
Abstract
Purpose
The 11+ injury prevention program has been shown to decrease injury rate. However, few studies have investigated compliance and if it is correlated to time loss. The purpose of this study was to (1) analyze how differences in compliance may impact injury rate and (2) if compliance may impact time loss due to injury.
Methods
This study was a Level 1 prospective cluster randomized controlled trial conducted in NCAA men’s football (soccer) teams that examined the efficacy of the 11+ injury prevention program. The two outcome variables examined were number of injuries and number of days missed from competition. Twenty-seven teams (n = 675 players) used the 11+ program. Compliance, injuries and time loss were recorded. There were three compliance categories, low (LC, 1–19 doses/season), moderate (MC, 20–39 doses/season), and high (HC, > 40 doses/season).
Results
There was a significant difference among the groups for injuries, p = 0.04, pη2 = 0.23. The LC group [mean (M) = 13.25, 95% confidence interval (CI) 9.82–16.68, injury rate (IR) = 10.35 ± 2.21] had a significantly higher injury rate than the HC group (M = 8.33, 95%CI 6.05–10.62, IR = 10.35 ± 2.21), p = 0.02. The MC group (M = 11.21, 95%CI 9.38–13.05, IR = 8.55 ± 2.46) was not significantly different than the LC group, p = 0.29, but was significantly greater than the HC group, p = 0.05. When examined as a continuous variable, compliance was significantly negatively related to injury rate (p = 0.004). It was also significantly negatively related to number of days missed (p = 0.012).
Conclusions
When compliance was high, there was a significant reduction in injury and time loss. This evidence reinforces the importance of consistent injury prevention program utilization. Clinically, these findings have important implications when discussing the importance of consistent utilization of an injury prevention protocol in sport.
Level of evidence
Level 1—Randomized controlled trial (RCT).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Efforts to design and implement effective injury prevention and reduction programs in sport have been researched in the medical community for several decades [8, 11, 14, 17, 19, 22, 24, 25, 31]. The success of such community-based programs is multifactorial and are predicated upon the identification of the injury risk, analyzing the mechanism of injury, education of the coaches and players, the qualitative content of the injury prevention program, and the fidelity, compliance and adherence to the prescribed evidence-based program, where compliance refers to an individual conforming to a recommended intervention with respect to dosage, frequency and timing and adherence refers to a process that is influenced by environment, social context, personal knowledge, motivation, skill and available resources [9, 18, 20, 30]. Once a program has been scientifically vetted, the sports medicine community is compelled, from a public health perspective, to increase awareness that such programs do indeed exist. Clinicians must stress the critical nature of the inclusion, adoption and adherence to such programs into the existing sports training repertoire [4, 5, 7].
Despite the numerous publications that discuss the notion of injury prevention and reduction in sport, only a few studies have thoroughly discussed how the role of program integrity, adherence, and compliance may directly impact the efficacy of such programs [1, 13, 15, 23]. This is a critical aspect to analyzing the overall fidelity of an injury prevention program. In some research circumstances, if compliance was not deemed adequate, it is impossible to ascertain scientifically if it was a failing of the content of the actual prevention protocol, or if the compliance to the program was so inordinately low, that the neuromuscular training benefit of the prevention program was nullified, respectively [27, 28].
The aim of this study was to characterize differences in compliance in competitive male football players and to determine if variability in compliance to a neuromuscular training program (11+) would impact injury rate. Additionally, this study assessed if a correlation existed between high compliance to the 11+ program and a decrease in time lost due to injury during competitive play and training. This study is necessary to stress the importance of consistent utilization of injury prevention programs to address the steady rise in injury associated with sport.
Materials and methods
This study was a prospective cluster randomized controlled trial, which was conducted in 27 of 61 Division I and Division II NCAA men’s football (football) teams. Human ethics internal review board approval and informed consent was obtained through Quorum IRB (Seattle, WA, USA). Individual player consent was obtained and a documentation of coaching understanding was signed by each institution to ensure that there was a thorough understanding of the expectations of study participation.
