
Abstract
Purpose
Recently, single-bundle (SB) anterior cruciate ligament (ACL) reconstruction has been advanced by the anatomic concept, but the biomechanical outcome of the anatomic method has not been fully investigated, especially for rotational instability. Anatomic SB and the single over-the-top procedures are the treatment of choice for primary cases and revision or skeletally immature cases, respectively. The purpose of this study was to investigate the dynamic rotational instability of anatomic SB and over-the-top reconstruction during a pivot shift test using triaxial accelerometry.
Methods
Eight fresh frozen human cadaveric knees were used in this study. Rotational instability measurement was conducted during a pivot shift test by the use of a triaxial accelerometer attached to the tibia. The tests were performed in the ACL-intact, ACL-deficient and ACL-reconstructed knees with two different procedures (anatomic SB and over-the-top). The acceleration in three directions and the magnitude of acceleration were measured to evaluate rotational instability and compare between four different knee states.
Results
The overall magnitude of acceleration was significantly different (P < 0.01) between the ACL-intact knees and the ACL-deficient knees. Both anatomic SB and over-the-top ACL reconstruction significantly reduced the overall magnitude of acceleration compared to the ACL-deficient knees, but still had larger accelerations compared to the ACL-intact knees. There was no significant difference for the overall magnitude of acceleration between anatomic SB and over-the-top reconstruction procedure.
Conclusion
Over-the-top reconstruction provides comparable result to anatomic SB reconstruction in terms of controlling the dynamic rotational stability. Over-the-top reconstruction might be one of the options for revision cases and in skeletally immature patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Transtibial single-bundle (SB) anterior cruciate ligament (ACL) reconstruction has been widely advocated until recent investigations revealed that with this technique, it is difficult to achieve anatomic graft placement [1, 4, 16, 24]. Non-anatomic reconstructions have been shown to result in abnormal knee kinematics and further progress to osteoarthritis over time [14, 27, 31, 39, 44]. Anatomic placement using a far anteromedial or accessory medial portal, that is, transportal technique, has been advocated for both SB and double-bundle (DB) reconstruction in order to achieve anatomic graft placement and improved knee rotational stability [6].
Rotational stability after DB ACL reconstruction has been extensively researched [37, 38, 46, 48, 50], but there is lack of rotational studies of the anatomic SB ACL reconstruction in spite of its increasing popularity [23]. Over-the-top (OTT) ACL reconstruction, in which the graft is passed over the superomedial border of lateral femoral condyle and fixed on the lateral femoral shaft over the condyle, is often used as salvage option for revision cases and in skeletally immature patients [3, 30, 45, 47]. OTT ACL reconstruction also has not been fully examined for rotational stability. Since this procedure is fundamentally non-anatomic, the resultant knee kinematics are assumed to be inferior to the anatomic ACL reconstruction. However, it is still unknown how much these two clinically prevalent techniques effect to the knee stability, especially rotational stability.
The rotational instability of the knee is clinically assessed by the pivot shift test which is basically a subjective evaluation [13, 25, 33], while its quantitative evaluation is yet to be established. However, recent research efforts and advanced technology have facilitated the investigation of quantitative assessment of the pivot shift by measuring dynamic parameters, such as velocity or acceleration, during the manually performed pivot shift test [2, 7–9, 17, 26, 32]. The increased acceleration during the pivot shift test in the ACL-deficient knees by the use of triaxial accelerometry, which can be used as an experimental method for exploring the resultant knee rotational stability after certain types of ACL reconstructions, was reported in previous study [36].
Therefore, the purpose of this study was to investigate the dynamic rotational instability of anatomic SB and the OTT ACL reconstructions during a pivot shift test using triaxial accelerometry. It was hypothesized that the anatomic SB reconstruction would provide better dynamic rotational stability than the OTT procedure.
Materials and methods
Eight fresh frozen human cadaveric knees were used in this study. Each specimen was screened for any bony and ligamentous abnormalities by manual examination, CT scan and arthroscopy. All specimens were stored at −20 °C and thawed at room temperature 24 h before testing. The femur and the tibia were cut approximately 20 cm from the joint line. All soft tissue was removed from the cut ends of femoral and tibial shafts in 10 cm while keeping the knee joint intact. Both exposed femoral and tibial shafts were secured in the cylindrical-shaped epoxy compound (Bondo, Atlanta, Georgia, USA) for mounting in custom-made aluminium clamps.
