
Abstract
Purpose
To describe the incidence and injury distribution of knee injuries in the general population of a European setting.
Methods
Retrospective study of all knee injuries registered at the Emergency Department at Umeå University Hospital, Sweden, during 1995–2009 in relation to age, sex, diagnosis, location and activity at the time of injury, mechanism of injury, and treatment and/or follow-up plan.
Results
During 1995–2009, 12,663 knee injuries were registered, 8 % of all injuries. The incidence of knee injuries resulting in a visit to the Emergency Department was six cases per 1,000 person years. One-third of all injuries occurred during sports. And 30 % were 15–24 years. More men than women were injured during sporting activities and women were mostly injured during transportation.
Conclusion
Knee injuries in a general population are common and the injury distribution varies with age and sex. Sports activities and young age were prominent features of the injured population.
Level of evidence
IV.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In 1991, Nielsen and Yde [8] noted the lack of description of the epidemiology of acute knee injuries in the literature. Their findings were that roughly 6 % of all injuries treated at an Emergency Department (ED) involved the knee joint, and the incidence was calculated to 12 injuries per 1,000 inhabitants per year [8]. The best attempt since then, in over 20 years, is the study of Gage et al. [3] published in 2012, including 6.6 million knee injuries where they found an incidence of 2.29 knee injuries per 1,000 persons per year. Most knee injuries are minor ones such as abrasions, contusions etc., and can be treated at the ED while other injuries are more severe; dislocations, fractures, ligament injuries, meniscal tears and cartilage damage and might need surgery.
Fractures have been shown to occur more frequently in early adolescence and old age [1, 5]. In other periods of life, injury is more likely to affect other tissues. In a long-term perspective, severe injuries like cartilage defects, but also meniscus tears and ligament injuries which lead to instability, may result in an increased risk of osteoarthritis besides impaired function, temporary or permanently [6, 10, 12, 13]. High injury rate is found among teenager and young adults; the impaired function will follow them throughout life with effects as social, emotional, psychological, physical, and economical [3]. Besides the personal suffering, there is also an impact on the society due to loss of work days and costs for health care [4]. With knowledge of incidence in a general population, there might be a better support for further studies and prevention work.
Umeå University Hospital (UUH), Sweden, has the only ED in the area, serving a population of approximately 140,000 inhabitants. All patients or next of kin are asked to fill in a questionnaire about the circumstances when seeking care at the ED, and this questionnaire serve as basis for the injury registration system (IRS). Previously, IRS has been used to identify risk factors and type of fractures in youth and elderly [1, 5]. The IRS also reports all traffic injuries to the Swedish Traffic Accident Data Acquisition (STRADA), and data are used in injury prevention work [9, 14, 15].
The aim of this study is to describe the incidence and injury distribution of knee injuries in a general population.
Materials and methods
UUH serves Umeå and its five neighboring municipalities with a total population of about 140,000. The average age of the population in the year of 2009 was 40 for women and 38 for men. During the study period, there was only one emergency and radiology unit within a radius of approximately 100 km; therefore, all injuries in the area requiring assessment by an orthopedic consult and/or radiographic investigation are registered.
The injury registration at UUH is part of a collaborative project within the European Union using the injury database (IDB) to which selected hospitals in Europe contribute data. The manner of registration at UUH is in accordance with registration at all other IDB centers. At UUH, the injury registration started in 1985; in 1993, all data collected were digitalized and fed into a database. For practical reason, data not digitalized were excluded from analyses. Also data from 1993 to 1994 were excluded from analyses as these years had fewer injuries recorded, compared to subsequent years of registration (maybe due to break-in period of the registration). The registration misses for in-patients are negligible, as a check against the hospitals compulsory E-number (External cause to inpatient treatment-ICD 10) made it possible to find missed cases. Since 1998, the registry of the ED’s reception desk was also cross-checked, to estimate the numbers of cases lost due to lack of registration among outpatients. The lack of registration of injuries among outpatients resulting in dropout for 1998–2009 was estimated to be 10 % or less, the loss has varied somewhat over the years, but it never exceeded 11 %.