Intervention
The 11+ is an injury prevention program designed as a dynamic warm-up program to address lower extremity injury incurred in the sport of football for athletes over the age of 14. It is a 20-min field-based program that consists of 15 exercises divided into three separate components: running exercises (8 min) that encompass cutting, change of direction, decelerating and proper landing techniques, strength, plyometric and balance exercises (10 min) that focus on core strength, eccentric control and proprioception, and running exercises (2 min) to conclude the warm-up and prepare the athlete for athletic participation. There are three progressions (level 1, level 2, level 3) that increase the difficulty for each respective exercise. This allows for both individual and team progression throughout the course of the competitive season. In this specific study, the FIFA 11+ program served as the intervention program over the course of one competitive collegiate football season [24].
Participants
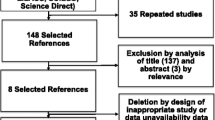
Sixty-five institutions were randomly assigned and completed the intervention study during one competitive football season (August–December): 34 control institutions (N = 850 athletes) and 31 intervention institutions (N = 775 athletes) with athletes between the ages of 18–25. Four Division II intervention teams discontinued the intervention (N = 100) secondary to time and personnel constraints, therefore, a per-protocol analysis was utilized. For the compliance aspect of the study, only the intervention teams that utilized the 11+ program as their dynamic warm-up completed the study were utilized (27 teams, N = 675) (Fig. 1).

Description of NCAA team randomization and study flow
Operational definitions
The following operational definitions were used during the injury data entry phase of the study. An injury was reported if a player was unable to participate fully in a scheduled game or training session. The player's return to play date was entered when the player was fully able to participate in a game or training session. All injuries were entered by Certified Athletic Trainers using The International Statistical Classification of Diseases and Related Health Problems (ICD-9) coding system. The severity of injury was defined utilizing the UEFA injury definition guidelines which was dictated by the amount of time missed from active participation (Table 1) [10].
Data collection
An internet-based injury surveillance data collection system was utilized (HealtheAthlete™, Overland Park, Kansas) by every enrolled institution in the study. Every athletic exposure, injury incurred, utilization of the FIFA 11+ program and compliance data was entered weekly by the team’s certified athletic trainer and verified by the research staff. Sixty-one institutions completed the study during the Fall, 2012 season (August–December): 34 control institutions (N = 850 athletes) and 27 intervention (N = 675 athletes) institutions. Only the intervention teams using the 11+ prior to games and training were analyzed for the compliance phase of the study. Upon the completion of the competitive football season, the injury, athletic exposure and compliance data entry was confirmed by each certified athletic trainer (ATC) and verified with their individual institution’s data collection system for accuracy and thoroughness. During the season, the research team monitored the team and individual compliance of the program weekly. If compliance within the IG was deemed less than optimal, an email was sent by a member of the research team to the individual institution. If the institution did not respond within 14 days, a research member contacted the team to encourage improvement in data entry and/or adherence to the program. At the completion of the season, compliance was analyzed and stratified by utilization consistency into tertile categories and by month of utilization and on a continuum.
Human ethics internal review board approval and informed consent was obtained through Quorum Internal Review Board (IRB # 26182/1) (Seattle, WA, USA).
Statistical analysis
This manuscript is based on an exploratory post hoc analysis of the data collected from the 11+ Intervention group (IG) in a larger randomized controlled trial [24]. All statistical analyses were conducted utilizing IBM SPSS for Windows version 23 (Armonk, NY). Descriptive and inferential tests were used to compare levels of compliance within the IG, including t tests, χ2 tests, and generalized linear regression models (GLM), with logit link function and Poisson distribution for injury count data between groups. Descriptive data for compliance, exposures and injury rates (IR) are presented as means (M) with standard errors (SE) and 95% confidence intervals (CI). P values of 0.05 or less were considered significant. The summary measure for injury rate (IR) was calculated according to the formula: IR = n/e, where n is defined as the number of injuries during the data collection period and e is the number of exposures expressed in number of games or trainings participated in. Relative rate ratios (RR), with their associated 95% confidence intervals, were calculated using the injury incidence for each compliance group. Analyses of variance (ANOVAs) were utilized to analyze the main effect of compliance (three levels) on both injury rate and time loss due to injury. All effects were deemed statistically significant with a p value of p < 0.05. Tukey’s post hoc analysis was utilized to analyze within group differences when a main effect was identified. χ2 tests were used to compare categorical variables within the compliance subgroups. A GLM regression model was used to analyze compliance as a continuous variable with respect to injury rate and days lost due to injury.
