
Abstract
Purpose
Sports activity after surgical AC joint stabilisation has not been comprehensively evaluated to date. The aim of this study was to determine rate, level and time to return to sports after AC joint stabilisation and to identify the influence of overhead sports on post-operative sports activity.
Methods
In this retrospective case series, a total of 68 patients with a high-grade AC joint dislocation (Rockwood type V) were stabilised using a single TightRope technique. Fifty-five patients (80.9 %) with median age of 42.0 (range, 18–65) years completed questionnaires regarding sports activity before and after surgery. Clinical outcome and complications were also evaluated. Forty-three patients participated in sports regularly before injury. Their sports activity was rated according to Allain, and non-overhead and overhead sports were differentiated.
Results
At median follow-up of 24 (18–45) months, 41 of 43 patients (95.3 %) had returned to sports. 63 % returned to the same sports activity as before injury. 16.3 % needed to adapt the type of sports to reduce demanding activities. 11.6 % reduced the frequency and 32.5 % the intensity of sports. The median time to return to sports was 9.5 (3–18) months. Overhead athletes (Allain Type III and IV) had to reduce their sports activity significantly more often (11.8 vs. 53.8 %; p = 0.011) and needed more time to return to sports (9.5 vs. 4.5 months; p = 0.009).
Conclusion
After stabilisation of AC joint dislocation, the majority of patients returned to sports after a substantial period of time. Overhead athletes, in particular, required more time and had to considerably reduce their sports activity. The findings impact therapeutic decision-making after AC joint injury and help with the prognosis and assessment of rehabilitation progress.
Level of evidence
IV.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acromioclavicular (AC) dislocation is common in young active patients. The injury occurs especially in contact sports or after a fall while cycling or winter sports [8, 14, 15, 19, 37, 51]. Approximately 9 % of shoulder girdle injuries involve the AC joint [34]. Depending on the type and the intensity of the sports activity being practised, the percentage increases up to 40 % [23]. Classified by Rockwood et al. [42] into six grades, there is consensus about initial conservative treatment of Type I and II injuries, and though lacking evidence, in high-grade dislocations (Type IV–VI) a primarily surgical treatment is considered in most of the cases [2]. The treatment of Type III joint separations is still under discussion [25]. A variety of surgical techniques has been described, but none of them is considered to be a gold standard. In this context, the anatomic AC joint stabilisation with a synthetic non-absorbable suture system in mini-open or arthroscopic technique is a well observed and increasingly used treatment option for Type III to VI lesions [17, 22, 28, 30, 36, 43, 46, 50]. Short- and midterm follow-up presented good to excellent clinical and radiographic results leaving open issues with respect to the optimal operation technique, the placement of the drilling hole or the required number of sutures [26, 27, 47, 52, 53].
Despite the high frequency of AC joint injury and its relation to an active patient cohort, no study has considered the sports activity after AC joint stabilisation in detail. Especially for surgically treated high-grade AC joint separations (Type V), there is a lack of evidence about the sports activity after surgery. To the authors’ best knowledge, this is the first study to comprehensively analyse sports activity after AC joint stabilisation.
The purpose of this study was to determine the rates of return to sports, the time it took the patients to return to sports, level of activity following stabilisation of high-grade (Type V) acromioclavicular joint dislocation and to investigate the relevance of overhead sports on activity following AC injury. It was hypothesised that overhead athletes exhibit more limitations regarding return to sports compared to non-overhead athletes after AC joint stabilisation.
Materials and methods
Between 2011 and 2014, a consecutive series of 68 patients with a Rockwood type V [42] injury, irrespective of pre-injury sports activity, was enrolled retrospectively. Initial radiographs included true anteroposterior/axillary view of the affected shoulder and bilateral anteroposterior stress view (10 kg). In all cases, an acromioclavicular joint stabilisation in a single TightRope technique was performed at a level 1 trauma centre.
The following inclusion criteria were set: AC dislocation Type V according to Rockwood [42]; the injury occurred within the last 4 weeks; no concomitant injury of upper extremity; no shoulder problems concerning the injured or contralateral side before injury; and age ≥18.