Data from patient’s questionnaire, from ambulance personnel, police reports, and medical record including attending physician’s diagnosis, have been included in the data set. All data collected were fed into the IRS by personnel at the Emergency and Disaster Medical Center at UUH. The staff responsible for the registration into the database uses a specific manual in order to secure consistency in the definition of variable values, and the staff is continuously educated how to register and code different injuries. Variables include injured body part, type of injury, age, sex, location and activity during injury, mechanism of injury, and type of treatment/follow-up. All injury events located to “the knee” were included in the analysis. In the case of multiple injuries to the knee, e.g., a simultaneous laceration and fracture, this was considered as one injury event in the analysis, except in the analysis of diagnosis where all diagnoses are reported. In this material, the diagnoses are divided into sprain/strain, dislocation, contusions, open wounds or abrasions, fractures, and others (frostbites, burns and inflammatory response due to overuse etc.).
Statistical analysis
Rates are presented as age- and sex-adjusted incidence density per person years, using Swedish national figures for the year 2000 as the standard population, or as age- and/or sex-specific incidence density. For all incidence density rates 95 % CI are given. For comparison of subgroups, rate ratios, i.e., risk ratio, are presented, with 95 % CIs.
This project was approved by the Regional Ethical Review Board in Umeå (2011-06-16, nr 2011-162-31M).
Results
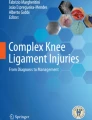
During 1995–2009, 162,467 injuries were registered in the IRS at UUH. Of all injuries in the IRS, between 536 and 1,010 each year, were registered as a knee injury, all together 12,663 injuries (8 %) (Fig. 1). These knee injuries occurred in 6,041 (48 %) women and 6,622 (52 %) men. The incidence of knee injuries resulting in a visit to the hospital ED was six cases per 1,000 inhabitants per years (Table 1).

Incidence of knee injuries per year 1995–2009. Bar graph showing incidence (cases per 1,000 inhabitants per year) for a visit to the Emergency Department at Umeå University Hospital involving a knee injury among the general population of Umeå and its five neighboring municipalities during 1995–2009
Mechanism of injury
The most common mechanism of injury in women and men was different types of falls, women 2,962 (23 %), and men 2,374 (19 %) (Table 2). Half of all women (50 %) sustaining a knee injury from falls were 50 years of age or older, for men only 28 % were 50 years of age or older.
Diagnosis
In total, 5,483 injuries are classified as sprains/strains (women 19 %, men 34 %); 596 as dislocation (women 3 %, men 2 %); 3,441 as contusions (women 14 %, men 12 %), 1,841 as open wounds or abrasions (women 6 %, men 8 %), 832 as fractures (women 3 %, men 3 %) (Table 3). The other 770 injuries included frostbites, burns, and inflammatory response due to overuse (Fig. 2). 81 women and 129 men were missing a specific diagnosis.

Incidence of knee injuries related to diagnosis. Line graphs showing sex- and age-specific rate of knee injuries categorized in different diagnoses seen at the Emergency Department at Umeå University Hospital among the general population in Umeå and its five neighboring municipalities. The mean age for men to suffer a knee sprain/strain was 30 (median 26) and for women 31 (median 24)
Age
The age group between 15 and 24 years accounted for a large proportion of all injuries, 1,731 women (14 %) and 2,004 men (16 %) (Fig. 2).
Activity
In women, the most common activity was transportation (walking, driving car or bicycle etc.); 2,174 injuries (17 %) (Fig. 3). In men, 1,741 injuries (14 %) occurred during transportation (Fig. 3; Table 4). In the transportation-related injuries, among women 1,155 (9 %) were pedestrians and in men 649 (5 %) (Table 5). In men, the most common activity was sports, 2,498 cases (20 %). In women, sports injuries accounted for 1,703 cases (13 %) (Table 6). Persons aged 15–24 years accounted for 1,902 cases (45 %) of all sports-related knee injuries.