Cohen’s d effect sizes were calculated and defined when compared to the following: small d = 0.20, medium d = 0.5, and large d = 0.8. Power calculations were performed, a priori, using preliminary data and G*Power software version 3.1.0 (Universität Düsseldorf, Düsseldorf, Germany). Using a generalized linear model with Tweedie distribution and logit link function, with p value = 0.05 and power = 0.80, it was determined that a relative risk of 1.1 could be detected with a total sample size of 125.
Results
Of the thirty-one teams in the intervention cohort, 27 teams (N = 675) completed the research study and, thus, compliance was analyzed using a per-protocol analysis. Injuries and time loss due to injury during the entire season were tracked within this cohort.
Team compliance
Twenty-seven intervention teams completed the FIFA 11+ injury prevention program over the course of the season (August through late November or early December, depending on the success of the team in the NCAA tournament). The total number of utilizations of the FIFA 11+ equated to 886 sessions (mean 32.8 ± 12.1 sessions, range 11–64, median = 32). There were 1304 overall team exposures in the IG (405 games and 899 training sessions) over the course of the season, translating into an average of 2.2 FIFA 11+ utilizations over the course of the season per week. Compliance was determined to be low for teams using the program ≤ 1 time per week (LC: 1–19 doses/season), moderate for > 1 and < 2 utilizations per week (MC: 20–39 doses/season) or high for ≥ 2 utilizations per week (HC: >39 doses per season,), predicated on a 19.4-week season. Four teams were categorized in the low tertile (15.8 ± 3.6 doses/season, range 11–19 days, median = 16.5), 14 teams in the moderate tertile (29.4 ± 5.9 doses/season, range 21–39 days, median = 29.5), and 9 teams were categorized in the high tertile (45.8 ± 7.5 doses/season, range 40–64 days, median = 43) (Table 2). The utilization in the first half of the season (August and September) exceeds that of the utilization in the second half of the season (October, November and December) secondary to the fact that many teams’ season were concluded in mid-November after being eliminated from conference tournament play. The decreased dosage of FIFA 11+ in the second half of the season does not necessarily reflect a decrease in utilization of the program (Table 2).
Compliance and injury rate
There were 53 injuries in 4 LC teams (M = 13.3, IR = 10.34 ± 2.2, RR = 1.6(1.3–2.1), p < 0.001), 157 injuries in 14 MC teams [M = 11.2, IR = 8.6 ± 2.5. RR = 1.3 (1.1–1.7), p = 0.009] and 75 injuries in 9 HC teams (M = 8.3, IR = 6.4 ± 2.7) (Table 2). There was a main effect within the groups for injury rate, f(2,24) = 3.6, p = 0.043, pη2 = 0.231. Upon post hoc analysis, the LC group (M = 13.3, 95% CI 9.8–16.7, IR = 10.4 ± 2.2) had a significantly higher injury rate than the HC group (M = 8.3, 95% CI 6.1–10.6, IR = 6.4 ± 2.7), p < 0.001. The MC group (M = 11.2, 95% CI 9.4–13.1, IR = 8.6 ± 2.5) was not significantly different than the LC group, p = 0.291, but was significantly greater than the HC group, p = 0.009. When examined as a continuous variable, compliance was significantly negatively related to injury rate (b = − 1.6, t = − 3.2, p = 0.004, R2 = 0.029) (Table 3; Fig. 2).

