
Abstract
Purpose
Clinical research in the area of anterior cruciate ligament (ACL) injury has shown substantial growth during the last decade. This was accompanied by the establishment of a wide range of outcome measures used to address the demands of clinical studies. The aim of this study was to evaluate outcome measures reported by highly cited level I trials in ACL research and identify factors influencing citation metrics.
Methods
The database of the Institute for Scientific Information (ISI) was utilized to screen journals under the subject categories “Orthopaedics”, “Sports Sciences”, “Radiology” and “General medicine” for the 50 most cited level I ACL trials based on predefined inclusion criteria. Metadata, citation metrics and outcome measures were extracted for each article. Frequencies of reported outcome measures were calculated, and a multiple linear regression model applied to identify factors influencing citation metrics.
Results
Two independent outcome measures demonstrated an influence on acquisition of citations including: 1—report of the pivot-shift test and 2—inclusion of the Knee Injury and Osteoarthritis Outcome (KOOS) score. Furthermore, highly cited ACL trials frequently reported KT-1000 measures of anterior translation, range of motion (ROM), graft failure, Lysholm, Tegner and subjective International Knee Documentation (IKDC) scores.
Conclusion
This analysis reflects on the outcome measures utilized in highly cited level I trials impacting the field of ACL research. It also identifies factors likely to influence acquisition of citations. This is of both clinical and academic relevance when choosing appropriate measures for post-operative outcome evaluation after ACL surgery.
Level of evidence
I.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anterior cruciate ligament (ACL) injury has attracted substantial interest of clinicians during the last decade, allowing it to occupy a spotlight position in the field of sports traumatology [1]. The fundamental role of the ACL as a stabilizer of the knee joint together with the posttraumatic consequences of its insufficiency fuelled this trend with increasing evidence [4, 8, 17].
The rapid growth of the field was accompanied by a rising number of questions with which clinicians were confronted, resulting in a corresponding increase in research activity [3, 5, 9, 16, 18–24]. Changes in treatment algorithms were experienced when initial historical techniques of primary suturing of the ACL were abandoned after proved a failure, allowing for a shift towards reconstructive techniques to restore functional anatomy [6, 7, 22]. A steep increase in the volume of published material related to ACL reconstruction was subsequently perceived. Between the years 1980 and 1999, 1328 articles containing the words “ACL reconstruction” or “Anterior cruciate ligament reconstruction” in their titles were published in the scientific literature. This number increased to 10,948 articles published between the years 2000 and 2015 (based on figures from the Institute for Scientific Information (ISI Web of Knowledge).
Careful selection of outcome measures is of fundamental importance for adequate demonstration of effects in clinical studies [10]. The process could become challenging when selection from a large pool of available measures is necessary. More than 54 scores have been designed alone for the ACL deficient knee and applied in the literature [14]. There is a lack of investigations on the most frequently applied scores and outcome measures in ACL studies with high impact in the field. Such studies would aid clinicians and researchers in selecting appropriate outcome measures for patient follow-up and monitoring.
Prompted by the points mentioned above, the aim of this study was to (1) Identify and evaluate the 50 most cited level I randomized trials in the field of ACL research. (2) Determine the outcome measures reported by these studies. (3) Identify factors influencing citation metrics.
Materials and methods
The annual Journal Citation Report ® of the Institute for Scientific Information (ISI) was utilized for identification of journals under the subject categories “Orthopaedics”, “Sports Sciences”, “Radiology” and “General medicine”. Two hundred and eighty-nine journals (all 72 orthopaedic journals, all 125 radiology journals, all 81 journals of sport sciences and 11 of the general medical journals with the highest impact factors) were identified and selected for further manual allocation of highly cited trials in the field of ACL research. The search was performed on the 4th and 5th of January 2016.
Allocation of articles and eligibility criteria
The ISI database comprising “MEDLINE”, “Web of Science core collection”, “BIOSIS previews” and “SciELO Citation Index” was employed for the generation of article lists within the selected journal categories regardless of language, which comprised the first step of the search process. The second step was based on article pre-selection, intended to identify randomized trials. The following keywords were employed: “random”, “randomly”, “randomized”, “randomised”, “randomizing” and “randomising”. Articles cited less than 50 times were excluded, given the assumption that the 50th article to be included in the analysis would posses more than 50 citations. In the third step of the search process, potentially relevant titles and abstracts were manually screened to exclude studies with obvious irrelevance to the ACL or incompatibility of study design (Fig. 1).