Rotational instability measurement
Rotational instability measurement using a triaxial accelerometer was conducted during a manually performed pivot shift test, repeatedly in the ACL-intact, ACL-deficient and ACL-reconstructed knees with two different procedures (anatomic SB and OTT). A single examiner performed the pivot shift test in all knees in order to exclude inter-examiner variation. The pivot shift test was performed according to the report of Hughston et al. [18], which reproduces the dislocation phase of the pivot shift phenomenon from flexion to extension [18].
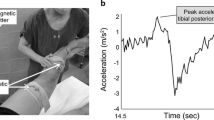
The three-dimensional acceleration (x-axis: anteroposterior; y-axis: mediolateral; z-axis: superoinferior) was measured with a triaxial accelerometer (Kistler, Winterhur, Switzerland) during the pivot shift test. The sensor was rigidly attached to the tibial tubercle with a bone screw (Fig. 1). Signals from the sensor were digitally recorded at a sampling rate of 10 kHz, while the waveforms expressing the acceleration were displayed on a computer screen (Fig. 2). The acceleration in each direction was then analysed and the overall magnitude of acceleration was calculated with use of the following formula: {|a| = √(ax 2 + ay 2 + az 2)}.

Human cadaveric knee mounted in custom fixture. The triaxial accelerometer was attached to the tibial tubercle with a screw

A typical example of waveforms in ACL-deficient condition during pivot shift test. Impulses are provoked at the time of pivot shift
Measurements were repeated at least three times in each knee state. The median value of three trials was used for comparison, while the other two results were used to assess the repeatability of the measurements. The overall magnitude of acceleration and each directional acceleration were compared between four different ACL states.
The reliability, repeatability and accuracy of this measurement were previously reported in the studies of dynamic instability [11, 34–36]. In the previous studies, the triaxial accelerometer showed a high repeatability of the measurements with a correlation coefficient over 0.95. The accuracy of the measurement for acceleration is given by the sensitivity of the accelerometer device, which is 1,000 mV/g.
Surgical technique
Both ACL reconstructions were performed arthroscopically using a three-portal technique comprising anterolateral, central and accessory anteromedial portals [10, 43].
For the anatomic SB ACL reconstruction, a guide pin was passed at the centre of the femoral insertion site of the ACL through the accessory anteromedial portal. The femoral tunnel was drilled with 8-mm-diameter acorn reamer. Subsequently, the 8-mm-diameter tibial tunnel was drilled at the centre of the tibial insertion site of the ACL. An 8-mm-diameter hamstring graft was passed through both femoral and tibial tunnels and fixed with EndoButton CL (Smith & Nephew, Andover, Massachusetts, USA) on the femoral side. The graft was preconditioned by cyclic flexion–extension loading for 10 cycles while applying a 44 N of graft tension. Tibial fixation was then performed at 30° of knee flexion using a staple with an initial tension of 44 N and augmented by suture to screw post-fixation.
For the OTT ACL reconstruction [47], a lateral incision was made at the distal femur to identify the OTT position, that is, posterolateral aspect of the distal femoral metaphysis, by palpation. A small hole was made in the posterior capsule from inside out by a curved clamp into the OTT position. The same size of hamstring graft was passed through the same location of the tibial tunnel as the anatomic SB procedure and fixed onto the OTT position with CL device (Smith & Nephew, Andover, Massachusetts, USA) and a post-screw at the lateral femoral metaphysis. The graft was preconditioned and fixed to the proximal tibia in the same fashion as the anatomic SB technique (Fig. 3).

Arthroscopic view of left knee after anatomic SB a and OTT b reconstruction. ACL anterior cruciate ligament, PCL posterior cruciate ligament, LFC lateral femoral condyle, MFC medial femoral condyle, OTT over-the-top
Statistical analysis
Statistical analysis for differences in the median acceleration during the pivot shift test among the four different ACL states was performed using the Kruskal–Wallis test, and differences between two groups were then tested by a post hoc Mann–Whitney U test. Statistical significance was assumed when P < 0.05 for Kruskal–Wallis test and P < 0.01 for Mann–Whitney U test. All statistical results were calculated using a statistical software package (SPSS ver. 17.0).
Results
A post hoc power analysis showed that a sample size of 8 specimens for each group would yield statistical power of 0.81.
The overall magnitude of acceleration was significantly different between the ACL-intact knees and the ACL-deficient knees (P < 0.01, Table 1). Both the anatomic SB and OTT ACL reconstructions significantly reduced the overall magnitude of acceleration compared to the ACL-deficient knees (P < 0.01), but still had larger accelerations compared to the ACL-intact knees (P < 0.01). There was no significant difference between anatomic SB and OTT reconstruction procedure (Fig. 4).