A questionnaire regarding sports activity, the Constant–Murley Score (CMS) for self-assessment [6, 10] and the Disability of the Arm, Shoulder and Hand (DASH) questionnaire [21] were sent to all 68 patients. Thirteen patients (19.1 %) did not reach follow-up: Six refused to participate and seven could not be contacted.
In the end, 55 patients, including 47 males (85.5 %) and eight females (14.5 %), completed the questionnaires (follow-up: 80.9 %). They were followed for a median period of 24 months (range, 18–45 months).
Surgical procedure and post-operative care
All patients were operated on a standard procedure using the mini-incision single TightRope technique as described by Beris et al. [5] (Fig. 1). All surgeries were performed by one of two shoulder specialists (SSF, TG).

Anteroposterior view after single TightRope stabilisation
The post-operative rehabilitation protocol consisted of immobilisation of the arm in a shoulder abduction orthosis (Medi SAK®; Medi, Bayreuth, Germany) at 30° for 4 weeks. Pain-free, passive range of motion up to 90° abduction and flexion and 40° internal/external rotation (IR/ER) was started on the first day post-surgery. Active motion restricted at 90° abduction and flexion and 40° IR/ER rotation was allowed after four weeks. Active range of motion on all ranges was allowed after 6 weeks, but overhead motion was especially trained under supervision of a physiotherapist at the start. Strength training for rotator cuff, deltoid and scapula stabilisers was gradually increased beginning at 6 weeks post-operative. Three months after surgery carrying weight and non-contact sports were allowed. After 6 months, the patients were allowed to return to sports without restriction.
Data acquisition
For all included participants, electronic patient records were screened for injury–surgery time interval, surgery time, hospitalisation time and documented revisions.
The participants received a questionnaire regarding general demographic data, pre-injury sports activity, post-injury sports activity and time to return to sports (see “Appendix in ESM”).
The type of sport was graded with regard to its strain on the shoulder according to Allain et al. (GI = “non-impact sports”; GII = “high-impact sports”; GIII = “overhead sports with hitting movements”; GIV = “overhead sports with hitting movements and sudden stops”) [1, 40]. Patients were grouped according to their pre-injury sports activity according to Allain et al. Group 1 included patients practising sports without overhead components (GI and G II according to Allain). Group 2 consisted of patients participating frequently in overhead sports (G III and G IV). A stratification between recreational and competitive or elite athletes was not conducted. None of the patients was a professional athlete. Patients who were not participating in sports before injury (non-athlete) were considered in regard to clinical outcome as well, but were not taken into account at the analysis of post-operative sports activity.
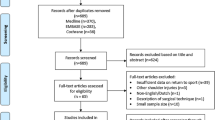
According to this assessment, 17 patients (30.9 %) were referred to group 1 (non-overhead sports) and 26 patients (47.3 %) were referred to group 2 (overhead sports). 12 patients (21.8 %) did no sports before injury (non-athlete) (Fig. 2).

Flow diagram; Group distribution
The functional outcome was evaluated using an adopted Constant–Murley Score (CMS) for self-assessment, which was inaugurated and validated by Böhm et al. (pts) [6, 10], the age and gender adjusted CMS (%) [54] and the DASH questionnaire [21].
This study was approved by the local ethics committee of the board of Medical Profession of Rhineland-Palatinate in Mainz (No. 837.009.15/9777).
Statistical analysis
Statistical analysis was performed, advised by a biometrician, using SPSS. Descriptive results are given as median and minimum/maximum for continuous variables, frequencies and percentage for categorical data. Nominal/categorical data were compared using the Chi-square test or Wilcoxon signed-rank test. For metric data, the Mann–Whitney U test was used. The level of significance was defined as p = 0.05. Evaluation of the data was retrospective; an a priori sample size estimation has not been conducted. A post hoc sample size calculation regarding the hypothesis computed, that a difference of 40 %, as found at this study, can be detected with a sample size of N = 19 per group with a power of 80 % at the level of significance of 0.05.