Injury rates in relationship to compliance with the FIFA 11+ program. The bars represent the level of compliance: Low compliance = 1–19 utilizations (n = 4 teams), moderate compliance = 20–39 utilizations (n = 14 teams) and high compliance = > 39 utilization (n = 9 teams) of the FIFA 11+ (error bars depict standard deviation), p = 0.004
Compliance and time loss due to injury
Compliance was also significantly negatively related to number of days missed, which served as a proxy for severity of injury (b = − 2.8, t = − 2.7, p = 0.012, R2 = 0.23). The LC teams reported 9.6 ± 2.8 days lost to injury compared to 11.9 ± 5.7 for the MC teams and 7.6 ± 4.8 days lost for the HC teams (F = 3.35, p = 0.012) (Fig. 3). Within the high compliance group, there was a lower injury rate and a decreased severity of injury, demonstrated by a decrease in time loss due to injury (Table 4; Fig. 3).

Team compliance compared to time lost due to injury. Utilization of FIFA 11+ stratified by team compliance (low, moderate and high) compared to time lost due to injury. The high compliance teams had significantly fewer days lost due to injury compared to the MC and LC compliance groups (p = 0.012)
There was a significant difference among the compliance groups on the average number of days missed per injury by team, f(2,24) = 3.35, p = 0.05, pη2 = 0.218. It should be noted that the partial eta squared (pη2) was equal to 0.218, meaning that the effect for the group differences recorded in days lost due to injury per team accounted for 21.8% of the variance plus error variance. Furthermore, there was a similar pattern noted when analyzing compliance compared to days lost to injury and compliance compared to injury rate. The LC group had the second highest number of days missed (M = 127.3 ± 54.1, 95% CI 60.0–194.6) and the MC group reported the highest number of days missed (M = 133.3 ± 76.6, 95% CI 97.3–169.2). The HC group had the fewest days missed per team (M = 63.2 ± 46.1, 95% CI 18.4–108.1) and fewest days lost per injury (M = 7.6 ± 4.8, 95% CI 8.2–12.5) (Table 4). Additionally, there was one potential outlier in the data for the MC group; a contact ACL/meniscal injury that occurred in the first game of the season resulting in 106 days of time loss (within the parameters of the data collection). Since we hypothesize that the benefit of performing an injury prevention program is not realized in the first week of utilization, we performed a secondary analysis with this one injury removed from the dataset. Once removed, there is a significant difference amongst compliance groups, with the HC having significantly fewer days lost to injury than both LC, p = 0.009, and MC, p = 0.018 groups, respectively.
Discussion
The most important finding of this present study, that corroborated findings by previous researchers, is high compliance to the 11+ injury prevention program demonstrated lower injury rates throughout the competitive season [26,27,28]. There is an inverse correlation between compliance and injury rate and severity of injury; which was reflected in fewer days lost due to injury. High compliance to the 11+ program resulted in fewer injuries and decreased severity of injury.
Compliance and injury risk
The teams with high compliance (HC) completed the FIFA 11+ nearly three times as frequently as the LC teams and nearly one and one-half times as frequently as the MC teams. When the exposure–response relationship was analyzed, the preventative impact of the program seemed to improve as the number of doses increased throughout the season. The injury rate was lowest in the HC group compared to the MC and the LC groups (Table 2). Thus, a statistically significant inverse relationship exists between compliance and injury rate; the more compliant the teams were to utilizing the FIFA 11+ program, the lower the injury rate reported. In addition, when the entire intervention group was compared to a control group that did not utilize the 11+ program, there was an overall injury reduction of 46.1% [24]. However, when the HC group was compared to the control group, there was a 57.5% decrease in overall injury rate. This supports the notion that as the dosage of the FIFA 11+ increases over the course of the season, the preventative benefit also increases.
