
Abstract
Purpose
To investigate how the Achilles tendon Total Rupture Score (ATRS) at 3 months and 1 year after injury is associated with a patient’s ability to return to work and sports as well as to investigate whether sex and age influence ATRS after 3 months and 1 year.
Method
This is a retrospective study analysing the data from the Danish Achilles tendon Database. A total of 366 patients were included. Logistic regression was conducted to describe the effect of ATRS on return to work and sports. The effect of age and sex on ATRS was analysed by linear regression.
Results
Three months after injury patients had a significantly increased chance of return to sport after 1 year with an increased ATRS (OR 1.06, p = 0.001) but a non-significant effect on return to work. After 1 year, patients had a significantly increased probability of having returned to sport (OR 1.11, p < 0.001) and also having returned to work (OR 1.05, p = 0.007) with an increased ATRS. Men had an average 7 (p = 0.006) points higher ATRS at 3 months and an average 22 (p = 0.006) points higher at 1 year.
Conclusion
ATRS is associated with patients’ ability to return to sports and work. ATRS at 3 months can be used as a predictor of the patient’s ability to return to sports after 1 year. Hereby, ATRS might help to individualise rehabilitation by identifying patients who do not respond adequately to the chosen treatment.
Level of evidence
II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Achilles tendon rupture (ATR) is a relatively common injury (11–37 per 100,000 per year) [8, 12, 18]. In a recent nationwide Danish register study, a small but statistically significant increase in incidences from 27 per 100,000 persons/year in 1994 to 31 per 100,000 persons/year in 2013 was found. The increasing incidence was explained by a large increase in the age group of those older than 50 years of age. The male–to-female ratio was 3:1 [5]. The ATR is an injury that affects patients in many ways with major functional deficits and prevailing symptoms 1 and 2 years after the injury [20, 23, 30]. As such, it is desirable to identify the predictive factors for an adequate outcome in order to make individualised treatment possible.
The capability of a person to return to work and sports activities after an ATR has been investigated when comparing different treatments. A meta-analysis by Soroceanu et al. [27] comparing surgical and conservative treatments found that patients who underwent surgery returned to work 19 days sooner than patients who underwent non-surgical treatment [95 % confidence interval (CI) 3.9–34.0; p = 0.0014]. In contrast, Wilkins and Bisson [29] concluded in their systematic review that no significant difference was noted in the time of return to work when the data were meta-analysed. In a meta-analysis comparing functional rehabilitation and immobilisation, a non-significant difference favouring controlled early motion was found [14].
When it comes to returning to previous sports, Mortensen et al. [19] found that patients receiving controlled early motion returned to their sport at a median of 4 months and patients being immobilised returned at a median of 7.5 months. No significant difference has been found in the capability of returning to sport when comparing operative and non-operative treatment and weight bearing or non-weight-bearing treatment [1, 10].
The Achilles tendon Total Rupture Score (ATRS) after 3 months was shown to be correlated with function after 1 year [24]. If ATRS correlates with other outcomes, the ability to use it as predictive factors is unclear. By identifying predictive factors, these can contribute to optimising and individualising the rehabilitation by identifying patients not responding as expected to the chosen treatment.
The purpose of this study is to describe the correlation between the ATRS 1 year after injury with a patient’s ability to return to sports and work and, furthermore, to investigate whether the ATRS, 3 months after injury, could predict a return to sports and work 1 year after the injury. Finally, the purpose is to describe the influence of sex and age on ATRS.
Materials and methods
This study was performed as a retrospective registry study that analyses prospectively gathered data.
Organisation of DADB
The Danish Achilles tendon Database (DADB) was initiated in April 2012. The DADB is a clinical research database with 781 registered patients (May 2015) from five different hospitals in Denmark. The objective of the DADB is to describe and monitor the quality of treatment of ATR and to conduct epidemiological research. The re-rupture rate and ATRS are used as quality indicators.
The data were collected in paper form until August 2015. Anamnestic data and questionnaires are registered by the patient, whereas test data are registered by the clinician. Completed forms are sent to the database administration that is responsible for entering data in a Microsoft Access database. Since August 2015, DADB is converted to a web-based database.
The DADB is located at the Clinical Orthopaedic Research Hvidovre (CORH) at Copenhagen University Hospital, Hvidovre. The DADB has one part-time research assistant. All data management is performed by an in-house statistician named Thomas Kallemose.