Results
Basic demographic data, concomitant injuries and surgery-related information for all 55 patients are given in Table 1. There were no significant discrepancies concerning descriptive data (Table 1) between group 1 and 2. A sports-related injury was reported in 28 cases (50.9 %), most frequently due to a bicycle accident (N = 16, 19.1 %).
Clinical outcome
For all 55 patients, the median CMS was 85.0 pts (range, 44.0–100.0 pts) at final follow-up. The CMS of the contralateral side was 99.3 pts in median (range, 70.0–100.0 pts), which was significantly higher than the involved shoulder (p < 0.001). The median DASH Score was 5.0 (range, 0.0–43.9). Comparisons of both groups revealed no significant differences between overhead and non-overhead athletes concerning CMS or DASH (Table 2).
Sports activity before injury
Forty-three patients (78.2 %) performed regular sports activity before injury. The median of sports frequency was three times a week (Fig. 3). According to Allain, 26 patients (60.5 %, group 2) participated in overhead sports and 17 patients (39.5 %, group 1) practised non-overhead sports (Table 4; Fig. 4).

Comparison of pre- and post-injury frequency of sports (N = 43); (p = 0.004)

Comparison of pre- and post-injury sports level according to Allain (N = 43); (p = 0.051)
Sports activity after surgery
At final follow-up, 41 of 43 (95.3 %) of the patients, who were participating in sports before injury, returned to sports. In detail, two patients (4.7 %) had to stop their sports activity due to injury-related shoulder problems. Overall, the sports frequency was significantly lower at follow-up (p = 0.004, Fig. 3). The level of sports according to Allain showed a trend towards lower shoulder demanding activity (n.s., Fig. 4).
Sixteen patients (37.2 %) had to change their sports activity after the operation (Table 3).
Athletes participating in overhead sports (group 2) needed to change sports activity significantly more often (53.8 vs. 11.8 %; p = 0.011). Mainly, overhead athletes had to reduce intensity (N = 13, 50 %) and frequency (N = 5, 19.2 %). Interestingly, seven patients (26.9 %) participating in overhead sports before injury had to reduce their sports level to low demanding sports, while none of the non-overhead athletes (group 1) lowered their level (p = 0.029) (Table 4).
The median time to return completely to their pre-injury sports activity was 9.5 months (range, 3.0–18.0 months). Overhead athletes needed a significantly longer time to completely return to sports (9.5 vs. 4.5 months; p = 0.009).
Discussion
The most important finding of the present study was that despite high general return rates to sports (95.3 %) there are considerable restrictions following a surgical AC joint stabilisation. For overhead athletes, in particular, we noticed a significant alteration of sports activity after surgery. More than half of them reported that they had to change their sports activity. In detail, 26.9 % of the overhead athletes had to choose another less demanding type of sport and 50 % reported that they reduced the intensity of sports. In contrast, only two of the non-overhead athletes (11.8 %) had to change their sports activity in general after surgery.
This supports the notion that overhead activity is more demanding for the AC joint [31, 33]. In fact, all of the overhead athletes, who needed to change the type of sports, practised non-shoulder demanding sports afterwards (Table 4). In addition, a reduction in sports frequency was only found in group 2. Despite the high return to sports rates, more than half of the patients reported soreness of the operated AC joint during sports activity. These complaints were independent from the type and intensity of sports.
Data concerning sports activity after AC joint injury are lacking, despite the fact that AC joint injury has been identified as a typical sports-related injury [12, 15, 38]. According to the literature, 42.9 % of AC joint injuries are sports related [8]. This is in agreement with our findings (50 % sports-associated traumas). Here, bicycle accidents were found to be responsible for most cases. However, it must be noted that we did not distinguished between road traffic and sports activity associated accidents.