Activity at time of injury. Histogram showing the distribution of activities taking place at the time of knee injury, resulting in a visit to the Emergency Department at Umeå University Hospital
The most common sporting activity leading to a knee injury was soccer [869 men (7 %), 528 women (4 %)]. 147 (1 %) cases had missing values in activity taking place at time when injury occurred.
Most patients were injured during their spare time, 4,838 (38 %) women and 5,314 (42 %) men.
Location
The single most common injury location for both women and men was sports hall/gymnasium, 645 women (5 %) and 874 men (7 %). Other common injury locations were sports facility outdoors; 406 women (3 %), 694 men (5 %); public street in urbanized area; 549 women (4 %), 439 men (3 %); ski resort; 330 women (3 %), 346 men (3 %).
Treatment
The distribution of various treatments and/or follow-up plans among patients registered with knee injuries was as follows: examined without treatment 2,347; 1,173 (9 %) women and 1,174 (9 %) men; treated with/without revisiting the same clinic 7,536; 3,518 (28 %) women and 4,018 (32 %) men; referred to other clinics 1,549; 686 (5 %) women and 863 (7 %) men; treated and admitted to hospital 1,201; 652 (5 %) women and 549 (4 %) men; other or unspecific treatment; 30 (12 women and 18 men) (Fig. 4).

Distribution of knee injuries related to treatments (include: patches, cast, bandage, crutches, sewing etc.). Bar graph showing distribution of treatment/follow-up plan (n) of acute knee injuries registered at Umeå University Hospital during 1995–2009
Discussion
The most important finding of the present study was that the incidence of knee injury in a general population, resulting in a visit at the ED at UUH, was as high as six cases per 1,000 inhabitants per years. The knee injury distribution varies with age; the age group between 15 and 24 years accounts for one-third of all injuries and the injury is most likely a sprain or strain. Our findings will hopefully encourage planning for medical resources to identify complex injuries in this young population, injuries that may lead to impaired function in long term perspectives, as fast as possible.
The analysis of IRS data showed that knee injuries causing visits at the ED are common; there are approximately as many knee injuries registered at UHH as there are wrist and ankle injuries. The true incidence of knee injuries is higher since some are not seen at the ED. Nielsen and Yde [8] reported a rate of knee injuries at two ED’s in Århus, Denmark, of 12 cases per 1,000 inhabitants per year. There are differences in the setup of the present study and Nielsen and Yde’s study; their study was during one single year, and in the present study, all knee injuries seen at the ED during 15 years were included. The difference in rates of knee injuries could also due to differences in people’s tendency to seek medical care at an ED. The total rate of visits due to injury was higher in the Århus study, 189 cases per 1,000 inhabitants per year compared to the rate of 78 cases per 1,000 inhabitants per year in the present study. The lower incidence in the present study might also reflect more severe injuries. The incidence in our study differs also from a study of 6.6 million knee injuries resulting in a visit to ED from 1999 through 2008 [3]. Gage et al. found a rate of 2.29 cases per 1,000 inhabitants per year while our incidence is 6. The higher incidence in our study may reflect that UUH has the only ED with a radiology department in a radius of 100 km, and Sweden has a social secure system that includes a health insurance for all inhabitants.