The overall utilization of the FIFA 11+ was 32.8 ± 12.1 doses per season and 2.0 ± 0.7 doses per week. The recommended dosage was 2 sessions per week. Despite the LC and MC teams performing the program fewer times than the recommended dosage, both groups still experienced a reduction in injuries and fewer days lost to injury compared to the control group [24]. Recent systematic reviews of the FIFA 11+ program noted that athletes with high compliance to the FIFA 11+ injury prevention program resulted in a 35–39% reduction in injury risk [3, 29]. In addition, the athletes using the FIFA 11+ program demonstrated significant improvements in neuromuscular and motor performance when the structured warm-up was utilized at least 1.5 times per week [3]. This supports the premise that FIFA 11+ program is indeed an effective manner unto which football-related injury might be prevented.
Compliance and time lost due to injury
The high compliance group experience fewer days lost to injury per team and fewer days lost to each individual injury compared to the low and moderate compliance groups. When compliance was analyzed as a continuous variable, this was also a statistically significant finding. Earlier research articles that demonstrated similar findings, have corroborated this evidence. In one of the initial studies analyzing the effectiveness of the FIFA11+ program in young female football players, there was a significantly lower risk of injuries overall overuse injuries, and severe injuries in the IG compared to the CG [25]. In a small cohort study conducted in men’s football over one season, the IG demonstrated a reduction in the relative risk of lower extremity injury of 72% and time lost due to lower extremity injury (p < 0.01) [12]. These studies, in addition to others that have utilized alternative neuromuscular training programs, have shown proven efficacy in reduction of injury rate, severity of injury and time lost due to injury [6, 11, 16, 17, 19]. However, despite very thorough implementation strategies, compliance continues to be an obstacle in optimal program adherence [4].
The compliance conundrum
Despite very promising research detailing the efficacy of the FIFA 11+ in male and female football athletes [12, 22, 24, 25], compliance and program adherence by players and coaches continues to be problematic across sport. Compliance and adherence to injury prevention protocols has been discussed in the literature, but acceptable levels of program adherence in sport continue to elude sports medicine researchers [18, 26,27,28]. In a recent survey of youth male football teams analyzing the awareness and utilization of the FIFA 11+ program, 61% of respondents had heard of the FIFA 11+ program, but only 28% reported using the program in some form (fully or modified versions). Interestingly, when the respondents were queried on who ultimately holds responsibility for injury prevention efforts, there was significant variability in the responses: 35% indicated that the head coach held the ultimate responsibility, 24% the player, and 24% the fitness coach [21]. Bahr et al. reported that despite the fact that 88% of Champions League and Norwegian Premier League teams being aware of the existence of hamstring injury prevention methodology, only 16 teams (10.7%) were fully compliant and 9 teams (6%) were partially compliant with the proposed intervention. This resulted in a startling 225 teams (83.3.%) of the teams being deemed completely non-compliant [2]. This research elucidates the magnitude of the work that stands before the sports medicine community. This study has important implications when discussing the importance of consistent utilization of an injury prevention protocol in sport.
This study was conducted in male football (soccer) players and only was conducted over the course of one season. The NCAA collegiate football (soccer) season only extends from August to December, and is significantly shorter than other competitive and professional seasons around the world. Unannounced site visits were not conducted during this data collection due to the vast geographic expanse of the study population (entire United States). Due to the nature of the NCAA substitution rule, the researchers analyzed exposure using athletic exposure versus playing hour as a unit of analysis. The researchers were only able to analyze compliance by team, and not by individual participant. Individual compliance to the program was not collected during the data collection phase. The low compliance group was limited to four teams and the 11+ utilizations ranged from 11 to 19. This may represent inter-team differences, which can affect the overall comparison between groups. This was overcome by including the analysis of compliance on a continuum.
Conclusions
The athletes utilizing the FIFA 11+ as their dynamic warm-up program with high compliance demonstrated a significant reduction in injury rate and time loss due to injury. The higher the consistency in the adherence to the program, the greater the benefit to the individual athlete with respect to decreased injury risk and severity of injury. This corroborates the research finding found in earlier studies conducted in men and women, globally [22, 25,26,27]. As researchers continue to revise and improve injury prevention and reduction efforts, there should be equal emphasis placed on analyzing optimal strategies to encourage optimal implementation and utilization by athletes, coaches and medical staffs universally.