Flow chart showing the process of allocation of relevant studies. *: “random”, “randomly”, “randomized”, “randomised”, “randomizing”, “randomising”
Finally, the full texts of remaining articles were evaluated for eligibility by two independent epidemiologically trained investigators based on the following inclusion criteria:
-
1.
The primary research question was set to address an injury or pathology of the ACL.
-
2.
The study design complies with the definition criteria of a randomized trial based on the Oxford Centre for Evidence Based Medicine (CEBM) definition [12].
-
3.
The study had a lost to follow-up rate of no more than 20 %, and a narrow confidence interval, to assure quality standards of a level I study.
Exclusion criteria included:
-
1.
Articles dealing with multiple ligament injuries or with primary focus on meniscal pathology.
-
2.
Non-clinical studies regardless of type.
-
3.
Lower-quality randomized trials that would not comply with the standards of a level I study.
-
4.
Systematic reviews and meta-analyses.
Data extraction
The 50 most cited eligible articles were subject for extraction of the following data: year of publication, geographic origin, number of citations, current citation rate (citations in the year 2014), citation density (citations/article age), authorship and outcome measures. The articles were further evaluated for quality using the Jadad scale [13] and the Cochrane risk of bias tool (addressing 7 domains namely sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting and “other issues”) [11]. The area of research and the conclusion of each study were noted. Disagreements between investigators were solved by consensus with the involvement of a third investigator.
Statistical analysis
Normally distributed data were presented as mean ± standard deviation. Analysis of variance (ANOVA) was performed for comparison between means. Univariate analysis was conducted to identify factors influencing article citation metrics, and multiple linear models subsequently performed for adjustments. The Mann–Kendall trend test was applied for time-dependent trends. Qualitative evaluation of intervention superiority was undertaken, based on the outcome of each included trial when homogeneity was present. Cohen’s Kappa coefficient was applied for inter-rater agreement. A p value of <0.05 was considered statistically significant.
Results
All 50 articles were published in eight orthopaedic journals, one sports sciences journal and one general medical journal (Tables 1, 2), between the years 1987 and 2012 (mean 2002 ± 6). They originated from 16 countries, mostly the USA and Sweden (nine articles each), followed by Japan (seven articles) (Table 2). Citations per article ranged from 56 to 223 (mean 122.2 ± 54.7). There were 9 authors each represented by two trials in the list. Ten of the 50 studies (20 %) were collaborative.
Quality assessment
The mean Jadad score for all articles was 2.2 ± 0.9 (range 1–5). The risk of bias was lowest amongst studies for the domain “completion of outcome data” (44/50). On the other hand, a high risk of bias was most common for the domain “selective reporting” (19/50). Insufficient reporting was found for the domain “blinding of participants and personnel” (Fig. 2).

Cochrane risk of bias assessment of all studies
Inter-rater agreement
The inter-rater agreement for inclusion of articles was high (κ 0.91, confidence interval (CI) 0.84–0.98). The agreement on the items of the Cochrane risk of bias tool was highest for the domain “sequence generation” (κ 0.77, CI 0.61–0.83), followed by “allocation concealment” (κ 0.58, CI 0.40–0.76). Lower inter-rater agreement was present for the domains “incomplete data” (κ 0.37, CI 0.29–0.46), blinding (κ 0.27, CI 0.18–0.37), “other sources of bias” (κ 0.34, CI 0.23–0.45), “overall risk of bias” (κ 0.30, CI 0.16–0.44) and “selective reporting” (κ 0.09, CI −0.07–0.22).
Citation metrics
Three factors showed to influence total citation count, namely article age, citation density and a North American origin of the article. The rate at which a trial was currently being cited showed to be influenced by the overall citation density of an article and the inclusion of the Knee Injury and Osteoarthritis Outcome Score (KOOS) as an outcome measure. Citation density itself was shown to be influenced by the inclusion of the pivot-shift test as an outcome measure. Table 3 illustrates the results of the multiple linear regression models. The Jadad quality score did not show to have an influence on citation count, citation density or current citation rate (p = n.s). There was no significant correlation between increasing article age and citation count (p = n.s). However, there was a significant negative correlation between current citation rates, citation density and age (r = −0.43, p = 0.002 and r = −0.60, p < 0.001, respectively) (Fig. 3).

