrosis after ACL reconstruction: trends over two decades. Knee Surg Sports Traumatol Arthrosc 25:532–537
Scott DJ, Sherman S, Dhawan A, Cole BJ, Bach BR Jr, Mather RC 3rd (2015) Quantifying the economic impact of provider volume through adverse events: the case of sports medicine. Orthop J Sports Med 3:2325967115574476
Shelbourne KD, Gray T (2000) Results of anterior cruciate ligament reconstruction based on meniscus and articular cartilage status at the time of surgery. five- to fifteen-year evaluations. Am J Sports Med 28:446–452
Shelbourne KD, Gray T, Haro M (2009) Incidence of subsequent injury to either knee within 5 years after anterior cruciate ligament reconstruction with patellar tendon autograft. Am J Sports Med 37:246–251
Sherman SL, Lyman S, Koulouvaris P, Willis A, Marx RG (2008) Risk factors for readmission and revision surgery following rotator cuff repair. Clin Orthop Relat Res 466:608–613
Slauterbeck JR, Hardy DM (2001) Sex hormones and knee ligament injuries in female athletes. Am J Med Sci 322:196–199
Spindler KP, Wright RW (2008) Clinical practice. Anterior cruciate ligament tear. N Engl J Med 359:2135–2142
Stein T, Mehling AP, Welsch F, von Eisenhart-Rothe R, Jager A (2010) Long-term outcome after arthroscopic meniscal repair versus arthroscopic partial meniscectomy for traumatic meniscal tears. Am J Sports Med 38:1542–1548
Swartz SH, Cowan TM, DePue J, Goldstein MG (2002) Academic profiling of tobacco-related performance measures in primary care. Nicotine Tob Res 4(Suppl 1):S38–44
Tejwani SG, Chen J, Funahashi TT, Love R, Maletis GB (2015) Revision risk after allograft anterior cruciate ligament reconstruction: association with graft processing techniques, patient characteristics, and graft type. Am J Sports Med 43:2696–2705
Trojian TH, Collins S (2006) The anterior cruciate ligament tear rate varies by race in professional Women's basketball. Am J Sports Med 34:895–898
van Dijck RA, Saris DB, Willems JW, Fievez AW (2008) Additional surgery after anterior cruciate ligament reconstruction: can we improve technical aspects of the initial procedure? Arthroscopy 24:88–95
Viswanath P, Monaco NA, Lubahn JD (2015) Patient-related factors influencing ulnar-shortening osteotomy outcomes using the trimed dynamic compression plate. Orthopedics 38:e106–111
von Porat A, Roos EM, Roos H (2004) High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: a study of radiographic and patient relevant outcomes. Ann Rheum Dis 63:269–273
Wasserstein D, Khoshbin A, Dwyer T, Chahal J, Gandhi R, Mahomed N et al (2013) Risk factors for recurrent anterior cruciate ligament reconstruction: a population study in Ontario, Canada, with 5-year follow-up. Am J Sports Med 41:2099–2107
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Funding
The authors did not receive any financial support for the research, authorship, or publication of this article.
Ethical approval
IRB Approval was not applicable according to New York University Langone Medical Center Office of Science and Research Institutional Review Board as the study did not contain human subjects research.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Capogna, B.M., Mahure, S.A., Mollon, B. et al. Young age, female gender, Caucasian race, and workers’ compensation claim are risk factors for reoperation following arthroscopic ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 28, 2213–2223 (2020). https://doi.org/10.1007/s00167-019-05798-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05798-4