
Abstract
Purpose
Femoral osteotomies are the preferred treatment in significant torsional deformity of the femur. The influence of torsional osteotomies on frontal plane alignment is poorly understood. Therefore, the aim of the present study was to evaluate the effects of external derotational osteotomies on proximal, mid-shaft and distal levels onto frontal plane alignment.
Methods
The effect of rotation around the anatomical axis of the femur on frontal plane alignment was determined with a 3D computer model, created from CT data of a right human cadaver femur. Virtual torsional osteotomies of 10°, 20° and 30° were performed at proximal, mid-shaft and distal levels under five antecurvatum angles of the femur. The change of the frontal plane alignment was expressed by the mechanical lateral femoral angle.
Results
Proximal derotational osteotomies resulted in an increased mechanical lateral distal femoral angle (mLDFA) of 0.8°–2.6° for 10°, of 1.6°–5.1° for 20° and of 2.3–7.9° for 30° derotational osteotomy, indicating an increased varus angulation. Supracondylar derotational osteotomy resulted in a decreased mLDFA of −0.1° to −1.7° for 10°, of −0.2 to −3.7° for 20° and of −0.7 to −6.9° for 30° derotational osteotomy, indicating an increased valgus angulation. The effect increased with the amount of torsional correction and virtually increased antecurvatum angles. Mid-shaft torsional osteotomies had the smallest effect on frontal plane alignment.
Conclusion
This three-dimensional computer model study demonstrates the relationship between femoral torsional osteotomies and frontal plane alignment. Proximal external derotational osteotomies tend to result in an increased varus angulation, whilst distal external derotational osteotomies tend to result in an increased valgus angulation. As a clinical consequence, torsional osteotomies have an increased risk of unintentional implications on frontal plane alignment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Increased femoral anteversion is a common cause of anterior knee pain and patellofemoral instability [2–5, 13]. Increased femoral anteversion can cause increased lateral facet pressure and increased medial retinacular strain [13, 16, 17, 24]. Additionally, increased femoral anteversion can cause in-toeing with gait disturbance. In patients with concomitant developmental dysplasia of the hip, increased stress on the anterior labrum has been described in the literature [14, 22, 28]. Although most patients with persistent anteversion are asymptomatic and require no treatment [9, 15, 22], rotational osteotomy has to be considered when a significant torsional deformity is present. Femoral derotational osteotomy for persistent femoral anteversion is performed most commonly in older children and adolescents, as remodelling after this age is minimal [7, 21, 25].
An obvious question that arises for rotational osteotomies is the level at which to perform the osteotomy.
In the literature, numerous techniques at the proximal [12, 21], diaphyseal [8, 9, 26] or distal femur [2, 5, 6, 21] have been reported with good results. Proximal intertrochanteric osteotomies are usually secured with angle blade plates, and distal metaphyseal osteotomies are usually secured with plates, whereas diaphyseal osteotomies are typically secured with an intramedullary nail [2, 6, 8, 9, 21, 26, 28].
The literature provides no evidence whether a proximal, mid-shaft or distal location of the osteotomy is preferable [2, 21]. Indications for surgical treatment have been described in the literature, although the preferred level of osteotomy is still controversial, with some surgeons preferring distal and some proximal [6, 8, 9]. Paley [20] has emphasized that derotational osteotomies of the femur can cause malalignment in the frontal plane, because the mechanical and anatomical axes are different. However, no specifications of the amount of change at different levels were provided.
In reviewing the literature, there has been no evidence evaluating the effect of derotational osteotomies performed on three different levels on frontal plane alignment [2, 6, 9, 12]. Therefore, this study set out with the aim to evaluate the effects of torsional osteotomies on frontal plane alignment. It has been hypothesized that distal femoral external derotational osteotomies tend to create an increased valgus angulation and proximal external derotational osteotomies tend to create an increased varus angulation.