Database content
The data were collected at the following points in time: recently after injury, after 3–4 months (listed as 3 months further on), after 1 year, and after 2 years. Complications were registered when they appeared. In addition, the first two data registrations were performed in the outpatient clinic. Registrations after the first and second year were conducted via mail correspondence.
A summary of the database content is shown in Fig. 1. The work-related questions (possible answers, “yes”/“no”) were as follows: Were you working before your present injury? Have you resumed the same type of work on a full-time basis? Have you changed your job or changed to working part-time due to the injury? The sports-related questions (possible answers, “yes”/“no”) were as follows: Did you participate in sports before your present injury? Have you resumed the same type of sport after the injury? Have you changed to a less stressful sport due to the injury?

Regarding all the data registrations, patients were also asked to fill out the ATRS. The ATRS is a patient-reported outcome measure (PROM) developed for use after an ATR. It consists of 10 questions concerning symptoms and physical activity, for which patients are asked to respond using an 11-point Likert scale (0–10). A patient scoring 0 implies major limitations/symptoms and 10 no limitations or symptoms. Answers from all 10 questions are added to a total score, with 100 being the maximum score [21].
The Danish version was found to have good validity and to be reliable for comparison on a group level with an intraclass correlation coefficient of the test–retest on 0.908. The minimal detectable change in the Danish version was 18.5, which may call into question the ability of the ATRS to assess individual patients over time. The standard error of measurement was 6.7. This indicates that the ATRS is a reliable PROM for measuring differences down to 7 points between groups of patients [4].
The DADB has approval from the Danish Data Protection Agency, and the study was reported to the IRB of Capital Region’s Research Ethics Committee. No IRB approval was needed (journal number: 15011368).
Statistical analysis
Logistic regression models were used to assess the association between the ATRS score and returning to work and sports after 1 year. The ATRS score was included in the models of the ATRS at a 3-month follow-up and a 1-year follow-up in separate models. Age and sex were also included in the models. The results were presented as odds ratios (ORs) with confidence intervals (CIs). The fits of the logistic models were evaluated by the Hosmer–Lemeshow goodness-of-fit (GOF) test [7]. The Hosmer–Lemeshow GOF test was conducted using the “Hoslem test” function in the “Resource Selection” package. Associations between the ATRS at 3 and 12 months regarding age and sex, with interaction between age and sex, were analysed by linear regression models, and the residuals of the model were evaluated by a Q–Q plot. All analysis was conducted using R 3.2.0. The sample size calculation was not done since the size of the population was given in advance.
Results
In the period from April 2012 to May 2015, 366 patients attended follow-up and had completed ATRS registrations after 3 months and 80 patients after 1 year (Fig. 2). The median age for the group was 47 years (range 20–86) with 81 % being males. Descriptive statistics of the two subgroups is given in Table 1.

Flow chart of patients from DADB included in this study
Association between the ATRS and return to sports and work 1 year after injury
The present results showed an association between the ATRS at 3-month follow-up and return to sport after 1 year (Fig. 3). One-point increment in the ATRS score led to a 6 % increased odds of the person returning to sports (OR 1.06, CI 1.02–1.09, p = 0.002). No evidence of an association between the ATRS score after 3 months and return to work after 1 year was found.

Predictive probability plot. Change in probability for return to sports and work at 1 year with changing ATRS at 3 month. The plot is based on male age 47
Results also demonstrated an association between the ATRS score at the 1-year follow-up and being active in sports (OR 1.11, CI 1.05–1.17, p < 0.001) and active in work (OR 1.05, CI 1.01–1.09, p = 0.007) (Fig. 4). At the same time, an increased ATRS score 1 year after injury indicates an increased probability for patients to be active in work and sports.

Probability plot. Change in probability for being sport- and work active with changing ATRS at 1 year. The plot is based on male age 47
All estimates of the association between the ATRS and return to sports or work are given in Table 2, and a graphical representation is shown in Figs. 3 and 4.
Effect of sex and age on the ATRS score 3 months and 1 year after injury
For both 3 months and 1 year no significant interaction between age and sex was found with p values of 0.107 and 0.847, respectively, so the following result is from models without the interaction.
