
Abstract
Purpose
An anatomical study was performed to assess the feasibility of arthroscopic visualization of the lateral ligaments of the ankle.
Methods
The fibular, talar and calcanear insertions of the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) were identified by standard arthroscopy portals. After dissection of the ATFL and CFL, bone tunnels were created at the estimated centres of their footprints. Dissection was then performed to identify the footprints and their position in relation to bony landmarks. The distance from the real centre of the footprint to the corresponding tunnel entrance was measured.
Results
Fourteen fresh frozen ankles were included. The ATFL and CFL were identified in all cases. The centre of the fibular ATFL footprint was found to be 16.1 ± 3.5 mm from the tip of the fibula, and the talar footprint was 18.4 ± 2.8 mm from the apex of the lateral talar process. The centre of the fibular CFL footprint was 4.2 ± 0.8 mm from the tip of the fibula, and the calcaneal footprint was 18.4 ± 2.5 mm from the fibular process of the calcaneum. The fibular tunnel was 2.9 ± 3 mm proximally from the centre of the ATFL fibular footprint, the talar tunnel was 4.4 ± 3.2 mm proximally from the centre of the talar footprint, and the calcaneal tunnel was 3.3 ± 2.8 mm too anterior from the CFL calcaneal footprint. No iatrogenic lesions were noted.
Conclusion
Arthroscopic identification of the ATFL, CFL and their corresponding footprints can be considered safe and reliable. Tunnels entrances, in preparation for arthroscopic ligament reconstruction, are precisely positioned. Arthroscopic anatomical ligament reconstruction is a feasible option.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic lateral ankle instability is a result of one or more ankle sprains. Chronic instability includes mechanical laxity [7, 14] (due to lengthening and/or tearing of the lateral ankle ligaments) functional or perceived instability [4, 7] (due to the relative loss of proprioceptive control and lack of use of periarticular muscles) and recurrent sprains [8]. The anterior talofibular ligament (ATFL) is the most frequently involved ligament of instability followed by the calcaneofibular ligament (CFL). Recent advances in arthroscopy have made it possible to treat most of the intraarticular lesions of the ankle associated with chronic instability such as anterior impingement, osteochondral lesions of the talar dome and the removal of foreign bodies or ossicles. Arthroscopic exploration of the ankle should be performed before beginning any stabilization or lateral ligament reconstruction procedures [6]. Recently, certain arthroscopic ankle stabilization procedures have been described and developed from the Broström-Gould procedure combining ligament repair and augmentation using the inferior extensor retinaculum [3, 11]. Autograft ligament reconstruction is recommended in patients with a high demand on the ankle such as overweight patients or high-level athletes. Better results could be expected with anatomical reconstruction which preserves natural ankle kinematics [6, 10]. Even though arthroscopic procedures for lateral ligament reconstruction are being developed, there are very few studies in the literature on the anatomy of the insertions of the lateral ligaments of the ankle. The aim of the present anatomical study was to describe a reliable arthroscopic procedure to assess both ATFL and CFL footprints.
Materials and methods
Fourteen ankles from ten fresh frozen cadavers (mean age, 81 ± 11 years) without ankle scars or obvious preexisting laxity were used for the present study. The same junior surgeon without extensive experience in ankle arthroscopy performed all procedures.
Surgical technique
First anterior ankle arthroscopy was performed using a standard 4.0-mm arthroscope and standard anteromedial and anterolateral portals with the ankle in the supine position without distraction. Anterolateral debridement of the ankle joint was performed with a 4.5-mm shaver, with visualization from the anteromedial portal.
Step 1: visualization of the ATFL (Figs. 1, 2)
The fibular insertion of ATFL was located by dissecting the distal fascicle of the anteroinferior tibiofibular (AITFL) ligament from the tibia to the anterior aspect of the lateral malleolus. A triangular space always appeared between the distal AITFL and the proximal ATFL. This triangular space was gradually debrided from the malleolus to the talus to visualize the superior edge of the ATFL. The talar insertion of the ATFL was then located on the lateral edge of the talar neck, just distal from an anterolateral zone of the talar dome without cartilage. A third instrumental portal was then created at the sinus tarsi. Dissection of the superficial part and distal edge of the ATFL was then performed with a blunt trocart and shaver from the sinus tarsi portal. The entire ATFL could then be evaluated, and the limits of both fibular and talar footprints were identified with a peak.

Visualization and palpation of the ATFL partially resected. AITFL remnant fibres of the anteroinferior tibiofibular ligament, FIATFL fibular insertion of the ATFL

Visualization and palpation of the anterior aspect of the ATFL. TIATFL talar insertion of the ATFL
Step 2: visualization of the CFL (Figs. 3, 4)
The ATFL was dissected from its fibular insertion, opening the anterior talofibular space and allowing visualization of the CFL. Debridement of the malleolar groove was performed with the arthroscope in the anterolateral portal from an anterior position at the sinus tarsi to a posterior position along the subtalar joint. The CFL was visualized crossing the talofibular space from the tip of the malleolus on the lateral side to the calcaneal wall on the medial side. Distally, the peroneal tendon sheaths were open where they cross the CFL. Thus, the entire CFL was visualized and the limits of both the fibular and calcaneal footprints were assessed with a peak.