References
Arnason A, Engebretsen L, Bahr R (2005) No effect of a video-based awareness program on the rate of soccer injuries. Am J Sports Med 33:77–84
Bahr R, Thorborg K, Ekstrand J (2015) Evidence-based hamstring injury prevention is not adopted by the majority of Champions League or Norwegian Premier League football teams: the Nordic Hamstring survey. Br J Sports Med 49:1466–1471
Barengo NC, Meneses-Echavez JF, Ramirez-Velez R, Cohen DD, Tovar G, Bautista JE (2014) The impact of the FIFA 11+ training program on injury prevention in football players: a systematic review. Int J Environ Res Public Health 11:11986–12000
Bizzini M, Junge A, Dvorak J (2013) Implementation of the FIFA 11+ football warm up program: how to approach and convince the Football associations to invest in prevention. Br J Sports Med 47:803–806
Blakely C, Mayer J, Gottschalk R, Schmitt N, Davidson W, Riotman D et al (1987) The fidelity-adaptation debate: implications for the implementation of public sector social programs. Am J Com Psychol 15(3):253–268. https://doi.org/10.1007/BF00922697
Caraffa A, Cerulli G, Projetti M, Aisa G, Rizzo A (1996) Prevention of anterior cruciate ligament injuries in soccer. A prospective controlled study of proprioceptive training. Knee Surg Sports Traumatol Arthrosc 4(1):19–21
Carroll C, Patterson M, Wood S, Booth A, Rick J, Balain S (2007) A conceptual framework for implementation fidelity. Implement Sci 2:40
Ekstrand J, Gillquist J, Lysholm J, Moller M, Oberg B (1983) Considerably decreased amount of soccer injuries after introduction of a preventive program. Lakartidningen 80:1803–1804 (1809)
Fortington LV, Donaldson A, Lathlean T, Young WB, Gabbe BJ, Lloyd D et al (2015) When ‘just doing it’ is not enough: assessing the fidelity of player performance of an injury prevention exercise program. J Sci Med Sport 18:272–277
Fuller C, Ekstrand J, Junge A et al (2006) Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med 40:193–201
Gilchrist J, Mandelbaum BR, Melancon H, Ryan GW, Silvers HJ, Griffin LY et al (2008) A randomized controlled trial to prevent noncontact anterior cruciate ligament injury in female collegiate soccer players. Am J Sports Med 36:1476–1483
Grooms DR, Palmer T, Onate JA, Myer GD, Grindstaff T (2013) Soccer-specific warm-up and lower extremity injury rates in collegiate male soccer players. J Athl Train 48:782–789
Hagglund M, Atroshi I, Wagner P, Walden M (2013) Superior compliance with a neuromuscular training programme is associated with fewer ACL injuries and fewer acute knee injuries in female adolescent football players: secondary analysis of an RCT. Br J Sports Med 47:974–979
Hagglund M, Walden M, Atroshi I (2009) Preventing knee injuries in adolescent female football players—design of a cluster randomized controlled trial [NCT00894595]. BMC Musculoskelet Disord 10:75
Heidt RS Jr, Carlonas RL, Traub JA, Tekulve FX (2000) Avoidance of soccer injuries with preseason conditioning. Am J Sports Med 28:659–662
Hewett TELT., Riccobene JV, Noyes FR (1999) The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med 27:699–706
Mandelbaum BR, Silvers HJ, Watanabe DS, Knarr JF, Thomas SD, Griffin LY et al (2005) Effectiveness of a neuromuscular and proprioceptive training program in preventing anterior cruciate ligament injuries in female athletes: 2-year follow-up. Am J Sports Med 33:1003–1010
McKay CD, Verhagen E (2016) ‘Compliance’ versus ‘adherence’ in sport injury prevention: why definition matters. Br J Sports Med 50:382–383
Myklebust G, Engebretsen L, Braekken IH, Skjolberg A, Olsen OE, Bahr R (2007) Prevention of noncontact anterior cruciate ligament injuries in elite and adolescent female team handball athletes. Instr Course Lect 56:407–418