There are several epidemiologic studies regarding professional athletes, which analyse incidence and mechanisms of AC joint injury in detail. These studies provide only sporadic information on sports activity after AC joint injury [13, 24, 32, 38]. In these studies, the time to return to sports varied between 9.8 and 22.1 days on average [24, 32, 38], differing considerably from our data. Further analyses of return to sports rates and sports activity after AC joint injuries were not provided. Moreover, the studies dealt with a very restricted cohort (solely professional football players) with various grades of injury (Rockwood I–IV). Most often, the injuries were rated as Rockwood I–III injuries and were treated conservatively.
In conclusion, the existing data about sports activity after a conservative treatment of AC joint injury report a remarkably shorter rehabilitation period and less impairment of sports activity [24, 32, 38]. In this context, the ongoing controversial debate about the benefit of surgical treatment should be considered. There is a general consensus about primary non-operative treatment of Rockwood I and II lesions [4]. Several studies promote a shorter rehabilitation period—an immobilisation of the shoulder is only recommended for short-term pain reduction [4]—and fewer complications in conservative treatment [49]. The aforementioned studies which are dealing with professional football players seem to confirm this argument.
In contrast, data about optimal treatment of Type III injury remain uncertain. An older survey among American team orthopaedics revealed that 69 % would treat the injury non-operatively [35]. Recently, Balke et al. reported a considerable preference among German surgeons for surgical treatment of Type III lesions (73 %). For Type V lesions, 99 % of surgeons prefer a surgical treatment [2].
Especially for active patient cohorts, surgical treatment is recommend [4, 18]. The data from this study call this approach into question. As elaborated above, in this series in particular the more active overhead athletes complained about impairment of sports activity post-operatively.
A comparison with conservative treated patients with Type V injury could clarify this point. Unfortunately, a conservative treated control group is lacking in our study and in the existing literature as well. It can be assumed that at least the time to return to sports would be shorter in favour of conservative treated patients. However, due to the heterogenic cohort and inconsistent evaluation of sports activity in comparable studies a substantiated statement cannot be made at this point.
Data about return to sports capacity after AC joint surgery are heterogeneous. Rangger et al. reported a reduction in sports activity in 28 % of patients after conservative or surgical treatment of AC joint injuries [41]. Gstettner et al. demonstrated that four of 19 patients (21 %) who were treated with a hook plate were not able to return to their former level of sports [18]. Bannister et al. compared conservative versus surgical treated patients and found a significant longer time to return to sports after surgical treatment (16 vs. 7 weeks) [3]. In contrast, Cardone et al. reported that the time to return to pre-injury sports level was in favour of the surgical group (18.8 vs. 26.2 weeks) [7]. These studies are limited by outdated surgical techniques and heterogeneous types of injury severity, and they also lack detailed information regarding post-operative sports activity.
To date, minimal invasive anatomic coracoclavicular reconstructions have been established as the gold standard. After TightRope stabilisation, 100 % return to sports rates are reported, without specification of type of sports or impairments after surgery [11, 16]. Time to return to sports (120 days) reported by De Carli et al. were comparable to our findings [9]. However, the influence of the type of sport was not considered. Loriaut et al. reported about an average time of 17 weeks before sports were resumed after TightRope stabilisation of distal clavicle fractures. Fourteen of 17 patients reached the same level as before trauma. A differentiation of sports activity was lacking [29].
To the best of our knowledge, our study is the first to provide detailed information on sports activity and impairments after AC stabilisation and to consider the factors that might affect the return to sports rates.
Overall, the clinical results of our study are in agreement with others reporting good to excellent functional results after TightRope stabilisation [9, 22, 45, 46]. A median CMS of 92.9 % and a DASH Score of 5.0 reports indicate satisfactory results.