Overall magnitude acceleration in 4 different knee conditions. *P value < 0.01
The acceleration in the x direction, or anterior direction of the tibial tubercle, was not significantly different between four different ACL states. The acceleration along the y-axis, lateral direction of the tibial tubercle, was significantly different between the ACL-intact knees and the ACL-deficient knees (P < 0.01). Both the anatomic SB and OTT ACL reconstruction significantly reduced the acceleration in y direction compared to the ACL-deficient knees (P < 0.01), but still had larger accelerations compared to the ACL-intact knees (P < 0.01). There was no significant difference in the acceleration in the y direction between anatomic SB and OTT reconstruction procedure. For the acceleration in z direction, proximodistal direction of the tibial tubercle, there was a significant difference between the ACL-intact knees and the ACL-deficient knees (P < 0.01); however, neither the anatomic SB nor OTT ACL reconstructions significantly reduced the acceleration from the ACL-deficient status (P = 0.09 and 0.06, respectively) and had larger accelerations compared to the ACL-intact knees (P < 0.01). There was no significant difference for the acceleration in z-axis between anatomic SB and OTT reconstruction procedures.
Discussion
The most important findings of this study are that anatomic SB and OTT ACL reconstruction significantly reduced the overall magnitude of acceleration compared to the ACL-deficient knees, but still had larger accelerations compared to the ACL-intact knees. Contrary to the hypothesis, SB and OTT ACL reconstruction were not significantly different in controlling the rotational stability. In addition, the largest difference was in the lateral component of acceleration of the tibial tubercle, which could represent rotation of the tibia.
The effect of tunnel placement on knee rotational laxity using SB ACL reconstruction has been reported with a favourable result in lower femoral placement, although it remains unknown if the tunnel location is truly anatomic. Scopp et al. [41] found that rotational laxity of cadaveric knees was restored to normal with an oblique femoral tunnel placement [41]. Loh et al. [31] reported that grafts in the 10-o’clock position were able to resist rotator loads more effectively than grafts in the 11-o’clock position [31]. Thus, low graft placement has been recommended for SB ACL reconstruction with the expectations of better rotational laxity, but the tunnel location suggested by the clock-face reference cannot be consistent and reliable for three-dimensional structure of the intercondylar notch [12]. Meanwhile, this study is different in that the femoral and tibial tunnel placements were directly confirmed at the centre of the femoral and tibial original footprint using the transportal technique, and the dynamic rotational instability was assessed instead of the rotational laxity.
Although the OTT is a non-anatomic procedure, it is still used as a salvage option for limited cases to avoid drilling in the lateral condyle, such as a revision cases with a significant bone loss or a skeletally immature individual with an open physis [15, 21, 42, 45]. However, little is known about the resultant knee kinematics or rotational stability after the OTT ACL reconstruction. Clinical reports demonstrated that there was no significant difference in hamstring reconstructions by either OTT or via a femoral tunnel [19, 20]. Radford et al. [40] compared the static laxity at 20° and 90° knee flexion with the biomechanics of single-bundle OTT and femoral tunnel techniques and showed that the OTT reconstruction gave better anteroposterior stability and functioned like an intact ACL at 20° of knee flexion [40]. A recent study by Lertwanich et al. [29] reported that both anatomic SB and OTT techniques closely restored the intact knee kinematics, and there was no difference between anatomic SB and OTT technique in the kinematics with an anterior tibial load and a combined rotatory load [29]. Rotational instability is clinically evaluated by pivot shift test [13, 33], which depends on the examiner’s technique for the pivot shift movement during dynamic testing procedure. The presence of a positive pivot shift test is predictive of osteoarthritis of the knee, failure to return to previous level of play, patient reported instability and poor subjective outcome scores following ACL reconstruction [5, 22, 28, 49]. Bignozzi et al. [7] concluded that the dynamic evaluation of a pivot shift is better able to describe dynamic rotational instability [7]. Hoshino et al. [17] measured the tibial anterior translation and calculated the acceleration of the tibial posterior reduction using an electromagnetic device [17], and Lane et al. [26] measured similar acceleration of the tibial movement using a computer navigation system [26]. They both demonstrated increased acceleration of the ACL-deficient knees [17, 26], similarly to this study. Furthermore, this study evaluated acceleration after different ACL-reconstructed procedures, anatomic SB and OTT procedure, and found that both procedures could successfully reduce the dynamic instability of ACL deficiency, but failed to restore the intact level.
