
Abstract
Purpose
The purpose of the study is to identify the safe zone in which the surgeon can place the screws for fixation of the coracoid graft during the Latarjet procedure to avoid injuries of the suprascapular nerve with the shoulder in internal and external rotation.
Methods
The dissection on twelve fresh-frozen shoulders was performed according to a standard posterior approach to the gleno-humeral joint. The suprascapular nerve and its branches for the infraspinatus muscle were identified at the spinoglenoid notch region. Then, the distance between the glenoid and the suprascapular nerve at the spinoglenoid notch region was measured by using a ruler with the shoulder at 90° internal rotation and at 90° of external rotation.
Results
The median distance between the glenoid and the suprascapular nerve was 12 mm (range 6–15 mm) with the shoulder at 90° of internal rotation and 19 mm (range 11–23 mm) with the shoulder at 90° of external rotation. The distance between the glenoid and the suprascapular nerve was statistically significantly greater with the shoulder at 90° of external rotation than 90° of internal rotation (P = 0.002).
Conclusions
The suprascapular nerve is furthest away from the glenoid with the shoulder at 90° of external rotation. Therefore, the placement of screws in external rotation of the humerus during glenoid bone block procedures likely reduces the risk of iatrogenic injuries of the suprascapular nerve.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Significant bony defects of glenoid and humeral head modify the congruency of glenohumeral joint surfaces and could result in recurrent dislocations of the shoulder [2]. The management of the bone loss in traumatic anterior glenohumeral instability is extremely challenging [9]. It is generally accepted that a glenoid bone loss >25 % should be managed by reconstruction with bone graft, Bristow or Latarjet procedures [13]. Both Bristow and Latarjet techniques involve transfer of the coracoid and the attached conjoint tendon to the anterior scapular neck at the antero-inferior glenoid rim. The bony augmentation allows to increase the arc of the glenoid and therefore the congruency of the joint. Arthroscopic bone block procedures have also been described [15, 16].
Given its good results, the use of Latarjet and others’ bony procedures has increased in the last decade to manage patients with shoulder instability associated with significant bony defects [3, 6, 8, 9]. The coracoid graft is usually fixed to the antero-inferior aspect of the glenoid with bicortical screws exiting on the posterior aspect of the scapula. For this reason, although suprascapular nerve injury is a rare complication of shoulder surgery, it can occur after the Latarjet procedure [10]. The suprascapular nerve enters in the supraspinatus fossa by passing under the transverse scapular ligament at the scapular notch and provides motor branches for the innervation of the supraspinatus muscle. Then, it courses distally passing in the spinoglenoid notch at the base of the scapular spine and enters in the infraspinatus fossa to provide motor branches for the innervation of the infraspinatus muscle [14]. Because the suprascapular nerve runs along the posterior aspect of the scapula, it is potentially vulnerable to injury during glenohumeral procedures involving placement of screws in the neck of the scapula. Moreover, the normal course of the suprascapular nerve is modified when rotator cuff tears occur [12]. Injuries to the suprascapular nerve have been reported during surgery for shoulder instability, up to 6 % [9].
Recently, a study from Ladermann et al. [7] firstly evaluated the relation between the screws securing the coracoid graft and the suprascapular nerve. To our knowledge, no study evaluated the extension of the safe zone in the internal and external rotation of the shoulder.
The aim of this study was to identify the safe zone, with the shoulder in internal and external rotation, in which surgeon can place the screws for the fixation of the coracoid graft during Latarjet procedure to avoid injuries of the suprascapular nerve. This study aimed therefore to evaluate the extension of the safe zone in a dynamic fashion to detect the safer position of the shoulder during the placement of the screws in Latarjet procedure. We hypothesized that there was no difference in terms of extension of the safe zone between internal- and external-rotated positions of the shoulder.