Interestingly, the present study demonstrates higher revision rates (18 %) compared to published data. Scheibel et al. [46] reported no revisions in 28 cases, the highest incidence of revision rates (12.5 %) was found by Murena et al. [36]. In the present study, five patients (9.1 %) developed wound-healing impairments. This might be related to the mini-open technique. According to the literature, wound-healing problems seem to be less frequent after arthroscopic stabilisation [22, 39, 46]. Conversely, Rosslenbroich et al. reported only one infection out of 83 patients operated on with mini-open technique [43]. All documented wound-healing impairments affected the clavicular incision. We identified a prominent knot of the TightRope, superior to the clavicular button as a potential cause of mechanical irritation or even wicking. Modifying our technique, by submerging the knot beneath the deltoid muscle using an additional vicryl suture, the wound-healing impairments seemed to decrease although there is no statistical evidence to support this. Any further investigation should clarify this point. The rate of revisions due to recurrent instability (7.3 %) was comparable to existing data about single or double TightRope stabilisation [36, 43, 45, 46]. The TightRope technique used in this study only addressed the horizontal instability. Recently, Saier et al. [44] promoted an additional acromioclavicular cerclage for horizontal stability. This might have provided a lower rate of re-instability or even better clinical outcome. Patients were included to this study if the surgical procedure was done within 4 weeks after injury. Several authors recommend an early operation when using artificial augmentation of CC ligaments. They hypothesised that the soft tissue which forms around the device is required for long-term stability [20]. Derived from that, the authors suggested a surgery within the first 3 weeks. To the best of our knowledge, there is no study providing evidence-based data concerning the optimal time to operate. In clinical routine, we are performing a AC stabilisation in TightRope technique within the first 4 weeks after injury and have not found major impairments in patients operated on in the third or fourth week. In this series, a subanalysis revealed no significant differences in clinical outcome between early (within 2 weeks) and late (after 2 weeks) surgical stabilisation. Despite these current findings, we tend to stabilise the AC joint as soon as possible after injury. The outcome of long-term follow-up is important in this regard.
This study was limited by its retrospective design and the relatively short median follow-up of 24 months. The main purpose of this study was to analyse the return to sports. Most of the patients return to sports within the first 18 months. Information about the time to return to sports or sports activity before injury could have been lost due to oblivion in the case of a longer follow-up period. Even so, the retrospective survey of pre-injury sports activity, in particular, might have caused a recall bias. In addition to our main objective, we evaluated the global functional outcome using the Constant–Murley Score. In consideration of the clarity of the study, we decided to omit an additional AC joint-specific evaluation tool as introduced by Scheibel et al. [46] or Taft et al. [48]. Scheibel et al. developed the ACJI because they observed an overestimation of the functional outcome after AC joint injuries by other shoulder scoring systems. This point might explain the high values of CMS, despite the remarkable limitation of sports activity. Applying such an AC joint-specific score could have provided a more differentiated analysis of AC joint function.
It should be noted that there were no professional athletes in this cohort. Here, higher demands on the stabilised joint on the one hand, but more comprehensive medical support on the other hand might lead to different results. The fact that patients with a surgical treatment within 4 weeks after injury were included might have lead to adverse results. All patients were operated on by one of two specialised surgeons, which provides a high standardisation of the surgical procedure, but might imply a performance bias. Beside the surgical technique, the rehabilitation protocol was standardised.
Another strength of this study is, besides its large number of patients, the homogeneous cohort. Only patients with a Rockwood Type V injury were enrolled.
Enhancing new knowledge about limitations of return to sports after AC stabilisation, especially for overhead athletes, can give the findings impact with respect to therapeutic decision-making after injury and help in prognosis and assessment of the rehabilitation progress. Patients can be informed about realistic chances and risks regarding sports activity after a surgical AC stabilisation.
Conclusion
After minimal invasive stabilisation of the AC joint using a single TightRope technique, the majority of patients return to sports within the first year. Besides this quite long rehabilitation period, a notable risk of surgical associated complication should be considered. In particular, athletes participating in overhead activity should be informed about the frequent necessity to reduce the intensity of the sporting activity or to even change the type of sport practised. On the basis of our data, the current assumption that sports activity is a relative indication to prefer surgical treatment should be further reviewed, particularly in high-grade AC instability. Further studies, including a conservative control group and other surgical techniques, need to be implemented.