Materials and methods
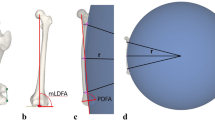
The effect of rotation around the anatomical axis of the femur on frontal plane alignment was determined with a 3D computer model (Fig. 1). The model was created from CT data of a right human cadaver femur using Simpleware software (Simpleware Ltd., Exeter, United Kingdom). The investigated femur had a length of 490 mm, the femoral anteversion was 19 and the projected neck-shaft angle was 128 (Fig. 1). In the literature, an average femoral anteversion angle of approximately 15° is reported; however, normal values depend on the method of measurement [7, 28].

Frontal view of the computer model. The mLDFA was 89°, and the neck-shaft angle was 128°
The degree of sagittal bowing was determined by measurement of the antecurvatum angle of the femur (ACA). In the investigated femur, the ACA was 7° which corresponds to a radius of 2.8 metres (curve in the sagittal plane). The mechanical lateral distal femoral angle (mLDFA) of the femur was 89° (Fig. 1).
An orthogonal anatomical coordinate system was defined via three anatomical landmarks (Fig. 2), which were the most distal location of the medial (LM1) and lateral (LM2) femoral condyle as well as the centre of the femoral head (LM3). The mechanical lateral femoral angle was determined according to Paley (Fig. 2) [19, 20]. The normal values for frontal plane mechanical axis deviation and mLDFA have been described [20]. To obtain an AP view, the most posterior locations of each condyle were kept aligned in the y and z direction.

a Frontal (left) and sagittal (right) view of the computer model. The landmarks LM1, LM2 and LM3 define an orthogonal anatomical coordinate system. VO1, VO2 and VO3 represent the levels of the virtual osteotomies (proximal, diaphyseal and distal). The mechanical femoral axis and the angles mLDFA and ACA are shown. b Frontal (left) and sagittal (right) view of the femur after external rotation of the distal fragment following osteotomy at level V01, showing the change of the landmarks and the change of the mLDFA, denoted as angle ϑ
Virtual osteotomies, as typically performed in clinical practice, were created at three different levels along the femoral axis (Fig. 2). The proximal osteotomy (VO1) was performed at the intertrochanteric, the mid-diaphyseal (VO2) and at the supracondylar level (VO3). The respective osteotomy plane was defined perpendicular to the anatomical axis of the femur. The distal part of the femur was then rotated internally and externally by 10°, 20° and 30° (Fig. 2b). The change of the frontal plane alignment was expressed by the mechanical lateral femoral angle. The change of the mLDFA was calculated as follows:
the subscripts x and z denote the respective coordinates of LM1 and LM2.
Positive ϑ values indicate an increased mLDFA, and negative ϑ values indicate a decreased mLDFA (Fig. 2).
In addition to the anatomical femoral antecurvatum angle of 7° (radius ~280 cm), four other antecurvatum angles were simulated in increments of 5° starting from the anatomical ACA of the investigated specimen: 12° (radius ~160 cm), 17° (radius ~120 cm), 22° (radius ~90 cm) and 27° (radius ~70 cm). All measurements were made to the tenth of a degree.
Results
The results are reported as change of the mLDFA after performing the osteotomies compared to the anatomical mLDFA of the specimen. The results are based on measurements with the patella pointing forward.
The effect of the performed virtual torsional osteotomy on the frontal plane depended on the level at which the osteotomy and rotation were performed and the magnitude of the antecurvatum angle of the femoral shaft.
Table 1 presents the results obtained from the analysis of external derotational (reduced femoral anteversion) and internal rotational osteotomies (increased femoral anteversion) at three different levels. It can be observed that the proximal external derotational osteotomies resulted in an increased mLDFA, whereas the proximal internal rotational osteotomies (increased femoral anteversion) resulted in a smaller mLDFA. The effect increased with the amount of torsional correction in either direction. At 7° antecurvatum angle, a 30° proximal external derotational osteotomy resulted in an increase in the mLDFA of 2.3°, indicating an increased varus alignment of the femur. The maximum effect of a proximal derotational osteotomy onto the frontal plane of 7.9° was found for a 30° derotational osteotomy and an antecurvatum angle of 27° (Table 1). A 30° proximal internal rotational osteotomy resulted in a decreased mLDFA of 3.5°, indicating an increased valgus alignment of the femur.