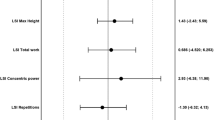
An association was found between the ATRS score and sex both 3 months and 1 year after injury. Men scored 7 points higher at 3 months and 22 points higher at 1 year. However, age showed no significant effect on the ATRS neither 3 months nor 1 year after injury. All estimates of the linear regression are given in Table 3.
Discussion
The main findings of the present study were that the ATRS is associated with patients’ ability to return to sports and work. ATRS at 3 months can be used as a predictor of the patients’ ability to return to sports after 1 year. Furthermore, an association was found between the ATRS and sex both 3 months and 1 year after injury, with male patients having a significantly better score than female patients.
The ATRS score as a predictive value
The most important finding of the study was a strong association between the ATRS at 3 months and a return to sports after 1 year. This indicates that 3 months after an injury, the ATRS can predict a patient’s ability to return to sports 1 year after an injury. An increased score affords the individual added opportunities to return to sporting activities 1 year after an injury. The use of the ATRS as a predictive value for a good outcome is supported by Olsson et al. [24]. They found that an increase of 10 points in the ATRS at 3 months predicted a 2 % higher heel-rise height at both 6 and 12 months. These studies may indicate that the ATRS has a predictive value concerning a patient’s functional outcome 1 year after an injury.
Other predictive factors identified by Olsson et al. [24] include the choice of surgical or non-surgical treatment. This factor was found to be a moderate predictor of symptoms and a weak predictor of function after an ATR. Moreover, increasing age was seen as a strong predictor of reduced heel-rise height.
Association between the ATRS score and return to sports and work
The strong association between the ATRS and patients being work- and sport active at the 1-year follow-up implicates that the ATRS as a PROM is measuring what it is attended to; it supports the construct validity of the ATRS. The purpose of the ATRS score is to “reflect the patients” opinions of the restrictions caused by their symptoms during various physical activities [21].
The present results suggest that the ATRS also reflects patients’ working ability. The expenses of not being able to return to work are high, for the both patient and society. Indeed, sick leave in Denmark has been estimated to cost society at least 37 billion Danish crowns. The longer the duration of the sick-leave period is, the larger the risk will be that the employee will never return to work [17].
Return to sport is an often used outcome in AT research, and it is usually measured in time to return [1, 10, 15]. The importance of returning to previous sports has not been investigated. Patients might abstain from sports due to the rupture or due to a change in life circumstances, the average patient being around 40 years of age [11, 12]. It might also be due to kinesiophobia, fear of re-rupture or the low self-efficacy of ankle function. Kinesiophobia has been seen to correlate with ATRS 12 weeks after injury [22].
Difference in the ATRS score between women and men
A strong association was found between the ATRS and sex both 3 months and 1 year after injury with men having a significantly better ATRS score than women. This raises the question: Can the ATRS be used equally for men and women, or should the score be modified for the two sexes? Are men healing better and achieving a better outcome, or is the ATRS skewed in favour of men?
Olsson et al. [22] found men to have a significantly better functional outcome in the short-term results, indicating an actual difference in performance between the sexes. In a recent cohort study, the difference in outcome between the sexes was evaluated by combining the data from two large randomised controlled trials. Their result presented male patients having a greater improvement in heel-rise height 1 year after injury. When they analysed the data in subgroups (divided in patients treated surgical/non-surgical), the female patients being treated surgically showed a statistically significant lower score on the ATRS compared to men, both 6 months and 1 year after injury [6]. Saxena et al. [25] found that it took a significantly longer time for women to initiate a return to their previous activity levels after an Achilles tendon surgery than for men. This difference might be due to the previously shown differences in tendon healing between the sexes [16, 28]. Magnusson et al. [13] found that women have a lower rate of new connective tissue formation in tendon tissue, respond less to mechanical loading and have less mechanical strength. However, data diverge as Bostick et al. [2] found women to have a better return of calf endurance after 1 year when compared to men. The present study along with previous studies suffers from the same weakness when comparing the sexes: a limited sample size of females leads to wide confidence intervals as females only account for 15–19 % of patients [2, 6, 22].