Graph representing the correlation between age (x-axis), citation density (y-axis blue) and current citation rate (y-axis res). R: correlation coefficient
Outcome measures
There were ten frequently reported outcome parameters, each constituting an outcome measure in more than 2 of the 50 highly cited trials, namely KT-1000 measures of anterior translation (n = 38), IKDC subjective score (n = 28), pivot shift (n = 21), Lysholm score (n = 21), reporting of graft failure (n = 17), range of motion (ROM) n = 17, Tegner score (n = 15), IKDC objective (n = 6), Cincinnati score (n = 6) and KOOS score (n = 6) (Fig. 4).

Radar chart illustrating the frequency of reports per outcome measure on each of the axis
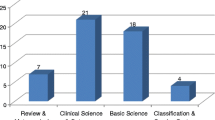
Areas of research
The 50 most cited trials covered six core research topics, mainly graft selection (n = 18), single- versus double-bundle graft utility (n = 10), rehabilitation (n = 9), surgical technique (n = 8), indication for surgery (n = 4) and injury prevention (n = 1).
Of the 18 articles related to graft selection, 16 dealt with the primary question: bone-patella tendon-bone (BPTB) versus hamstrings grafts. Qualitative illustration of the results is shown in Fig. 5. A general similarity in outcome between both graft types, however, the studies showed a tendency towards favouring hamstring graft reconstruction with regard to donor site morbidity. Laxity and pivot-shift outcome results were favoured in BPTB graft groups in 3/16 and 3/8 studies, respectively.

Graph presenting a qualitative illustration of the outcome of the 16 studies comparing bone-patella tendon-bone (BPTB) to hamstring grafts. The x-axis represents the outcome measures. The upper portion of the y-axis is BPTB—graft favouring, the lower portion hamstring-graft favouring. The size of the diamonds demonstrates the number of papers (also in numbers)
Ten articles dealt with the question double-bundle versus single-bundle techniques. More than half the articles reporting on laxity (4/8 studies), pivot shift (6/8 studies) and graft failure (3/5 studies) favoured the double-bundle technique (Fig. 6).

Graph presenting a qualitative illustration of the outcome of the 10 studies comparing single-bundle and double-bundle techniques. The x-axis represents the outcome measures. The upper portion of the y-axis is double-bundle favouring, the lower portion single-bundle favouring. The size of the diamonds demonstrates the number of papers (also in numbers)
Four trials dealt with the question of surgical versus non-surgical treatment of an ACL rupture, all originating from Sweden. The first article by Sandberg et al. in 1987 demonstrated the only difference of an increased abundance of a positive pivot-shift test in conservatively treated ACL ruptures, compared to ACL sutured knees. The second article was published by Andersson et al. in 1989 comparing three groups undergoing different treatment strategies (1) repair of all major injuries including suture and augmentation of the ACL using a strip of the iliotibial band, (2) ACL repair without augmentation and (3) repair of all major injuries except the ACL. The results favoured the group receiving augmented ACL repair in terms of stability of the knees and the need for subsequent meniscal repair. The third trial was published by Meunier et al. in 2007 proving the significant benefit of ACL repair in reducing secondary meniscal lesions. The fourth article by Frobell et al. published in 2010 showed that 40 % of patients receiving initial conservative treatment required ACL reconstruction within 2 years and demonstrated a higher need for subsequent meniscal surgery in the primary rehabilitation group compared to an early ACL reconstruction group.
Discussion
The most important finding of this study was that the inclusion of the pivot-shift test and the KOOS score in an ACL trial would influence acquisition of citations
It is apparent that there is a change in citation practice, as it was shown in this study that the rate at which an ACL trial is currently being cited is determined by factors differing from those influencing the total citation count (Table 3); a North American origin of an article no longer shows an influence on its likelihood of being cited.