Simulating a distal supracondylar external derotational osteotomy (reduced femoral anteversion) of 10° resulted in no measurable change of the mLDFA at 7° antecurvation. A 30° supracondylar external derotational osteotomy resulted in a decreased mLDFA of 0.7° at 7° antecurvatum angle and of 2.1° at 12° antecurvatum angle. The maximum effect of a distal external derotational osteotomy onto the frontal plane of 6.3° decreased mLDFA was found for a 30° external derotational osteotomy and an antecurvatum angle of 27° (Table 1).
A 10° mid-diaphyseal derotational osteotomy resulted in no change of the mLDFA at all measured antecurvatum angles; 20° and 30° mid-diaphyseal derotational osteotomy resulted in a decreased mLDFA of less than 1° (Table 1).
The virtually increased antecurvatum angles of the femur aggravated the effect of torsional osteotomies on the mLDFA on the proximal and distal levels (Table 1).
Discussion
The main finding of the study is that torsional osteotomies of the femur can cause malalignment in the frontal plane, depending on the level of osteotomy, the amount of antecurvatum angle and the magnitude of derotation.
Proximal external derotational osteotomies performed to treat femoral anteversion resulted in an increased varus angulation due to an increased mLDFA. The opposite effect onto the frontal plane could be observed in distal osteotomies. Distal external derotational osteotomies resulted in an increased valgus angulation due to a decreased mLDFA.
The observed differences in the results can be explained as follows. Firstly, in the femur, the mechanical and anatomical axes are different [20]. Therefore, rotation around the anatomical axis has a different effect than that of a rotation around the mechanical axis. In proximal osteotomies, the malalignment created by derotation is caused by the change of length of the femoral neck projection in the frontal plane [21]. Internal rotation of the femoral neck (retroversion) produces a lengthening of the femoral neck in the frontal plane, which leads to an increased mLDFA and increased varus angulation and external rotation of the femoral neck (anteversion) produces a shortening of the femoral neck and accordingly decreased mLDFA. Similar to our results not only rotational osteotomies affect the frontal plane but also varus and valgus osteotomies of the proximal femur can affect femoral version. This has been shown in the paper of Liu et al. [18]. The study showed that a proximal intertrochanteric varus osteotomy is decreasing anteversion and a proximal valgus osteotomy is increasing anteversion. These results indirectly confirm the results of the present study, as a varus osteotomy implicates an increased mLDFA and a valgus osteotomy implicates a decreased mLDFA [18].
There has been no evidence in the literature investigating the effect of distal torsional osteotomies and the effect of the femoral antecurvatum angle onto frontal plane alignment.
In distal osteotomies, the effect on the frontal plane is different due to two predominant reasons. The mechanical axis passes through or close to the centre of rotation of the osteotomy in distal osteotomies; thus, the effect of external derotational osteotomies onto varus angulation is less.
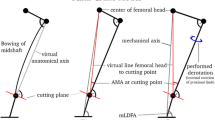
The second effect in distal osteotomies can even lead to an increased valgus angulation. The X-rays of a patient with a severely increased anteversion of the femur in Fig. 3 illustrate the different effects of proximal and distal derotational osteotomies onto the frontal plane. Due to the internal rotation of the femur, the femoral antecurvatum angle, which normally is in the sagittal plane, rotates into the frontal plane (Fig. 3a). The bowing can then be seen on the radiograph with the knees in compensatory functional internal rotation (Fig. 3a). The X-ray on Fig. 3b of the same leg with the patient advised to externally rotate the leg shows the real a.p. view of the femur. On the following figures, the different effects of simulated proximal and distal osteotomies on mLTFA can be seen (Fig. 3c, d).