Materials and methods
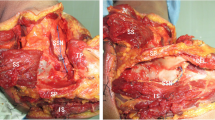
Twelve fresh-frozen shoulders with unknown history of disease or trauma to the shoulder were used. Shoulders with any evidence of rotator cuff tear at gross examination were excluded from the study. There were six male and six female cadavers with a median age of 59 years (range 52–82). The dissection was performed according to a standard posterior approach to the gleno-humeral joint. After the exposure of the infraspinatus and teres minor muscles, the suprascapular nerve was identified at the spinoglenoid notch region. The branches innervating the infraspinatus muscle were also identified on the inferior aspect of the muscle with a gentle dissection without detaching the tendon of the infraspinatus muscle from its insertion on the humerus. Then, the distance between the glenoid and the suprascapular nerve at the spinoglenoid notch region was measured by using a ruler with the shoulder at 90° internal rotation and at 90° of external rotation (Fig. 1). The glenoid can be defined as a shallow pear-shaped cavity covered with articular cartilage. It is located on the lateral angle of the scapula and articulates with the head of the humerus. At the end, the scapula was obtained in all specimens and the following measurements were performed: the length of the scapula’s superior border (a) and the maximum length of the antero-posterior diameter of the glenoid (b). For each specimen, two examiners performed all the measurements two times in blind fashion.

The distance between the glenoid and the suprascapular nerve at the spinoglenoid notch region (c) was measured by using a ruler with the shoulder at 90° internal rotation and at 90° of external rotation. The length of the scapula’s superior border (a) and the maximum length of the antero-posterior diameter of the glenoid (b) were also measured
Statistical analysis
Data were recorded in a computer database and analyzed using SPSS for Mac (version 16.0, SPSS Inc, Chicago, IL, USA). Descriptive statistics were calculated reporting frequencies and percentages for discrete data and medians with range of values for continuous data.
Analysis of the relationship between the distance from the glenoid to the suprascapular nerve and the length of the scapula’s superior border (a) and the maximum length of the antero-posterior diameter of the glenoid (b) was performed, calculating the Spearman rank order correlation coefficient (r).
Analysis of the intra- and inter-tester agreement was performed with the intra-class correlation coefficient (ICC) with 95 % of confidence interval (CI), ranging between 0.0 and 1.0.
The Wilcoxon signed-rank test was performed to compare the measurements of the distance between the glenoid and the suprascapular nerve achieved with the shoulder at 90° of internal and external rotation. Finally, the Wilcoxon–Mann–Whitney test was performed to compare the distance between the glenoid and the suprascapular nerve in males and females in both internal and external rotation. Because of the small number of cadavers, it has been assumed that the values were not normally distributed. For this reason, nonparametric statistical tests were selected. A P value of <0.05 was considered significant.
Results
None of the specimens included in the present study showed any evidence of rotator cuff tear at gross examination.
In all specimens, the suprascapular nerve was identified at the spinoglenoid notch region. The median distance between the glenoid and the suprascapular nerve was 12 mm (range 6–15 mm) with the shoulder at 90° of internal rotation and 19 mm (range 11–23 mm) with the shoulder at 90° of external rotation. The distance between the glenoid and the suprascapular nerve was statistically significantly greater with the shoulder at 90° of external rotation than 90° of internal rotation (P = 0.002).
In male samples, the median distance between the glenoid and the suprascapular nerve was 12 mm (range 6–15 mm) with the shoulder at 90° of internal rotation and 19 mm (range 17–23 mm) with the shoulder at 90° of external rotation (P = 0.026). In female samples, the median distance between the glenoid and the suprascapular nerve was 10 mm (range 6–13 mm) with the shoulder at 90° of internal rotation and 18 mm (range 11–20 mm) with the shoulder at 90° of external rotation (P = 0.027). The comparison between the distances measured in both gender did not show any significant difference in both internal (n.s.) and external (n.s.) rotation.
In all specimens, the median length of the scapula’s superior border was 111 mm (range 95–118 mm) and the median maximum length of the antero-posterior diameter of the glenoid was 30 mm (range 22–33 mm). The distance from the glenoid to the suprascapular nerve did not correlate with the length of the scapula’s superior border (a) and the maximum length of the antero-posterior diameter of the glenoid (b) in both internal rotation (r = 0.07 and r = −0.15, respectively) and external rotation (r = 0.18 and r = −0.14, respectively) of the shoulder.
Finally, the measurements performed by two examiners showed a very good inter-tester agreement: shoulder in external rotation: ICC 0.98 (95 % CI 0.94–0.99), shoulder in internal rotation: ICC 0.98 (95 % CI 0.95–0.99) and intra-tester agreement; observer 1; shoulder in external rotation: ICC 0.98 (95 % CI 0.93–0.99), shoulder in internal rotation: ICC 0.99 (95 % CI 0.97–0.99); observer 2; shoulder in external rotation: ICC 0.97 (95 % CI 0.91–0.99), shoulder in internal rotation: ICC 0.99 (95 % CI 0.96–0.99).