The Jadad quality score of studies did not show to influence any of the citation metrics
The outcome measure that is frequently being reported in more recent trials is the pivot-shift test. This may be seen as a corresponding result to the increase in clinical and academic focus on restoring functional anatomy and rotational stability. There are, however, associated challenges due to the variety of described testing techniques and lack of consensus regarding the ideal testing manoeuvre [15]. This highlights the need for establishing consensus over a reproducible standardized testing manoeuvre that can ideally be quantitatively assessed. The results of this study do show that reporting of pivot shift is likely to influence acquisition of citations, emphasizing the need to include this outcome measure in all clinical studies.
It is to be affirmed that despite age being a factor influencing total citation count, increasing article age does not guarantee citations, as citation density and rates were shown to drop as the article ages. This underlines the fact that it is the quality of an article based on multiple factors, which determines its likelihood of being cited in the future.
The phenomenon of acquiring high citation counts is considered the natural consequence of the decision of researchers to cite one article [2]. The underlying rationale for this phenomenon was postulated in explanatory models by scientometric researchers based on both quality and visibility dynamics of citation practices [2]. Therefore, a high citation count represents a reflection of at least a methodological agreement amongst peers.
This in turns highlights the importance of the frequently reported outcome measures in highly cited ACL trials. The primary implication of these findings is on the planning of clinical study designs. Based on the results of this study, the inclusion of the following outcome measurers in ACL outcome studies can be recommended: (1) The use of KT-1000 for measurement of anterior translation. (2) Reporting of pivot-shift test results. (3) Inclusion of the subjective IKDC, Lysholm, Tegner and KOOS scores. (4) ROM and (5) Reporting of graft failure (Fig. 4). Both the pivot-shift test and KOOS score are likely to positively influence acquisition of citations. This recommendation should be used as a guide for planning ACL outcome studies of all types, since all therapeutic clinical studies, regardless of study design, ranging from level IV to level I evidence, mandate sufficient selection of outcome measures.
It is fair to mention that results deduced from the included studies are biased towards conclusions from highly cited articles, thereby accounting for a limitation of this type of analysis as a meta-study. However, the primary aim of this study was not to provide a meta-analysis, but to reflect on the conclusions of highly cited impacting studies dealing with the most common questions in the field of ACL research. Due to the dependence of the primary research question on citation metrics, the ISI Web of Knowledge database was utilized solely, being the only source for retrieving accurate citation information. Despite being comprehensive, the risk of missing articles cannot be excluded, therefore accounting for a further limitation of the study. It is also necessary to point out that recent qualitative trials that have not yet gathered sufficient citations to enter the list were not included in the study.
The results of this study should provide an aid for clinicians and researchers when choosing appropriate outcome measures to monitor patients postoperatively after an ACL intervention.
Conclusion
The vast increase in ACL research during the last decade led to the establishment of many measures used for outcome evaluation in clinical research. Based on the analysis of highly cited level I research, it can be recommended that an ACL outcome study should include KT-1000 measurements of anterior translation, should report on pivot shift, and include the subjective IKDC, Lysholm, Tegner and KOOS scores, ROM and report on graft failure. The inclusion of the pivot-shift test and KOOS scores is likely to influence whether or not an article will be cited in the future.