There are some limitations in this study. First, the knees were evaluated immediately after surgery, and consequently, the results represent time-zero conditions. The healing of the graft at the OTT position may be different from that of the femoral tunnel technique which utilizes circumferential tendon-to-bone contact. After time to develop adequate graft corporation into the bone, anatomic SB ACL could have different biomechanical properties than the replaced ACL on the OTT position. Second, manual tests like the pivot shift have a wide variability among examiners. In order to exclude such variability, the manual tests were performed by a single experienced examiner and the repeatability was re-evaluated in this study. The repeatability, that is, 331 ± 218 mm/s2 as a standard deviation, was consistent with our previous reports and other studies [17]. Last, since the acceleration was measured on the tibial tubercle, the direction of the acceleration change could not be directly described on the basis of 6°-of-freedom knee coordinate system which is commonly used for defining knee motion. Interestingly, our result indicated increase in the acceleration in the medial movement of the tibial tubercle, which appears to represent tibial rotation, while most of the previous report using 6°-of-freedom coordinate system demonstrated the increase in the acceleration in the tibial anteroposterior direction [17, 26]. Although the evaluated phase of the pivot shift test was also different, that is, the dislocation phase in this study and the reduction phase in the previous studies [17, 26], further investigation is warranted to examine how our measured acceleration can be explained by the common 6°-of-freedom knee kinematics.
Anatomic ACL reconstruction has been increasing its popularity. For revision cases and in skeletally immature patients, OTT ACL reconstruction is often used as salvage option. This study showed that both reconstructions had no significant differences in dynamic stability. OTT reconstruction might be one of the options for revision cases and in skeletally immature patients.
Conclusion
Although OTT reconstruction is used for limited cases, it provides comparable result to anatomic SB reconstruction in terms of controlling the dynamic rotational instability.
References
Abebe ES, Moorman CT III, Dziedzic TS, Spritzer CE, Cothran RL, Taylor DC, Garrett WE Jr, DeFrate LE (2009) Femoral tunnel placement during anterior cruciate ligament reconstruction. An in vivo imaging analysis comparing transtibial and 2- incision tibial tunnel-independent techniques. Am J Sports Med 37:1904–1911
Ahldén M, Hoshino Y, Samuelsson K, Araujo P, Musahl V, Karlsson J (2012) Dynamic knee laxity measurement devices. Knee Surg Sports Traumatol Arthrosc 20:621–632
Andrews M, Noyes FR, Barber-Westin SD (1994) Anterior cruciate ligament allograft reconstruction in the skeletally immature athlete. Am J Sports Med 22:48–54
Arnold MP, Kooloos J, van Kampen A (2001) Single-incision technique misses the anatomical femoral anterior cruciate ligament insertion: a cadaver study. Knee Surg Sports Traumatol Arthrosc 9:194–199
Ayeni OR, Chahal M, Tran MN, Sprague S (2012) Pivot shift as an outcome measure for ACL reconstruction: a systematic review. Knee Surg Sports Traumatol Arthrosc 20:767–777
Bedi A, Musahl V, Steuber V, Kendoff D, Choi D, Allen AA, Pearle AD, Altchek DW (2011) Transtibial versus anteromedial portal reaming in anterior cruciate ligament reconstruction: an anatomic and biomechanical evaluation of surgical technique. Arthroscopy 27:380–390
Bignozzi S, Zaffagnini S, Lopomo N, Fu FH, Irrgang JJ, Marcacci M (2010) Clinical relevance of static and dynamic tests after anatomical double-bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 18:37–42
Bull AMJ, Andersen HN, Basso O, Targett J, Amis AA (1999) Incidence and mechanism of the pivot shift. An in vitro study. Clin Orthop Relat Res 363:219–231
Bull AMJ, Earnshaw PH, Smith A, Katchburian V, Hassan ANA, Amis AA (2002) Intraoperative measurement of knee kinematics in reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br 84:1075–1081