Discussion
The main finding of this study is that the suprascapular nerve was significantly further away from the glenoid when the shoulder is held at 90° of external rotation compared with 90° of internal rotation. Thus, the posterior safe area of the neck of the scapula, where the screws for the fixation of the coracoid graft should be placed, is greatest in external rotation.
In the last decades, cadaveric studies have been performed to define the safe zone in the posterior aspect of the neck of the scapula to avoid suprascapular nerve injuries [1, 4, 5, 7, 11, 14].
Ebraheim et al. [4] performed an anatomic study using a posterior approach to the scapula with the shoulder in neutral position. They showed that the suprascapular neurovascular bundle was at an average of 14 mm from the glenoid rim, where it is adherent to the spinoglenoid angle of the scapula. Dynamic measurements were performed showing that the median distance between the glenoid and the suprascapular nerve was 12 and 19 mm with the shoulder at 90° of internal and external rotation, respectively.
Although some authors showed that gender and scapular dimensions influence the extension of the safe zone [5], we found that the distance between the glenoid and the suprascapular nerve did not correlate with the length of the scapula’s superior border and the maximum length of the antero-posterior diameter of the glenoid. Moreover, no differences between males and females in terms of distance between the glenoid and the suprascapular nerve were found in both internal and external rotation. On the other hand, the subgroup analysis confirmed that the safe zone is significantly wider with the shoulder in external position in both gender.
Some authors defined the safe zone by investigating the insertion angle of wires in the neck of the scapula. Bigliani et al. [1] used three pins that were drilled in anterior–posterior direction with different angles at the middle of the glenoid neck just inferior and lateral to the base of the coracoid process. The pin passed in a cranio-caudal direction was the furthest away from the suprascapular nerve at the spinoglenoid notch region with an average distance of 16 mm. Shishido et al. [14] evaluated the safe zone by measuring the insertion angle of a Kirschner wire toward the suprascapular nerve at the base of the scapular spine. The average values of the insertion angle were 37 and 17.5° spine in the transverse and sagittal planes, respectively. The Kirschner wire drilled toward the bifurcation of the infraspinatus motor branch had average insertion angles of 44.3 and 27.7° in the transverse and sagittal planes, respectively.
Recently, a study from Ladermann et al. [7] firstly evaluated the relation between the specific exit point of the screws securing the coracoid graft and the suprascapular nerve during the Latarjet procedure. The authors concluded that the proximity of the suprascapular nerve to the posterior glenoid rim puts this nerve at risk during insertion of the screws used for the Latarjet procedure and recommended to place the screw within 10° of the face of the glenoid in the axial plane, which is safe and will avoid the potential for suprascapular nerve injury. In this study, the distance of the safe area of the posterior aspect of the neck of the scapula was examined in a static setting, suggesting shoulder surgeons to avoid iatrogenic injury to this nerve. Our study implements such information, adding data on dynamic evaluation of the nerve position. The main clinical implication of our study is that the arm should be held at 90° of external rotation when inserting the guidewires into cannulated screws to avoid damage to the suprascapular nerve. However, despite the posterior safe area of the neck of the scapula is grater in external rotation, we would highlight that the minimum distance between the glenoid and the suprascapular nerve is 11 mm.
To our knowledge, this is the first study to describe the posterior safe area of the suprascapular nerve in a dynamic fashion (internal and external rotation).
Strengths of this study were the homogeneity of the sample, as shoulders with any evidence of rotator cuff tear at gross examination were excluded from the study. Further strengths of the study include the fact that the extension of the safe area was determined in relation to the dimensions of the scapula and the glenoid width in the anterior–posterior dimension, and the results were consistent in all the specimens. Moreover, data achieved in males and females were compared.
This study has some limitations. Differences in the safe zone between cadaveric and live patient’s shoulders or between passive and active motion may exist. However, the cadaveric nature of this study did not allow us to detect such potential differences. We are also aware that the sample size is small, but there is a limited availability of cadavers, and we used all specimens we were able to enroll. Moreover, a post hoc power analysis on our results was performed, showing a power of 0.71 to detect a significant difference at 5 % significance level.
Massimini et al. [12] showed that the normal course of the suprascapular nerve changes when rotator cuff tears occur. In the present study, only specimens without any evidence of rotator cuff tear at gross examination were included to examine a more homogenous sample and to avoid potential bias. The course of the suprascapular nerve in internal and external rotation in specimens with rotator cuff tears could be assessed in future studies.