Visualization and palpation of the CFL. FICFL fibular insertion of the CFL

Visualization of the CFL (outlined) lateral to the subtalar joint and medial to the fibular tendons
Step 3: assessment of footprint centres
A hole was drilled with a 2.8-mm drill at the estimated centres of each footprint defining tunnel positions for anatomical ATFL and CFL reconstruction with a tendon graft. Because the ATFL and CFL have a confluent footprint on the anterior border of the distal fibula, the footprint centres are very close making it impossible to drill one hole for each fibular footprint [12]. Thus, the fibular ATFL and CFL footprints were treated as a single footprint and the hole was drilled at the estimated centre of the confluent footprint.
Measurements
All iatrogenic lesions (chondral, neurovascular, tendinous) were identified during open anatomical dissection performed after the arthroscopic procedure. All measurements were performed using a call with a reading error of 0.5 mm. Data are presented as mean ± standard error. The anatomical ATFL and CFL footprint centres were identified following open dissection. The distance of the anatomical footprint centres from anatomical landmarks was then assessed (in mm):
-
the distance between the fibular ATFL anatomical footprint centre and the tip of the lateral malleolus,
-
the distance between the talar ATFL anatomical footprint centre and the apex of the lateral talar process,
-
the distance between the fibular CFL anatomical footprint centre and the tip of the lateral malleolus,
-
the distance between the calcaneal CFL anatomical footprint centre and the apex of the fibular calcaneal process.
The arthroscopic ATFL and CFL footprint centres were defined as the centres of the segments between the marks made during arthroscopic dissection. The following measurements were then made to evaluate the gap between the anatomical and arthroscopic footprint centres and the anatomical footprint centres and the drill holes (representing the estimated footprint centres during arthroscopy) including:
-
the distance between the arthroscopic fibular ATFL footprint centre and the anatomical fibular ATFL footprint centre,
-
the distance between the arthroscopic talar ATFL footprint centre and the anatomical talar ATFL footprint centre.
-
the distance between the arthroscopic fibular CFL footprint centre and the anatomical fibular CFL footprint centre.
-
the distance between the arthroscopic calcaneal CFL footprint centre and the anatomical calcaneal CFL footprint centre,
-
the distance between the fibular ATFL and CFL drill hole and the anatomical fibular ATFL footprint centre,
-
the distance between the talar ATFL drill hole and the anatomical talar ATFL footprint centre,
-
the distance between the fibular ATFL and CFL drill hole and the anatomical fibular CFL footprint centre, and
-
the distance between the calcaneal CFL drill hole and the anatomical calcaneal CFL footprint centre.
Results
The procedure was successfully performed in all ankles, and both the ATFL and CFL were visualized in all cases. The ATFL and CFL always appeared intact during arthroscopic exploration and palpation. No iatrogenic neurovascular, chondral or tendinous lesions were identified based on careful inspection of superficial peroneal nerve, the dorsal pedis artery, peroneal and extensor digitorum tendons and talar and subtalar cartilage during open anatomical dissection following the arthroscopic procedure.
ATFL
The centre of the ATFL fibular insertion was 16.1 ± 3.5 mm from the tip of the lateral malleolus. The centre of the ATFL talar insertion was 18.4 ± 2.8 mm from the apex of the lateral talar process (Fig. 5). The gap between the arthroscopic and anatomical fibular ATFL footprints was 1.7 ± 1.8 mm proximally. The gap between the arthroscopic and anatomical talar ATFL footprint centres was 1.5 ± 1.7 mm anteriorly (Fig. 6).

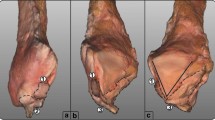
Lateral view of a right ankle showing the distances between anatomical landmarks and the centre of the ATFL in mm. The white star shows the constant anterolateral zone of the talar dome with no cartilage, AITFL anteroinferior tibiofibular ligament, CFL calcaneofibular ligament

Gap between anatomical footprint centres (black dots) and arthroscopic centres (black squares) of the anterior talofibular ligament (in mm)
CFL
The centre of the CFL fibular insertion was 4.2 ± .8 mm from the tip of the lateral malleolus. The centre of the CFL calcaneal insertion was 18.4 ± 2.5 mm from the apex of the fibular process of the calcaneus (Fig. 7). The gap between the arthroscopic and anatomical centres of the fibular CFL footprint was 1.4 ± 1.4 mm proximally. The gap between the arthroscopic and anatomical calcaneal CFL footprint centres was 4.1 ± 2.2 mm proximally and anteriorly (Fig. 8).