The AP radiograph shows the medialized patella of a patient with increased femoral anteversion. Due to internal femoral rotation the distal femur is shown in oblique projection with apparent valgus angulation (a). The X-ray on b of the same leg with the patient advised to externally rotate the leg shows the real a.p. view of the femur. The green and yellow rectangles represent the level of the osteotomy as performed on c and d. In c, the simulated proximal derotational femoral osteotomy demonstrates the increased femoral neck offset and increased mLDFA. In d, the simulated distal derotational osteotomy demonstrates the increased femoral neck offset and additionally the persistent valgus deformity of the femoral shaft. Accordingly, the mLDFA is decreased
Performing a virtual proximal external derotational osteotomy (external rotation of the distal fragment), the neck-shaft angle decreases due to relative internal rotation of the proximal fragment. The lengthening of the femoral neck causes an increase in the mLDFA (Fig. 3c). Performing a distal osteotomy, the neck-shaft angle decreases less as the osteotomy is close to the mechanical axis, additionally the antecurvatum angle of the shaft is not derotated into the sagittal plane and remains in the frontal plane (Fig. 3d). These two effects are responsible for the decreased mLDFA and therefore increased valgus angulation in distal external derotational osteotomies.
Increased antecurvatum angles of the femur substantially aggravate the observed effects of both proximal and distal torsional osteotomies on the mLDFA.
In the literature, large variances of the femoral antecurvatum angle have been reported [11, 23, 27, 29]. Seo et al. [23] found a mean ACA of 13.9° (range 6.2°–24.5°). Harper and Carson [11] also found a wide range of ACA. The radius of curvature of the femurs ranged from 188.5 to 68.9 cm (average 114.4 cm). Assuming a virtual ACA of 17°, which equates a radius of 120 cm in our specimen, a proximal external derotational osteotomy of 30° leads to an increased varus alignment of 5.1°, whereas a distal external derotational osteotomy of 30° leads to an increased valgus alignment of 3.5°.
Assuming a virtual ACA of 22°, which equates a radius of 90 cm in our specimen a proximal external derotational osteotomy of 30° leads to an increased varus alignment of 6.5°, whereas a distal external derotational osteotomy of 30° leads to an increased valgus alignment of 4.9°.
These examples demonstrate that external derotational osteotomies in patients with increased sagittal increased femoral antecurvatum angle are prone to inadvertent effects on frontal plane alignment. In the literature, increased ACA is very common in the normal population. Therefore, in patients with clinical signs of increased ACA, radiographic evaluation of the sagittal plane has to be considered before planning a torsional osteotomy.
The least implications onto the frontal plane were seen at mid-shaft diaphyseal osteotomies. In mid-shaft diaphyseal osteotomies, the two opposite effects of proximal and distal osteotomies are most likely neutralized.
Although in the literature, there is no study that evaluated the effect of torsional osteotomies performed on different levels on frontal plane alignment, two studies tried to evaluate the effect of shaft malrotation after a femoral fracture on frontal plane alignment.
The study of Gugenheim et al. [10] also used a three-dimensional computer model to simulate a malrotated fracture. It was demonstrated that internal and external rotation causes malalignment in the frontal plane, depending on the level of the fracture and the magnitude of malrotation. The radius of the curvature in the sagittal plane in their model was 2.2 m. When comparing their results with the results of the present study, similar effects on frontal plane alignment could be observed. On the supracondylar level, external rotation of the distal fragment, which is equivalent to a decreased anteversion angle, leads to an increased valgus angulation. They found a decreased mLDFA of 1.5° after 30° of external rotation. The correspondent simulation (antecurvatum angle of 12°) in the present study showed a decreased mLDFA of 2.1°.