Cohen SB, Fu FH (2007) Three-portal technique for anterior cruciate ligament reconstruction: use of a central medial portal. Arthroscopy 23:325
Debandi A, Maeyama A, Hoshino Y, Asai S, Goto B, Smolinski P, Fu FH (2013) The effect of tunnel placement on rotational stability after ACL reconstruction: evaluation with use of triaxial acceletometry in a porcine model. Knee Surg Sports Traumatol Arthrosc 21:589–595
Fu FH (2008) The clock-face reference: simple but nonanatomic. Arthroscopy 24:1433
Galway BA, MacIntosh DL (1980) The lateral pivot shift: a symptom and sign of anterior cruciate ligament insufficiency. Clin Orthop Relat Res 147:45–50
Georgoulis AD, Ristanis S, Chouliaras V, Moraiti C, Stergiou N (2007) Tibial rotation is not restored after ACL reconstruction with hamstring graft. Clin Orthop Relat Res 454:89–94
Harner CD (2004) Double bundle or double trouble? Arthroscopy 20:1013–1014
Heming JF, Rand J, Steiner E (2007) Anatomic limitation of transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med 35:1708–1715
Hoshino Y, Kuroda R, Nagamune K, Yagi M, Mizuno K, Yamaguchi M, Muratsu H, Yoshiya S, Kurosaka M (2007) In vivo measurement of the pivot-shift test in the anterior cruciate ligament-deficient knee using an electromagnetic device. Am J Sports Med 35:1098–1104
Hughston JC, Andrews JR, Cross MJ, Moschi A (1976) Classification of knee ligament instabilities. Part I. The medial compartment and cruciate ligaments. J Bone Joint Surg Am 58:159–172
Jonsson H, Elmqvist L, Karrhom J, Tegner Y (1994) Over-the-top or tunnel reconstruction of the anterior cruciate ligament? A prospective randomized study of 54 patients. J Bone Joint Surg Br 76:82–87
Karlson JA, Steiner ME, Brown CH, Johnston J (1994) Anterior cruciate ligament reconstruction using gracilis and semitendinosus tendon. Am J Sports Med 22:659–666
Kocher MS, Saxon HS, Hovis WD, Hawkins RJ (2002) Management and complications of anterior cruciate ligament injuries in skeletally immature patients: survey of the herodicus society and the ACL study group. J Pediatr Orthop 22:452–457
Kocher MS, Steadman JR, Briggs KK, Sterett WI, Hawkins RJ (2004) Relationships between objective assessment of ligament stability and subjective assessment of symptoms and function after anterior cruciate ligament reconstruction. Am J Sports Med 32:629–634
Kondo E, Merican AM, Yasuda K, Amis AA (2011) Biomechanical comparison of anatomic double-bundle, anatomic single-bundle, and nonanatomic single-bundle anterior cruciate ligament reconstructions. Am J Sports Med 39:279–288
Kopf S, Forsythe B, Wong AK, Tashman S, Anderst W, Irrgang JJ, Fu FH (2010) Nonanatomic tunnel position in traditional transtibial single-bundle anterior cruciate ligament reconstruction evaluated by three-dimensional computed tomography. J Bone Joint Surg Am 94:1427–1431
Kuroda R, Hoshino Y, Kubo S, Araki D, Oka S, Nagamune K, Kurosaka M (2012) Similarities and differences of diagnostic manual tests for anterior cruciate ligament insufficiency: a global survey and kinematics assessment. Am J Sports Med 40:91–99
Lane CG, Warren RF, Stanford FC, Kendoff D, Pearle AD (2008) In vivo analysis of the pivot shift phenomenon during computer navigated ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 16:487–492
Lee MC, Seong SC, Lee S, Chang CB, Park YK, Jo H, Kim CH (2007) Vertical femoral tunnel placement results in rotation knee laxity after anterior cruciate ligament reconstruction. Arthroscopy 23:771–778
Leitze Z, Losee RE, Jokl P, Johnson TR, Feagin JA (2005) Implications of the pivot shift in the ACL-deficient knee. Clin Orthop Relat Res 436:229–236
Lertwanich P, Kato Y, Martins CAQ, Maeyama A, Ingham SJM, Kramer S, Linde-Rosen M, Smolinski P, Fu FH (2011) A biomechanical comparison of 2 femoral fixation techniques for anterior cruciate ligament reconstruction in skeletally immature patients: over-the-top fixation versus transphyseal technique. Arthroscopy 27:672–680
Lo IKY, Kirkley A, Fowler PJ, Miniaci A (1997) The outcome of operative treated anterior cruciate ligament disruptions in the skeletally immature child. Arthroscopy 13:627–634
Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL-Y (2002) Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o’clock and 10 o’clock femoral tunnel placement. Arthroscopy 19:297–304