Lateral view of the distances between anatomical landmarks and the centre of the CFL ligament in a right ankle (in mm)

Gap between anatomical footprint centres (black dots) and arthroscopic centres (black squares) of the calcaneofibular ligament (in mm)
Tunnels
The gap between the fibular anatomical footprint centre and the fibular tunnel position was 2.9 ± 3 mm proximally. The gap between the talar ATFL anatomical footprint centre and the talar tunnel position was 4.4 ± 3.2 mm anteriorly. The gap between the calcaneal CFL anatomical footprint centre and the calcaneal tunnel position was 3.3 ± 2.8 mm anteriorly and proximally (Fig. 9).

Gap, in mm, between footprints centres (black dots) and tunnel entry points (grey dots)
Discussion
The main finding of this cadaveric study is that both the ATFL and CFL can be easily visualized by a simple 3-portal arthroscopic procedure of the anterior ankle. The arthroscopic technique of lateral ankle ligament dissection in the present study appears relatively easy and does not require extensive experience in ankle arthroscopy because it was performed by a resident in orthopaedic surgery. The technique is safe and reliable as long as the different steps are followed as described. The third instrumental sinus tarsi portal is highly important to obtain complete dissection of the lateral part of the hindfoot and accurate assessment of both the ATFL and CFL, providing control of the peroneal tendons and drilling of the fibular and calcaneal tunnels for anatomical ligament reconstruction using a tendon graft.
The first landmark is the superior edge of the ATFL, which is normally taut between the anterior distal fibula and the superolateral edge of the talar neck, preventing access to the talofibular space and visualization of the CFL. Thus, easy visualization of the CFL during anterior ankle arthroscopy suggests a complete ATFL tear. In these cases, the superior edge of the ATFL is lacking, replaced by significant capsuloligamentous distension. Thorough evaluation of the ATFL is best performed after dissection through the sinus tarsi portal with a blunt trocart to separate the superficial ATFL and extensor retinaculum from the subcutaneous layer. The entire ATFL can then be visualized, and its thickness, strength and tightness can be evaluated by palpation with a probe. Arthroscopic ATFL assessment seems to be an interesting decision-making decision tool to determine the best surgical option to treat chronic ankle instability (ATFL repair or ligament reconstruction) depending on the mechanical condition of the ATFL [13].
Following ATFL removal, the CFL is easily identified with the scope in the anterolateral portal and lateral debridement is performed with the shaver in the sinus tarsi portal. It is important to keep the shaver in contact with the bone and gradually visualize the different landmarks from anterior to posterior:
-
the sinus tarsi and lateral aspect of the posterior subtalar joint on the medial side,
-
the tip of the lateral malleolus on the lateral side,
-
the CFL seen as a rope-like ligament crossing from the tip of the fibula to the calcaneus in an oblique direction from anterior and proximal to posterior and medial,
-
and the peroneal tendons crossing the CFL distally.
The sheath of the peroneal tendons should be opened where they cross the CFL to visualize the calcaneal CFL footprint by distal and posterior debridement with the shaver, pushing back the tendons laterally with the rotating blade placed medially.
The position of ATFL and CFL footprints found in the present series were similar to those in previous anatomical studies [1, 2, 9, 12]. Although it was impossible to identify two or more bundles in the ATFL during arthroscopy and after open dissection because the ATFL was cut and removed during the arthroscopic procedure [5, 12], it can be noted that the ATFL talar footprint extends from the superolateral edge of the talar neck to the anterior lateral talar process [12, 15]. The arthroscopic results of this study confirm that the ATFL and CFL have a single confluent fibular footprint on the anterior distal fibula [12]. The present study shows that arthroscopic assessment of the ATFL and CFL footprints is excellent with a mean error of <2 mm except for the calcaneal CFL footprint with an error of 4 mm. The reduced accuracy for the calcaneal CFL footprint is mainly due to insufficient debridement, which was limited to the anterior CFL calcaneal insertion. More extensive dissection was necessary.