The significantly better ATRS among men might be due to a different perception of the score and as such may not reflect an actual difference in function, or it might reflect the female subgroup being in need of special treatment and special rehabilitation in order to regain the best possible function. This potential weakness of the ATRS when being used as an outcome should be investigated further in future studies.
The large number of dropouts from the first registration in the database to the 3-month registration and further to 1 year is a clear limitation of this study, thereby affecting the result. The loss of many patients to the 1-year follow-up can partly be explained by the deficiency of routines at the different hospitals and by a lack of compliance from the patients. It is also limited by the short lifespan of the DADB, which leads to a limited sample size at the 1-year follow-up. A similar loss to follow-up is seen in a recent paper by Hutchison et al. [9], where they had approx 16 % of the patients left to follow-up 9 months after injury (with the exception of patients who returned to the required level of activity and thereby were discharged and, therefore, also missing). The phrasing considering return to work and sports is not optimal in the present study. It would be interesting to know the type of work patients returned to and the intensity and type of sports people participated in.
The possible use of the ATRS as a predictive factor might help to individualise rehabilitation by identifying patients who do not respond as expected to a chosen treatment in the clinic. This group of patients may need extra contributions in their rehabilitation to be able to reach their goals in hopes of returning to sports activities.
Conclusion
The ATRS score was associated with a patient’s ability to return to sports and work. The ATRS at 3 months could predict a patient’s ability to return to sports 1 year after an injury. As a result, the ATRS might help to individualise rehabilitation after an ATR by identifying patients who do not respond adequately to a chosen treatment. Men obtained a noticeably higher ATRS 3 months and 1 year after their injuries.
References
Barfod KW, Bencke J, Lauridsen HB, Ban I, Ebskov L, Troelsen A (2014) Nonoperative dynamic treatment of acute Achilles tendon rupture: the influence of early weight-bearing on clinical outcome: a blinded, randomized controlled trial. J Bone Joint Surg Am 96:1497–1503
Bostick GP, Jomha NM, Suchak A, Beaupré L (2010) Factors associated with calf muscle endurance recovery 1 year after Achilles tendon rupture repair. J Orthop Sports Phys Ther 40:345–351
Carmont MR, Silbernagel KG, Mathy A, Mulji Y, Karlsson J, Maffulli N (2013) Reliability of Achilles tendon resting angle and calf circumference measurement techniques. Foot Ankle Surg 19:245–249
Ganestam A, Barfod K, Klit J, Troelsen A (2013) Validity and reliability of the Achilles tendon Total Rupture Score. J Foot Ankle Surg 52:736–739
Ganestam A, Kallemose T, Troelsen A, Barfod KW (2015) Increasing incidence of acute Achilles tendon rupture and a noticeable decline in surgical treatment from 1994 to 2013. A nationwide registry study of 33,160 patients. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-015-3544-5
Gravare Silbernagel K, Brorsson A, Olsson N, Eriksson BI, Karlsson J, Nilsson-Helander K (2015) Sex differences in outcome after an acute Achilles tendon rupture. Orthop J Sports Med. doi:10.1177/2325967115586768
Hosmer DW, Lemeshow S (2000) Applied logistic regression. Wiley, New York
Houshian S, Tscherning T, Riegels-Nielsen P (1998) The epidemiology of Achilles tendon rupture in a Danish county. Injury 29:651–654
Hutchison M, Topliss C, Beard D, Evans RM, Williams P (2015) The treatment of a rupture of the Achilles tendon using a dedicated management programme. Bone Joint J 97:510–515
Jiang N, Wang B, Chen A, Dong F, Yu B (2012) Operative versus nonoperative treatment for acute Achilles tendon rupture: a meta-analysis based on current evidence. Int Orthop 36:765–773
Lantto I, Heikkinen J, Flinkkilä T, Ohtonen P, Leppilahti J (2014) Epidemiology of Achilles tendon ruptures: increasing incidence over a 33-year period. Scand J Med Sci Sports 25:133–138