Lopomo N, Signorelli C, Bonanzinga T, Marcheggiani Muccioli GM, Visani A, Zaffagnini S (2012) Quantitative assessment of pivot-shift using inertial sensors. Knee Surg Sports Traumatol Arthrosc 20:713–717
Losee RE (1983) Concepts of the pivot shift. Clin Orthop Relat Res 172:45–51
Maeyama A, Naito M, Moriyama S, Yoshimura I (2008) Evaluation of dynamic instability of the dysplastic hip with use of triaxial accelerometry. J Bone Joint Surg Am 90:85–92
Maeyama A, Naito M, Moriyama S, Yoshimura I (2009) Periacetabular osteotomy reduces the dynamic instability of dysplastic hips. J Bone Joint Surg Br 91:1438–1442
Maeyama A, Hoshino Y, Debandi A, Kato Y, Saeki K, Asai S, Goto B, Smolinski P, Fu FH (2011) Evaluation of rotational instability in the anterior cruciate ligament deficient knee using triaxial accelerometer: a biomechanics model in porcine knees. Knee Surg Sports Traumatol Arthrosc 19:1233–1238
Markolf KL, Park S, Jackson SR, McAllister DR (2009) Anterior-posterior and rotator stability of single and double-bundle anterior cruciate ligament reconstructions. J Bone Joint Surg Am 91:107–118
Musahl V, Plaksey A, VanScyoc A, Sasaki T, Debski RE, McMahon PJ, Fu FH (2005) Varying femoral tunnels between the anatomic footprint and isometric position. Am J Sports Med 33:712–718
Øiestad BE, Holm I, Aune AK, Gunderson R, Myklebust G, Engebretsen L, Fosdahl MA, Risberg MA (2010) Knee function and prevalence of knee osteoarthritis after anterior cruciate ligament reconstruction: a prospective study with 10 to 15 years of follow-up. Am J Sports Med 38:2201–2210
Radford WJP, Amis AA (1990) Biomechanics of a double prosthetic ligament in the anterior cruciate deficient knee. J Bone Joint Surg Br 72:1038–1043
Scopp JM, Jasper LE, Belkoff SM, Moorman CT (2004) The effect of oblique femoral tunnel placement on rotational constrain of knee reconstructed using patellar tendon autograft. Arthroscopy 20:294–299
Siebold R (2007) Observation on bone tunnel enlargement after double-bundle anterior cruciate ligament reconstruction. Arthroscopy 23:291–298
Shino K, Horibe S, Hamada M, Nakamura N, Nakata K, Toritsuka Y, Mae T (2002) Allograft anterior cruciate ligament reconstruction. Tech Knee Surg 1:78–85
Tashman S, Collon D, Anderson K, Kolowich P, Anderst W (2004) Abnormal rotational knee motion during running after anterior cruciate ligament reconstruction. Am J Sports Med 32:975–983
van Eck CF, Schreiber VM, Liu TT, Fu FH (2010) The anatomic approach to primary, revision and augmentation anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 18:1154–1163
Yagi M, Wrong EK, Kanamori A, Debski RE, Fu FH, Woo SL-Y (2002) Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med 30:660–666
Yiannakopoulos CK, Fules PJ, Korres DS, Mowbray MAS (2005) Revision anterior cruciate ligament surgery using the over-the-top femoral route. Arthroscopy 21:243–247
Zaffagnini S, Marcheggiani Muccioli GM, Lopomo N, Signorelli C, Bonanzinga T, Musiani C, Vassilis P, Nitri M, Macacci M (2012) Can the pivot-shift be eliminate by anatomic double-bundle anterior cruciate ligament reconstruction? Knee Surg Sports Traumatol Arthrosc 20:743–751
Zampeli F, Pappas E, Giotis D, Hantes ME, Georgoulis AD (2012) Kinematic predictors of subjective outcome after anterior cruciate ligament reconstruction : an in vivo motion analysis study. Knee Surg Sports Traumatol Arthrosc 20:785–792
Zantop T, Diermann N, Schumacher T, Schanz S, Fu FH, Peterson W (2008) Anatomical and nonanatomical double-bundle anterior cruciate ligament reconstruction. Am J Sports Med 36:678–685
Acknowledgments
This study was supported by Albert B. Ferguson, Jr MD Orthopaedic Fund of The Pittsburgh Foundation.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Asai, S., Maeyama, A., Hoshino, Y. et al. A comparison of dynamic rotational knee instability between anatomic single-bundle and over-the-top anterior cruciate ligament reconstruction using triaxial accelerometry. Knee Surg Sports Traumatol Arthrosc 22, 972–978 (2014). https://doi.org/10.1007/s00167-013-2499-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-013-2499-7