On the basis of the present study, we recommend to hold the shoulder at 90° of external rotation during the placement of screws in glenoid bone block procedures to reduce the risk of iatrogenic injuries of the suprascapular nerve.
Conclusions
The present study compared the distance between the glenoid and the suprascapular nerve at the spinoglenoid notch region in fresh-frozen shoulders. The suprascapular nerve is furthest away from the posterior edge of the glenoid with the shoulder at 90° of external rotation. Thus, the posterior safe area of the neck of the scapula is the greatest in external rotation.
References
Bigliani LU, Dalsey RM, McCann PD, April EW (1990) An anatomical study of the suprascapular nerve. Arthroscopy 6:301–305
Bollier MJ, Arciero R (2010) Management of glenoid and humeral bone loss. Sports Med Arthrosc 18:140–148
Burkhart SS, De Beer JF, Barth JR, Cresswell T, Roberts C, Richards DP (2007) Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss. Arthroscopy 23:1033–1041
Ebraheim NA, Mekhail AO, Padanilum TG, Yeasting RA (1997) Anatomic considerations for a modified posterior approach to the scapula. Clin Orthop Relat Res 334:136–143
Gumina S, Albino P, Giaracuni M, Vestri A, Ripani M, Postacchini F (2011) The safe zone for avoiding suprascapular nerve injury during shoulder arthroscopy: an anatomical study on 500 dry scapulae. J Shoulder Elbow Surg 20:1317–1322
Hovelius L, Sandstrom B, Olofsson A, Svensson O, Rahme H (2012) The effect of capsular repair, bone block healing, and position on the results of the Bristow–Latarjet procedure (study III): long-term follow-up in 319 shoulders. J Shoulder Elbow Surg 21:647–660
Ladermann A, Denard PJ, Burkhart SS (2012) Injury of the suprascapular nerve during Latarjet procedure: an anatomic study. Arthroscopy 28:316–321
Lafosse L, Lejeune E, Bouchard A, Kakuda C, Gobezie R, Kochhar T (2007) The arthroscopic Latarjet procedure for the treatment of anterior shoulder instability. Arthroscopy 23:1242 e1241–1242 e1245
Longo UG, Loppini M, Rizzello G, Romeo G, Huijsmans PE, Denaro V (2013) Glenoid and humeral head bone loss in traumatic anterior glenohumeral instability: a systematic review. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-013-2403-5
Maquieira GJ, Gerber C, Schneeberger AG (2007) Suprascapular nerve palsy after the Latarjet procedure. J Shoulder Elbow Surg 16:e13–e15
Marsland D, Ahmed HA (2011) Arthroscopically assisted fixation of glenoid fractures: a cadaver study to show potential applications of percutaneous screw insertion and anatomic risks. J Shoulder Elbow Surg 20:481–490
Massimini DF, Singh A, Wells JH, Li G, Warner JJ (2012) Suprascapular nerve anatomy during shoulder motion: a cadaveric proof of concept study with implications for neurogenic shoulder pain. J Shoulder Elbow Surg 22:463–470
Provencher MT, Bhatia S, Ghodadra NS, Grumet RC, Bach BR Jr, Dewing CB, LeClere L, Romeo AA (2010) Recurrent shoulder instability: current concepts for evaluation and management of glenoid bone loss. J Bone Joint Surg Am 92(Suppl 2):133–151
Shishido H, Kikuchi S (2001) Injury of the suprascapular nerve in shoulder surgery: an anatomic study. J Shoulder Elbow Surg 10:372–376
Sugaya H, Moriishi J, Kanisawa I, Tsuchiya A (2006) Arthroscopic osseous Bankart repair for chronic recurrent traumatic anterior glenohumeral instability. Surgical technique. J Bone Joint Surg Am 88(Suppl 1 Pt 2):159–169
Taverna E, Golano P, Pascale V, Battistella F (2008) An arthroscopic bone graft procedure for treating anterior-inferior glenohumeral instability. Knee Surg Sports Traumatol Arthrosc 16:872–875
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Longo, U.G., Forriol, F., Loppini, M. et al. The safe zone for avoiding suprascapular nerve injury in bone block procedures for shoulder instability. A cadaveric study. Knee Surg Sports Traumatol Arthrosc 23, 1506–1510 (2015). https://doi.org/10.1007/s00167-014-2900-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-014-2900-1