Levi N (1997) The incidence Copenhagen of Achilles tendon rupture in Copenhagen. Injury 28:311–313
Magnusson SP, Hansen M, Langberg H, Miller B, Haraldsson B, Westh EK, Koskinen S, Aagaard P, Kjaer M (2007) The adaptability of tendon to loading differs in men and women. Int J Exp Pathol 88:237–240
Mark-Christensen T, Troelsen A, Kallemose T, Barfod KW (2014) Functional rehabilitation of patients with acute Achilles tendon rupture: a meta-analysis of current evidence. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-3180-5
Metz R, Verleisdonk E-JMM, van der Heijden GJ-M-G, Clevers G-J, Hammacher ER, Verhofstad MHJ, van der Werken C (2008) Acute Achilles tendon rupture: minimally invasive surgery versus nonoperative treatment with immediate full weightbearing—a randomized controlled trial. Am J Sports Med 36:1688–1694
Miller BF, Hansen M, Olesen JL, Schwarz P, Babraj J, Smith K, Rennie MJ, Kjaer M (2007) Tendon collagen synthesis at rest and after exercise in women. J Appl Physiol 102:541–546
Ministry of Employment (2008) Analysis of sick-leave. http://bm.dk/~/media/BEM/Files/Dokumenter/Publikationer/2008/Sygefravaer.ashx
Moller A, Astron M, Westlin N (1996) Increasing incidence of Achilles tendon rupture. Acta Orthop Scand 67:479–481
Mortensen HM, Skov O, Jensen PE (1999) Early motion of the ankle after operative treatment of a rupture of the Achilles tendon. A prospective, randomized clinical and radiographic study. J Bone Joint Surg Am 81:983–990
Nilsson-Helander K, Silbernagel KG, Thomeé R, Faxén E, Olsson N, Eriksson BI, Karlsson J (2010) Acute Achilles tendon rupture: a randomized, controlled study comparing surgical and nonsurgical treatments using validated outcome measures. Am J Sports Med 38:2186–2193
Nilsson-Helander K, Thomeé R, Silbernagel KG, Thomeé P, Faxén E, Eriksson BI, Karlsson J (2007) The Achilles tendon Total Rupture Score (ATRS): development and validation. Am J Sports Med 35:421–426
Olsson N, Karlsson J, Eriksson BI, Brorsson A, Lundberg M, Silbernagel KG (2014) Ability to perform a single heel-rise is significantly related to patient-reported outcome after Achilles tendon rupture. Scand J Med Sci Sports 24:152–158
Olsson N, Nilsson-Helander K, Karlsson J, Eriksson BI, Thomée R, Faxén E, Silbernagel KG (2011) Major functional deficits persist 2 years after acute Achilles tendon rupture. Knee Surg Sports Traumatol Arthrosc 19:1385–1393
Olsson N, Petzold M, Brorsson A, Karlsson J, Eriksson BI, Grävare Silbernagel K (2014) Predictors of clinical outcome after acute Achilles tendon ruptures. Am J Sports Med 42:1448–1455
Saxena A, Ewen B, Maffulli N (2011) Rehabilitation of the operated achilles tendon: parameters for predicting return to activity. J Foot Ankle Surg 50:37–40
Silbernagel KG, Steele R, Manal K (2012) Deficits in heel-rise height and Achilles tendon elongation occur in patients recovering from an Achilles tendon rupture. Am J Sports Med 40:1564–1571
Soroceanu A, Sidhwa F, Aarabi S, Kaufman A, Glazebrook M (2012) Surgical versus nonsurgical treatment of acute Achilles tendon rupture: a meta-analysis of randomized trials. J Bone Joint Surg Am 94:2136–2143
Westh E, Kongsgaard M, Bojsen-Moller J, Aagaard P, Hansen M, Kjaer M, Magnusson SP (2008) Effect of habitual exercise on the structural and mechanical properties of human tendon, in vivo, in men and women. Scand J Med Sci Sports 18:23–30
Wilkins R, Bisson LJ (2012) Operative versus nonoperative management of acute Achilles tendon ruptures: a quantitative systematic review of randomized controlled trials. Am J Sports Med 40:2154–2160
Willits K, Amendola A, Bryant D, Mohtadi NG, Giffin JR, Fowler P, Kean CO, Kirkley A (2010) Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation. J Bone Joint Surg Am 92:2767–2775
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hansen, M.S., Christensen, M., Budolfsen, T. et al. Achilles tendon Total Rupture Score at 3 months can predict patients’ ability to return to sport 1 year after injury. Knee Surg Sports Traumatol Arthrosc 24, 1365–1371 (2016). https://doi.org/10.1007/s00167-015-3974-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3974-0