References
Allain J, Goutallier D, Glorion C (1998) Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 80:841–852
Balke M, Schneider MM, Shafizadeh S, Bathis H, Bouillon B, Banerjee M (2015) Current state of treatment of acute acromioclavicular joint injuries in Germany: is there a difference between specialists and non-specialists? A survey of German trauma and orthopaedic departments. Knee Surg Sports Traumatol Arthrosc 23:1447–1452
Bannister GC, Wallace WA, Stableforth PG, Hutson MA (1989) The management of acute acromioclavicular dislocation. A randomised prospective controlled trial. J Bone Joint Surg Br 71:848–850
Beitzel K, Cote MP, Apostolakos J, Solovyova O, Judson CH, Ziegler CG, Edgar CM, Imhoff AB, Arciero RA, Mazzocca AD (2013) Current concepts in the treatment of acromioclavicular joint dislocations. Arthroscopy 29:387–397
Beris A, Lykissas M, Kostas-Agnantis I, Vekris M, Mitsionis G, Korompilias A (2013) Management of acute acromioclavicular joint dislocation with a double-button fixation system. Injury 44:288–292
Boehm D, Wollmerstedt N, Doesch M, Handwerker M, Mehling E, Gohlke F (2004) Development of a questionnaire based on the Constant–Murley-score for self-evaluation of shoulder function by patients. Unfallchirurg 107:397–402
Cardone D, Brown JN, Roberts SN, Saies AD, Hayes MG (2002) Grade III acromioclavicular joint injury in Australian Rules Football. J Sci Med Sport 5:143–148
Chillemi C, Franceschini V, Dei Giudici L, Alibardi A, Salate Santone F, Ramos Alday LJ, Osimani M (2013) Epidemiology of isolated acromioclavicular joint dislocation. Emerg Med Int 2013:171609
Cohen G, Boyer P, Pujol N, Hamida Ferjani B, Massin P, Hardy P (2011) Endoscopically assisted reconstruction of acute acromioclavicular joint dislocation using a synthetic ligament. Outcomes at 12 months. Orthop Traumatol Surg Res 97:145–151
Constant CR, Murley AH (1987) A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res 214:160–164
De Carli A, Lanzetti RM, Ciompi A, Lupariello D, Rota P, Ferretti A (2015) Acromioclavicular third degree dislocation: surgical treatment in acute cases. J Orthop Surg Res 10:13
Dick R, Ferrara MS, Agel J, Courson R, Marshall SW, Hanley MJ, Reifsteck F (2007) Descriptive epidemiology of collegiate men’s football injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train 42:221–233
Dragoo JL, Braun HJ, Bartlinski SE, Harris AH (2012) Acromioclavicular joint injuries in National Collegiate Athletic Association football: data from the 2004–2005 through 2008–2009 National Collegiate Athletic Association Injury Surveillance System. Am J Sports Med 40:2066–2071
Ekstrand J, Hagglund M, Tornqvist H, Kristenson K, Bengtsson H, Magnusson H, Walden M (2013) Upper extremity injuries in male elite football players. Knee Surg Sports Traumatol Arthrosc 21:1626–1632
Flik K, Lyman S, Marx RG (2005) American collegiate men’s ice hockey: an analysis of injuries. Am J Sports Med 33:183–187
Glanzmann MC, Buchmann S, Audige L, Kolling C, Flury M (2013) Clinical and radiographical results after double flip button stabilization of acute grade III and IV acromioclavicular joint separations. Arch Orthop Trauma Surg 133:1699–1707
Grantham C, Heckmann N, Wang L, Tibone JE, Struhl S, Lee TQ (2014) A biomechanical assessment of a novel double endobutton technique versus a coracoid cerclage sling for acromioclavicular and coracoclavicular injuries. Knee Surg Sports Traumatol Arthrosc 24:1918–1924
Gstettner C, Tauber M, Hitzl W, Resch H (2008) Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg 17:220–225
Headey J, Brooks JH, Kemp SP (2007) The epidemiology of shoulder injuries in English professional rugby union. Am J Sports Med 35:1537–1543