Bretin et al. [1] measured intraarticular contact pressures after internal rotation and external rotation of the distal fragment of ten cadaveric legs. Internal rotation resulted in valgus deviation of the mechanical axis. External rotation caused varus deviation. The authors demonstrated that femoral malrotation has a significant effect on mechanical axis alignment and force vectors within the knee. However, the influence of the femoral antecurvatum angle on frontal plane alignment was not evaluated.
Different limitations of this study have to be considered. The computer model used was created from CT data of a human cadaver with no anatomical abnormalities. This model only provides mechanical scenarios, which should be considered when planning torsional osteotomies. It was beyond the scope of the study to provide exact data for the surgeon in each single case. A desirable algorithm for the surgeon would have to include a high number of combinations of possible values for femoral length, femoral anteversion, neck-shaft angle and femoral antecurvatum angle. Measuring the effects of all these combinations in cadavers or patients would be very difficult to achieve.
As a clinical consequence in cases with concomitant varus malalignment of the femur a distal osteotomy might be preferable when performing an external derotational osteotomy, in cases with concomitant valgus malalignment of the femur a proximal osteotomy might be preferable. Higher degrees of torsional correction and clinical suspicion of increased ACA have an increased risk of unintentional implications on frontal plane alignment.
In summary, this three-dimensional computer model study demonstrates the relationship between femoral torsional osteotomies and frontal plane alignment. The results of the present study confirm the results of studies that evaluated the effect of malrotation after femoral fractures.
Performing torsional osteotomies of the femur several issues have to be considered.
-
1.
Proximal external derotational osteotomies resulted in an increased varus angulation due to an increased mLDFA, and distal external derotational osteotomies resulted in an increased valgus angulation due to a decreased mLDFA.
-
2.
In patients with increased antecurvatum angles of the femur (increased sagittal bowing), the effects on frontal plane alignment are more pronounced.
-
3.
Mid-shaft torsional osteotomies had the smallest effect on frontal plane alignment.
-
4.
In patients with a pre-existing concomitant, frontal plane malalignment torsional osteotomies can induce a clinically relevant increase in malalignment.
Conclusion
Torsional osteotomies can induce a clinically relevant change of frontal plane femoral malalignment, especially in patients with an increased antecurvatum angle of the femur.
References
Bretin P, O’Loughlin PF, Suero EM, Kendoff D, Ostermeier S, Hüfner T, Krettek C, Citak M (2005) Influence of femoral malrotation on knee joint alignment and intra-articular contract pressures. Arch Orthop Trauma Surg 131:1115–1120
Bruce WD, Stevens PM (2004) Surgical correction of miserable malalignment syndrome. J Pediatr Orthop 24:392–396
Collado H, Fredericson M (2010) Patellofemoral pain syndrome. Clin Sports Med 29:379–398
Cooke TD, Price N, Fisher B, Hedden D (1990) The inwardly pointing knee. An unrecognized problem of external rotational malalignment. Clin Orthop Relat Res 260:56–60
Delgado ED, Schoenecker PL, Rich MM, Capelli AM (1996) Treatment of severe torsional malalignment syndrome. J Pediatr Orthop 16:484–488
Dickschas J, Harrer J, Pfefferkorn R, Strecker W (2012) Operative treatment of patellofemoral maltracking with torsional osteotomy. Arch Orthop Trauma Surg 132:289–298
Fabry G, MacEwen GD, Shands AR (1973) Torsion of the femur. A follow-up study in normal and abnormal conditions. J Bone Joint Surg Am 55:1726–1738