As expected, the results show that fractures around the knee were more common among elderly and young age as is the case with fractures in general [1, 5]. In the older population, fractures are more common, in incidence when it comes to women (12–17/10,000), but also in proportion (13–29 %) for both sexes. Clinical relevance of this finding is that there should be a high suspicion of fracture when evaluating the senior patient (65+) with a knee injury. Sprains and strains were the most common type of knee injury in both women and men especially in ages 15–24 years. Women and men aged 15–24 account for a large proportion of the sports-related knee injuries, almost half of these injuries. The fact that sport is related to a large proportion of acute knee injuries is consistent with previous studies [3, 7, 8, 16]. The sex-related differences in rates of sporting injuries may reflect changes in activity and sports participation with age. It could be that women become less active in sports as they enter late adolescence. But it could also be that men, through their behavior and choice of sporting activities, are more prone to knee injury from late adolescence to middle age. The only activity women are more frequently represented is transportation and especially as pedestrians. Perhaps women walk to a greater extent, instead of using a vehicle for transportation, and are thereby more exposed to falls? Umeå is located in the northern part of Sweden with an average temperature below zero, 5 months per year (November–March) with slippery roads and sidewalks. This could increase the risk of pedestrian injuries and be reflected in the rate of injuries among those groups who are most active in walking. Transportation, as an activity code, is not mentioned in the study of Gage et al. [3] and is probably in the group of “other” activity (6.9 %). Is this a result of prevention work? Or is “walking” only a recreational activity in the United States and seldom used for transportation? In a previous study of falls among people aged 50 and older by Painter et al. [11], it was presented that walking was the most frequent cause of falling among both women and men; women demonstrated a higher percentage of falls compared to men regardless of age group.
Only 69 % of all knee injuries needed treatment at the ED. The main reason to seek health care at an ED is probably to exclude fracture by radiograph and to get an examination and diagnosis, not to get treatment in the first instance unless, of course, there is a fracture, dislocation or open wound that needs treatment.
The strength of the present study is the well-defined community of approximately 140,000 inhabitants, with unselected material. The average age of the population in this study is slightly lower than the average age in Sweden; this is probably because Umeå holds a university with more than 12,000 students living in Umeå. A further strength of this study is that the questionnaire used in the IRS has been well adopted by the staff at the hospital, and the questionnaire is an advantage in itself compared to information from a diagnostic register; it gives a more complex picture of the injury because it includes not only medical details but also information about circumstances surrounding the injury. The missing cases in IRS are few, less than 11 % (1998–2009). Funding from the Social Board and the County Council has enabled an organization whose only task it is to optimize the data in the IRS.
A limitation of the present study is the imprecise method of classifying the injuries. We found it difficult to distinguish sprain from strain why we have chosen a combined diagnosis, as used earlier by Gage et al. [3]. The diagnosis of dislocation occurs mostly among young girls and probably consists of luxations of patellae, since “true” knee luxation is very rare.
An avulsion fracture may be registered as a fracture though it is a ligament injury and on the other hand; a dislocation of the knee joint is classified with the same code as a simple sprain. In the study of Nielsen and Yde, knee injuries seen at two ED’s in Denmark during 1 year were investigated; they followed their patients with knee injuries for at least 18 months and they described that many of their patients had a change of diagnosis during the period of investigation [8]. In this study, we have analyzed knee injuries, not patients; we do not know if some patients repeatedly sought medical care for the same kind of injury. For example, an injury of the anterior cruciate ligament might lead to instability of the knee joint and those patients could have multiple give-away episodes [2].
Results from the present study show a relatively high incidence of strain and sprains in young people where sport activity was most common among men. Early diagnosis of complex knee injuries is probably crucial for best outcome in the long run why there should be a specified follow-up plan for this group with access to MRI and surgery. Medical resources can also be better planned due to proportion of children and elderly in the population; they are most likely to incurring a fracture that might need treatment by surgery and in hospital care. Our results can also inspire to prevention work; why do female pedestrians have a relatively high rate of knee injuries?
The incidence of knee injuries in a general population, as described, is relatively high and the injury distribution varies with age and sex. Sports activities and young age were prominent features of the injured population. The presented epidemiology of knee injuries gives a perspective and a basis for every forthcoming study involving knee injuries. Analyzing material from a database is a blunt method and it is not possible to distinguish a severe knee injury from a minor one. In the present study, we have analyzed knee injuries seen at an ED, which probably reflects at least the incidence of more severe injuries.
Conclusion
Knee injuries in a general population are common, and the injury distribution varies with age and sex. Sports activities and young age were prominent features of the injured population.