The hypothesis was that the tunnels for graft fixation during arthroscopic anatomical ATFL and CFL reconstruction should be placed in the footprint centres. The results of the present study and anatomical studies in the literature confirm that a single fibular tunnel for both the ATFL and CFL graft is logical and technically easier because these two ligaments have a confluent fibular footprint. Thus, the fibular tunnel should not be mid-distance from the anterior distal fibula because this is the location of the ATFL fibular footprint centre [2]. The common ATFL and CFL fibular tunnel should be drilled at a distal third of the anterior distal fibula from the sinus tarsi portal. The positioning error for the fibular tunnel with this technique is 3 mm too proximally from the fibular footprint centre, so the tunnel should be drilled as distally as possible. The position of the ATFL talar tunnel is more difficult to determine because the talar footprint is at a distance from the superolateral edge of the talar neck up to the anterior part of the lateral talar process. The mean positioning error for the ATFL talar tunnel is 4.4 mm too proximally. Thus, this tunnel should be placed more distally on the lateral aspect of the talar neck and drilled from the anterolateral portal in the direction of the talar body to avoid talar neck fractures on the dorsal cortex. The mean error for the positioning of the calcaneal CFL tunnel was 3.3 mm anteriorly, and thus, more posterior complete debridement should be performed and the tunnel should be placed in a more posterior position. The soft tissues should be protected during this step including a guide to push the peroneal tendons laterally. The calcaneal tunnel could also be created through another posterolateral portal with a guide applied on the calcaneal footprint centre. However, this technique was not tried in the present study.
The main limitation of this study was that the procedures were performed by only one surgeon. Further anatomical studies are needed to confirm the reliability of this arthroscopic technique for the dissection of the ATFL and CFL. The clinical relevance of this study is that new arthroscopic techniques of lateral ligament repair or reconstruction can be safely and accurately developed and improved.
Conclusion
Arthroscopic identification of the ATFL, CFL and their respective footprints is safe and reliable. Tunnels entrances, in preparation for arthroscopic ligament reconstruction, are precisely positioned. Arthroscopic anatomical ligament reconstruction is a feasible option.
References
Burks RT, Morgan J (1994) Anatomy of the lateral ankle ligaments. Am J Sports Med 22:72–77
Clanton TO, Campbell KJ, Wilson KJ, Michalski MP, Goldsmith MT, Wijdicks CA, LaPrade RF (2014) Qualitative and quantitative anatomic investigation of the lateral ankle ligaments for surgical reconstruction procedures. J Bone Joint Surg Am 96:e98
Cottom JM, Rigby RB (2013) The “All Inside” arthroscopic Broström procedure: a prospective study of 40 consecutive patients. J Foot Ankle Surg 52:568–574
Freeman MAR (1965) Treatment of ruptures of the lateral ligament of the ankle. J Bone Joint Surg Br 47:661–668
Golanó P, Vega J, de Leeuw PAJ, Malagelada F, Manzanares MC, Götzens V, van Dijk CN (2010) Anatomy of the ankle ligaments: a pictorial essay. Knee Surg Sports Traumatol Arthrosc 18:557–569
Guillo S, Bauer T, Lee JW, Takao M, Kong SW, Stone JW, Mangone PG, Molloy A, Perera A, Pearce CJ, Michels F, Tourné Y, Ghorbani A, Calder J (2013) Consensus in chronic ankle instability: aetiology, assessment, surgical indications and place for arthroscopy. Orthop Traumatol Surg Res 99:S411–S419
Hertel J (2002) Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J Athl Train 37:364–375
Hiller CE, Kilbreath SL, Refshauge KM (2011) Chronic ankle instability: evolution of the model. J Athl Train 46:133–141
Khawaji B, Soames R (2015) The anterior talofibular ligament: a detailed morphological study. Foot (Edinb) 25:141–147
Krips R, van Dijk CN, Lehtonen H, Halasi T, Moyen B, Karlsson J (2002) Sports activity level after surgical treatment for chronic anterolateral ankle instability. A multicenter study. Am J Sports Med 30:13–19
Nery C, Raduan F, Del Buono A, Asaumi ID, Cohen M, Maffulli N (2011) Arthroscopic-assisted Brostrom-Gould for chronic ankle instability: a long-term follow-up. Am J Sports Med 39:2381–2388
Neuschwander TB, Indresano AA, Hughes TH, Smith BW (2013) Footprint of the lateral ligament complex of the ankle. Foot Ankle Int 34:582–586
Takao M, Innami K, Matsushita T, Uchio Y, Ochi M (2008) Arthroscopic and magnetic resonance image appearance and reconstruction of the anterior talofibular ligament in cases of apparent functional ankle instability. Am J Sports Med 36:1542–1547
Tropp H, Odenrick P, Gillquist J (1985) Stabilometry recordings in functional and mechanical instability of the ankle joint. Int J Sports Med 6:180–182
Wenny R, Duscher D, Meytap E, Weninger P, Hirtler L (2015) Dimensions and attachments of the ankle ligaments: evaluation for ligament reconstruction. Anat Sci Int 90:161–171
Acknowledgments
The authors would like to thank sincerely Mr. Jean Thès for his drawings.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Thès, A., Klouche, S., Ferrand, M. et al. Assessment of the feasibility of arthroscopic visualization of the lateral ligament of the ankle: a cadaveric study. Knee Surg Sports Traumatol Arthrosc 24, 985–990 (2016). https://doi.org/10.1007/s00167-015-3804-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3804-4