Gérard R, Stindel E, Moineau G, Le Nen D, Lefèvre C (2009) Rotational femoral osteotomies using an endomedullary saw. Orthop Traumatol Surg Res 95:414–419
Gordon JE, Pappademos PC, Schoenecker PL, Dobbs MB, Luhmann SJ (2005) Diaphyseal derotational osteotomy with intramedullary fixation for correction of excessive femoral anteversion in children. J Pediatr Orthop 25:548–553
Gugenheim JJ, Probe RA, Brinker MR (2004) The effects of femoral shaft malrotation on lower extremity anatomy. J Orthop Trauma 18:658–664
Harper MC, Carson WL (1987) Curvature of the femur and the proximal entry point for an intramedullary rod. Clin Orthop Relat Res 220:155–161
Huber H, Haefeli M, Dierauer S, Ramseier LE (2009) Treatment of reduced femoral antetorsion by subtrochanteric rotational osteotomy. Acta Orthop Belg 75:490–496
Insall J, Falvo KA, Wise DW (1976) Chondromalacia patellae. A prospective study. J Bone Joint Surg Am 58:1–8
Kitaoka HB, Weiner DS, Cook AJ, Hoyt WA, Askew MJ (1989) Relationship between femoral anteversion and osteoarthritis of the hip. J Pediatr Orthop 9:396–404
Kling TF Jr, Hensinger RN (1983) Angular and torsional deformities of the lower limbs in children. Clin Orthop Relat Res 176:136–147
Lee TQ, Anzel SH, Bennett KA, Pang D, Kim WC (1994) The influence of fixed rotational deformities of the femur on the patellofemoral contact pressures in human cadaver knees. Clin Orthop Relat Res 302:69–74
Lee TQ, Morris G, Csintalan RP (2003) The influence of tibial and femoral rotation on patellofemoral contact pressure. J Orthop Sports Phys Ther 33:686–693
Liu RW, Toogood P, Hart DE, Davy DT, Cooperman DR (2009) The effect of varus and valgus osteotomies on femoral version. J Pediatr Orthop 29:666–675
Paley D, Testworth K (1992) Mechanical axis deviation of the lower limbs. Preoperative planning of uniapical angular deformities of the tibia or femur. Clin Orthop Relat Res 280:48–64
Paley D (2001) Rotation and angulation–rotation deformities. In: Paley D (ed) Principles of deformity correction. Springer, Berlin, pp 235–236
Payne LZ, DeLuca PA (1994) Intertrochanteric versus supracondylar osteotomy for severe femoral anteversion. J Pediatr Orthop 14:39–44
Sankar WN, Neubuerger CO, Moseley CF (2009) Femoral anteversion in developmental dysplasia of the hip. J Pediatr Orthop 29:885–888
Seo JG, Kim BK, Moon YW, Kim JH, Yoon BH, Ahn TK, Lee DH (2009) Bony landmarks of determining the mechanical axis of the femur in the sagittal plane during total knee arthroplasty. Clin Orthop Surg 1:128–131
Souza RB, Draper CE, Fredericson M, Powers CM (2010) Femur rotation and patellofemoral joint kinematics: a weight-bearing magnetic resonance imaging analysis. J Orthop Sports Phys Ther 40:277–285
Staheli LT, Corbett M, Wyss C, King H (1985) Lower-extremity rotational problems in children. J Bone Joint Surg Am 67:39–47
Stevens PM, Anderson D (2008) Correction of anteversion in skeletally immature patients: percutaneous osteotomy and transtrochanteric intramedullary rod. J Pediatr Orthop 28:277–283
Tang WM, Chiu KY, Kwan MF, Ng TP, Yau WP (2005) Sagittal bowing of the distal femur in Chinese patients who require total knee arthroplasty. J Orthop Res 23:41–45
Tönnis D, Heinecke A (1999) Acetabular and femoral anteversion: relationship with osteoarthritis of the hip. J Bone Joint Surg Am 81:1747–1770
Yehyawi TM, Callaghan JJ, Pedersen DR, O’Rourke MR, Liu SS (2007) Variances in sagittal femoral shaft bowing in patients undergoing TKA. Clin Orthop Relat Res 464:99–104
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nelitz, M., Wehner, T., Steiner, M. et al. The effects of femoral external derotational osteotomy on frontal plane alignment. Knee Surg Sports Traumatol Arthrosc 22, 2740–2746 (2014). https://doi.org/10.1007/s00167-013-2618-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-013-2618-5