References
Bergstrom U, Bjornstig U, Stenlund H, Jonsson H, Svensson O (2008) Fracture mechanisms and fracture pattern in men and women aged 50 years and older: a study of a 12-year population-based injury register, Umea, Sweden. Osteoporos Int 19(9):1267–1273
Courtney C, Rine RM, Kroll P (2005) Central somatosensory changes and altered muscle synergies in subjects with anterior cruciate ligament deficiency. Gait Posture 22(1):69–74
Gage BE, McIlvain NM, Collins CL, Fields SK, Comstock RD (2012) Epidemiology of 6.6 million knee injuries presenting to United States Emergency Departments from 1999 through 2008. Acad Emerg Med 19(4):378–385
Gianotti SM, Marshall SW, Hume PA, Bunt L (2009) Incidence of anterior cruciate ligament injury and other knee ligament injuries: a national population-based study. J Sci Med Sport 12(6):622–627
Hedstrom EM, Svensson O, Bergstrom U, Michno P (2010) Epidemiology of fractures in children and adolescents. Acta Orthop 81(1):148–153
Ichiba A, Kishimoto I (2009) Effects of articular cartilage and meniscus injuries at the time of surgery on osteoarthritic changes after anterior cruciate ligament reconstruction in patients under 40 years old. Arch Orthop Trauma Surg 129(3):409–415
Kannus P, Jarvinen M (1989) Incidence of knee injuries and the need for further care—a one-year prospective follow-up-study. J Sport Med Phys Fitness 29(4):321–325
Nielsen AB, Yde J (1991) Epidemiology of acute knee injuries: a prospective hospital investigation. J Trauma 31(12):1644–1648
Nyberg A, Gregersen NP (2007) Practicing for and performance on drivers license tests in relation to gender differences in crash involvement among novice drivers. J Safety Res 38(1):71–80
Oiestad BE, Holm I, Aune AK, Gunderson R, Myklebust G, Engebretsen L, Fosdahl MA, Risberg MA (2010) Knee function and prevalence of knee osteoarthritis after anterior cruciate ligament reconstruction: a prospective study with 10 to 15 years of follow-up. Am J Sports Med 38(11):2201–2210
Painter JA, Elliott SJ, Hudson S (2009) Falls in community-dwelling adults aged 50 years and older: prevalence and contributing factors. J Allied Health 38(4):201–207
Potter HG, Jain SK, Ma Y, Black BR, Fung S, Lyman S (2012) Cartilage injury after acute, isolated anterior cruciate ligament tear: immediate and longitudinal effect with clinical/MRI follow-up. Am J Sports Med Am J Sports Med 40(2):276–285
Roos EM, Roos HP, Ekdahl C, Lohmander LS (1998) Knee injury and Osteoarthritis Outcome Score (KOOS)—validation of a Swedish version. Scand J Med Sci Sports 8(6):439–448
Sakshaug L, Laureshyn A, Svensson A, Hyden C (2010) Cyclists in roundabouts—different design solutions. Accid Anal Prev 42(4):1338–1351
Strandroth J, Rizzi M, Sternlund S, Lie A, Tingvall C (2011) The correlation between pedestrian injury severity in real-life crashes and Euro NCAP pedestrian test results. Traffic Inj Prev 12(6):604–613
Yawn BP, Amadio P, Harmsen WS, Hill J, Ilstrup D, Gabriel S (2000) Isolated acute knee injuries in the general population. J Trauma 48(4):716–723
Acknowledgments
The authors would like to thank the staff at the Emergency Department at UUH and the staff at Emergency and Disaster Medical Center, UUH, for their work in maintaining and the compilation of the database. We would especially like to thank Magnus Hellström and P-O Bylund for their advices and help with the database.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ferry, T., Bergström, U., Hedström, E.M. et al. Epidemiology of acute knee injuries seen at the Emergency Department at Umeå University Hospital, Sweden, during 15 years. Knee Surg Sports Traumatol Arthrosc 22, 1149–1155 (2014). https://doi.org/10.1007/s00167-013-2555-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-013-2555-3