Hou Z, Graham J, Zhang Y, Strohecker K, Feldmann D, Bowen TR, Chen W, Smith W (2014) Comparison of single and two-tunnel techniques during open treatment of acromioclavicular joint disruption. BMC Surg 14:53
Hudak PL, Amadio PC, Bombardier C (1996) Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand). Am J Ind Med 29:602–608
Jensen G, Katthagen JC, Alvarado LE, Lill H, Voigt C (2014) Has the arthroscopically assisted reduction of acute AC joint separations with the double tight-rope technique advantages over the clavicular hook plate fixation? Knee Surg Sports Traumatol Arthrosc 22:422–430
Kaplan LD, Flanigan DC, Norwig J, Jost P, Bradley J (2005) Prevalence and variance of shoulder injuries in elite collegiate football players. Am J Sports Med 33:1142–1146
Kelly BT, Barnes RP, Powell JW, Warren RF (2004) Shoulder injuries to quarterbacks in the national football league. Am J Sports Med 32:328–331
Korsten K, Gunning AC, Leenen LPH (2014) Operative or conservative treatment in patients with Rockwood type III acromioclavicular dislocation: a systematic review and update of current literature. Int Orthop 38:831–838
Kraus N, Haas NP, Scheibel M, Gerhardt C (2013) Arthroscopically assisted stabilization of acute high-grade acromioclavicular joint separations in a coracoclavicular Double-TightRope technique: V-shaped versus parallel drill hole orientation. Arch Orthop Trauma Surg 133:1431–1440
Kraus N, Scheibel M (2011) Arthroskopisch-assistierte Stabilisierung der akuten Schultereckgelenkinstabilität. Obere Extremität 6:90–98
Liu X, Huangfu X, Zhao J (2015) Arthroscopic treatment of acute acromioclavicular joint dislocation by coracoclavicular ligament augmentation. Knee Surg Sports Traumatol Arthrosc 23:1460–1466
Loriaut P, Moreau PE, Dallaudiere B, Pelissier A, Vu HD, Massin P, Boyer P (2015) Outcome of arthroscopic treatment for displaced lateral clavicle fractures using a double button device. Knee Surg Sports Traumatol Arthrosc 23:1429–1433
Lu N, Zhu L, Ye T, Chen A, Jiang X, Zhang Z, Zhu Q, Guo Q, Yang D (2014) Evaluation of the coracoclavicular reconstruction using LARS artificial ligament in acute acromioclavicular joint dislocation. Knee Surg Sports Traumatol Arthrosc 22:2223–2227
Ludewig PM, Phadke V, Braman JP, Hassett DR, Cieminski CJ, LaPrade RF (2009) Motion of the shoulder complex during multiplanar humeral elevation. Journal Bone Joint Surg Am 91:378–389
Lynch TS, Saltzman MD, Ghodasra JH, Bilimoria KY, Bowen MK, Nuber GW (2013) Acromioclavicular joint injuries in the National Football League: epidemiology and management. Am J Sports Med 41:2904–2908
Mall NA, Foley E, Chalmers PN, Cole BJ, Romeo AA, Bach BR Jr (2013) Degenerative joint disease of the acromioclavicular joint: a review. Am J Sports Med 41:2684–2692
Mazzocca AD, Arciero RA, Bicos J (2007) Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med 35:316–329
McFarland EG, Blivin SJ, Doehring CB, Curl LA, Silberstein C (1997) Treatment of grade III acromioclavicular separations in professional throwing athletes: results of a survey. Am J Orthop (Belle Mead NJ) 26:771–774
Murena L, Vulcano E, Ratti C, Cecconello L, Rolla PR, Surace MF (2009) Arthroscopic treatment of acute acromioclavicular joint dislocation with double flip button. Knee Surg Sports Traumatol Arthrosc 17:1511–1515
Nordqvist A, Petersson CJ (1995) Incidence and causes of shoulder girdle injuries in an urban population. J Shoulder Elbow Surg 4:107–112
Pallis M, Cameron KL, Svoboda SJ, Owens BD (2012) Epidemiology of acromioclavicular joint injury in young athletes. Am J Sports Med 40:2072–2077