References
Ahmad SS, Evangelopoulos DS, Abbasian M, Roder C, Kohl S (2014) The hundred most-cited publications in orthopaedic knee research. J Bone Joint Surg Am 96(22):e190
Aksnes DW (2003) Characteristics of highly cited papers. Res Eval 12(3):159–170
Bohn MB, Sorensen H, Petersen MK, Soballe K, Lind M (2015) Rotational laxity after anatomical ACL reconstruction measured by 3-D motion analysis: a prospective randomized clinical trial comparing anatomic and nonanatomic ACL reconstruction techniques. Knee Surg Sports Traumatol Arthrosc 23(12):3473–3481
Daniel DM, Stone ML, Dobson BE, Fithian DC, Rossman DJ, Kaufman KR (1994) Fate of the ACL-injured patient a prospective outcome study. Am J Sports Med 22(5):632–644
Desai N, Björnsson H, Musahl V, Bhandari M, Petzold M, Fu FH, Samuelsson K (2014) Anatomic single-versus double-bundle ACL reconstruction: a meta-analysis. Knee Surg Sports Traumatol Arthrosc 22(5):1009–1023
Drogset JO, Grontvedt T, Robak OR, Molster A, Viset AT, Engebretsen L (2006) A sixteen-year follow-up of three operative techniques for the treatment of acute ruptures of the anterior cruciate ligament. J Bone Joint Surg Am 88(5):944–952
Feagin JA Jr, Curl WW (1976) Isolated tear of the anterior cruciate ligament: 5-year follow-up study. Am J Sports Med 4(3):95–100
Girgis FG, Marshall JL, Monajem A (1975) The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res 106:216–231
Granan L-P, Forssblad M, Lind M, Engebretsen L (2009) The Scandinavian ACL registries 2004–2007: baseline epidemiology. Acta Orthop 80(5):563–567
Grimes DA, Schulz KF (2002) An overview of clinical research: the lay of the land. Lancet 359(9300):57–61
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savović J, Schulz KF, Weeks L, Sterne JA (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928
http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM, Gavaghan DJ, McQuay HJ (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17(1):1–12
Johnson DS, Smith RB (2001) Outcome measurement in the ACL deficient knee—what’s the score? Knee 8(1):51–57
Kuroda R, Hoshino Y, Kubo S, Araki D, Oka S, Nagamune K, Kurosaka M (2012) Similarities and differences of diagnostic manual tests for anterior cruciate ligament insufficiency: a global survey and kinematics assessment. Am J Sports Med 40(1):91–99
Lind M, Menhert F, Pedersen AB (2009) The first results from the Danish ACL reconstruction registry: epidemiologic and 2 year follow-up results from 5818 knee ligament reconstructions. Knee Surg Sports Traumatol Arthrosc 17(2):117–124
Lohmander LS, Englund PM, Dahl LL, Roos EM (2007) The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med 35(10):1756–1769
Lyman S, Koulouvaris P, Sherman S, Do H, Mandl LA, Marx RG (2009) Epidemiology of anterior cruciate ligament reconstruction. J Bone Joint Surg Am 91(10):2321–2328
Mascarenhas R, Cvetanovich GL, Sayegh ET, Verma NN, Cole BJ, Bush-Joseph C, Bach BR Jr (2015) Does double-bundle anterior cruciate ligament reconstruction improve postoperative knee stability compared with single-bundle techniques? A systematic review of overlapping meta-analyses. Arthroscopy 31(6):1185–1196
Mascarenhas R, Saltzman BM, Sayegh ET, Verma NN, Cole BJ, Bush-Joseph C, Bach BR (2015) Bioabsorbable versus metallic interference screws in anterior cruciate ligament reconstruction: a systematic review of overlapping meta-analyses. Arthroscopy 31(3):561–568
Saccomanno MF, Shin JJ, Mascarenhas R, Haro M, Verma NN, Cole BJ, Bach BR Jr (2014) Clinical and functional outcomes after anterior cruciate ligament reconstruction using cortical button fixation versus transfemoral suspensory fixation: a systematic review of randomized controlled trials. Arthroscopy 30(11):1491–1498
Schindler OS (2012) Surgery for anterior cruciate ligament deficiency: a historical perspective. Knee Surg Sports Traumatol Arthrosc 20(1):5–47
Speziali A, Delcogliano M, Placella G, Bartoli M, Menghi A, Cerulli G (2014) Fixation techniques for the anterior cruciate ligament reconstruction: early follow-up. A systematic review of level I and II therapeutic studies. Musculoskelet Surg 98(3):179–187
Zeng C, Gao SG, Li H, Yang T, Luo W, Li YS, Lei GH (2014) Autograft versus allograft in anterior cruciate ligament reconstruction: a meta-analysis of randomized controlled trials and systematic review of overlapping systematic reviews. Arthroscopy 32(1):153–163
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
No funding was received for the conduction of this study.
Ethical approval
For this type of study, formal consent is not required.
Informed consent
None
Rights and permissions
About this article

Cite this article
Ahmad, S.S., Meyer, J.C., Krismer, A.M. et al. Outcome measures in clinical ACL studies: an analysis of highly cited level I trials. Knee Surg Sports Traumatol Arthrosc 25, 1517–1527 (2017). https://doi.org/10.1007/s00167-016-4334-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-016-4334-4