Nilsen P (2004) What makes community based injury prevention work? In search of evidence of effectiveness. Injury Prev 10:268–274
O’Brien J, Finch CF (2017) Injury prevention exercise programs for professional soccer: understanding the perceptions of the end-users. Clin J Sport Med 27:1–9
Owoeye OB, Akinbo SR, Tella BA, Olawale OA (2014) Efficacy of the FIFA 11+ warm-up programme in male youth football: a cluster randomised controlled trial. J Sports Sci Med 13:321–328
Pfeiffer RP, Shea KG, Roberts D, Grandstrand S, Bond L (2006) Lack of effect of a knee ligament injury prevention program on the incidence of noncontact anterior cruciate ligament injury. J Bone Joint Surg Am 88:1769–1774
Silvers-Granelli H, Mandelbaum B, Adeniji O, Insler S, Bizzini M, Pohlig R et al. (2015) Efficacy of the FIFA 11+ Injury Prevention Program in the Collegiate Male Soccer Player. Am J Sports Med. https://doi.org/10.1177/0363546515602009
Soligard T, Myklebust G, Steffen K, Holme I, Silvers H, Bizzini M et al (2008) Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ 337:a2469
Soligard T, Nilstad A, Steffen K, Myklebust G, Holme I, Dvorak J et al (2010) Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br J Sports Med 44:787–793
Steffen K, Emery CA, Romiti M, Kang J, Bizzini M, Dvorak J et al (2013) High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: a cluster randomised trial. Br J Sports Med 47:794–802
Steffen K, Myklebust G, Olsen OE, Holme I, Bahr R (2008) Preventing injuries in female youth football—a cluster-randomized controlled trial. Scand J Med Sci Sports 18:605–614
Thorborg K, Krommes KK, Esteve E, Clausen MB, Bartels EM, Rathleff MS (2017) Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: a systematic review and meta-analysis of the FIFA 11 and 11+ programmes. Br J Sports Med 51:562–571
Tilson HH (2004) Adherence or Compliance? Changes in Terminology. Ann Pharmacother 38:161–162
Walden M, Atroshi I, Magnusson H, Wagner P, Hagglund M (2012) Prevention of acute knee injuries in adolescent female football players: cluster randomised controlled trial. BMJ 344:e3042
Funding
This study was funded by The Fédération Internationale de Football Association (FIFA).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
One of the authors (HJS-G) received a PhD Research Grant from Simbex, Inc (less than 10,000 USD); and is a research consultant to Major League Soccer’s M-MARC program (less than 10,000 USD) unrelated to this work. One of the authors (AA) received a Grant from the National Institutes of Arthritis and Musculoskeletal and Skin Diseases (R01-AR048212) (less than 10,000 USD) and the Foundation for Physical Therapy–Promotion of Doctoral Studies I Scholarship (less than 10,000 USD). One of the authors (BRM) received funding from FIFA to support the completion of this study (see below); and is a consultant to Athrex, RTI, Exactech, and DePuy Mitek. The institution (Santa Monica Orthopaedic Group) of one or more of the authors (HJS-G, BRM) has received funding from FIFA’s (Fédération Internationale de Football Association) F-MARC Program (2012) for the initial publication (10,000–100,000 USD).
Ethical approval
This study received Internal Review Board (IRB) and Human Ethics approval.
Informed consent
Informed consent was obtained through Quorum Internal Review Board (IRB # 26182/1) (Seattle, WA, USA).
Rights and permissions
About this article

Cite this article
Silvers-Granelli, H.J., Bizzini, M., Arundale, A. et al. Higher compliance to a neuromuscular injury prevention program improves overall injury rate in male football players. Knee Surg Sports Traumatol Arthrosc 26, 1975–1983 (2018). https://doi.org/10.1007/s00167-018-4895-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-018-4895-5