Pauly S, Kraus N, Greiner S, Scheibel M (2013) Prevalence and pattern of glenohumeral injuries among acute high-grade acromioclavicular joint instabilities. J Shoulder Elbow Surg 22:760–766
Ranalletta M, Rossi LA, Piuzzi NS, Bertona A, Bongiovanni SL, Maignon G (2015) Return to sports after plate fixation of displaced midshaft clavicular fractures in athletes. Am J Sports Med 43:565–569
Rangger C, Hrubesch R, Paul C, Reichkendler M (2002) Capacity to participate in sports after injuries of the acromioclavicular joint. Orthopaede 31:587–590
Rockwood CA (1984) Injuries in the acromioclavicular joint: subluxations and dislocations about the shoulder. In: Rockwood CA, Green DP (eds) Fractures in Adults, 2nd edn, vol 1. JB Lippincott, Philadelphia, pp 860–910
Rosslenbroich SB, Schliemann B, Schneider KN, Metzlaff SL, Koesters CA, Weimann A, Petersen W, Raschke MJ (2015) Minimally invasive coracoclavicular ligament reconstruction with a flip-button technique (MINAR): clinical and radiological midterm results. Am J Sports Med 43:1751–1757
Saier T, Venjakob AJ, Minzlaff P, Fohr P, Lindell F, Imhoff AB, Vogt S, Braun S (2015) Value of additional acromioclavicular cerclage for horizontal stability in complete acromioclavicular separation: a biomechanical study. Knee Surg Sports Traumatol Arthrosc 23:1498–1505
Salzmann GM, Walz L, Buchmann S, Glabgly P, Venjakob A, Imhoff AB (2010) Arthroscopically assisted 2-bundle anatomical reduction of acute acromioclavicular joint separations. Am J Sports Med 38:1179–1187
Scheibel M, Droschel S, Gerhardt C, Kraus N (2011) Arthroscopically assisted stabilization of acute high-grade acromioclavicular joint separations. Am J Sports Med 39:1507–1516
Schwarting T, Lechler P, Bockmann B, Debus F, Ziring E, Frink M (2015) The benefit of arthroscopically assisted therapy for concomitant glenohumeral injuries in patients with unstable lateral clavicle fractures. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-015-3909-9
Taft TN, Wilson FC, Oglesby JW (1987) Dislocation of the acromioclavicular joint. An end-result study. J Bone Joint Surg Am 69:1045–1051
Tamaoki MJ, Belloti JC, Lenza M, Matsumoto MH, Gomes Dos Santos JB, Faloppa F (2010) Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults. Cochrane Database Syst Rev:Cd007429
Venjakob AJ, Salzmann GM, Gabel F, Buchmann S, Walz L, Spang JT, Vogt S, Imhoff AB (2013) Arthroscopically assisted 2-bundle anatomic reduction of acute acromioclavicular joint separations: 58-month findings. Am J Sports Med 41:615–621
Weaver JK (1987) Skiing-related injuries to the shoulder. Clin Orthop Relat Res 216:24–28
Weiser L, Nuchtern JV, Sellenschloh K, Puschel K, Morlock MM, Rueger JM, Hoffmann M, Lehmann W, Grossterlinden LG (2015) Acromioclavicular joint dislocations: coracoclavicular reconstruction with and without additional direct acromioclavicular repair. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-015-3920-1
Yi Y, Kim JW (2015) Coronal plane radiographic evaluation of the single TightRope technique in the treatment of acute acromioclavicular joint injury. J Shoulder Elbow Surg 24:1582–1587
Yian EH, Ramappa AJ, Arneberg O, Gerber C (2005) The Constant score in normal shoulders. J Shoulder Elbow Surg 14:128–133
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
All costs arising for this clinical study was funded by the internal clinic-budget for scientific follow up.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Porschke, F., Schnetzke, M., Aytac, S. et al. Sports activity after anatomic acromioclavicular joint stabilisation with flip-button technique. Knee Surg Sports Traumatol Arthrosc 25, 1995–2003 (2017). https://doi.org/10.1007/s00167-016-4287-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-016-4287-7