
Abstract
Purpose
The aims of this study were to evaluate the functional recovery before and after ACL reconstruction and to evaluate the sensitivity to change in performance-based and self-reported outcomes prior to and after ACL reconstruction and to determine whether these changes represent clinically relevant improvement.
Methods
Eighty-three athletes participated in this study. Athletes were tested after an ACL injury, after preoperative training, and 6 and 12 months after ACL reconstruction. Athletes completed quadriceps strength testing, hop testing, and self-reported questionnaires for knee function (International Knee Documentation Committee subjective knee form, Knee Outcome Survey-Activities of Daily Living Scale, and the Global Rating Scale of Perceived Function) at each testing period.
Results
A significant interaction of limb by time was seen in normalized quadriceps strength, and single, triple, and 6-m timed hop, where the involved limb improved more than the uninvolved limb over time. A main effect of time was noted for performance-based limb symmetry indexes and self-reported measures.
Conclusion
Limb-to-limb asymmetries are reduced, and normal limb symmetry is restored after perturbation training and aggressive quadriceps strengthening and returned to similar levels 6 months after reconstruction. Performance-based values on the involved limb and self-reported outcomes are sensitive to change over time, and these were clinically relevant improvements.
Level of evidence
Prognostic study, Level II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The anterior cruciate ligament is the most frequently injured ligament in the knee, [33] with upward of 250,000 injuries annually in the United States [21]. The current standard of care advocated by the majority of orthopaedic surgeons for young, active individuals after ACL injury is early reconstruction [13, 36]. Athletes are frequently counseled to undergo ACL reconstruction with the expectation of normal knee function and a successful return to their previous levels of activity [6, 36]. Not all patients who have surgical reconstruction of the ACL return to previous levels of activity or exhibit normal knee function [3, 7, 13, 36]. Many individuals may continue to exhibit impaired functional performance with knee instability and pain, reduced range of motion, quadriceps strength deficits, reduced functional performance, neuromuscular dysfunction, and biomechanical maladaptations that may account for the highly variable outcomes [11, 12, 23, 30, 40].
Few prospective or longitudinal studies have evaluated the pattern of functional recovery prior to and after ACL reconstruction [12, 30, 47]. The restoration of limb symmetry appears to be a vital component in the functional recovery after ACL reconstruction [23, 38, 51]. Attainment of high limb symmetry may reduce asymmetrical ligament, soft tissue loading [38, 51], and risk of further injury [44, 51], and contribute to walking and jogging patterns similar to uninjured subjects [32]. Additionally, varying standards in limb symmetry indexes have previously been suggested as the milestone for determining normal limb symmetry [19, 23, 42].
The sensitivity to change in performance-based and self-reported outcomes may provide insight in detecting when a meaningful change has occurred over time and providing clinical guidance regarding functional recovery after ACL reconstruction. Patients with an ACL injury improve with treatment prior to and after ACL reconstruction [12, 23, 30, 37, 47]. Quadriceps strength and hop performance are sensitive to changes over time [48, 49], but clinically relevant change has not been reported. While studies have investigated the rate of change in quadriceps strength and hop performance prior to and after ACL reconstruction, little is known whether these changes represent clinically relevant improvements.
Therefore, the purpose of this study was to examine the pattern of functional recovery prior to and after ACL reconstruction up to 12 months after surgery. The aims of this study were (1) to identify at what time period the involved limb is symmetrical with the uninvolved limb in quadriceps strength and hop performance, (2) to analyze the changes in quadriceps strength, hop performance, and self-reported outcomes at different intervals, and (3) to determine whether these changes represent clinically relevant improvement. We hypothesized that involved limb performance would be symmetrical with the uninvolved limb performance in quadriceps strength and hop performance by 12 months after ACL reconstruction. In addition, we hypothesized that involved limb performance and self-reported measures would improve from baseline testing to 12 months after ACL reconstruction.
Materials and methods
One hundred and two subjects who sustained a unilateral ACL rupture were recruited for a prospective longitudinal observational study between 2005 and 2010. All subjects participated regularly (≥50 h/year) in Level I or II activities [11]. All subjects were between the ages of 15 and 53. Subjects were excluded for participation in this study if they had concomitant ligamentous injury, bilateral lower limb involvement, repairable meniscal damage, or full-thickness articular cartilage damage greater than 1 cm2. Complete ACL rupture was identified by greater than 3 mm side-to-side difference in anterior tibial translation [11] with maximum pull with a KT-2000 arthrometer (MedMetrics, San Diego, CA) and confirmed by magnetic resonance imaging. Maximum manual pull with KT arthrometer exhibits high sensitivity and specificity in discriminating normal knees from abnormal knees [4]. The study was approved by the University of Delaware Institutional Human Subjects Review Board (165436-1), and each subject gave informed consent. The flow diagram for subject participation for this study is illustrated in Fig. 1.

Flow diagram for subject involvement
Testing
All patients had an initial physical therapy evaluation to determine the level of physical impairments after ACL injury. Subjects who presented with knee effusion greater than trace effusion [53], limitations in knee range of motion, quadriceps side-to-side strength differences less than 70%, or who were unable to hop up and down on the involved limb without pain while wearing a functional knee brace underwent pre-baseline testing rehabilitation to address these physical impairments. Once these impairments were resolved, subjects were permitted to perform functional testing. Functional testing is a battery of tests that consists of quadriceps strength testing, single limb hop testing, and self-reported questionnaires. Subjects completed the functional testing at baseline (Baseline), after perturbation training (prior to surgery) (Post-perturbation), and 6 (6 M ACLR) and 12 months after ACL reconstruction (12 M ACLR).
Quadriceps strength
Quadriceps strength testing consisted of maximal voluntary isometric contraction (MVIC) of the quadriceps with burst superimposition technique [52]. This method was been shown to have high reliability with intraclass coefficients (ICC2,1) of 0.97–0.98 [9]. Patients performed an MVIC with a burst superimposition stimulation delivered to the quadriceps to determine patients’ ability to fully activate the quadriceps muscles. Verbal encouragement from the therapist and visual feedback from the dynamometer’s real-time visual display were used to help facilitate maximal effort. If the subject was unable to achieve 95% muscle activation during the burst superimposition technique, the test was repeated until 95% muscle activation was achieved or the subject became fatigued (up to 2 more MVICs). Quadriceps force was normalized to body mass index (N/BMI). Quadriceps strength index was calculated by dividing the involved quadriceps force by the uninvolved quadriceps force and expressing the result as a percentage.
Single limb hop testing
Single limb hop testing was conducted using the four hop tests described by Noyes et al. [42] while wearing a functional knee brace. The hop testing was administered in the following order: single, crossover, triple, and 6-m timed hop. These hop tests are valid and reliable [45, 50]. Reid et al. [45] showed ICC2,1 for limb symmetry limb indexes in patients after ACL reconstruction ranged from 0.82 to 0.92. Minimum detectable change (MDC) at 90% confidence level ranged from 7.05 to 12.96% [45]. Hop limb symmetry index (LSI) was expressed as a percentage of the averaged involved limb hop distances divided by the averaged uninvolved limb hop distances for each hop distance test or as a percentage of the averaged uninvolved limb hop times divided by the averaged involved limb hop times for 6-m timed hop.
Self-reported questionnaires
Patients completed three self-reported questionnaires: Knee Outcome Survey-Activities of Daily Living Scale (KOS-ADLS) [29], the International Knee Documentation Committee 2000 Subjective Knee Form (IKDC2000) [27, 28], and the Global Rating Scale of Perceived Function (GRS). The KOS-ADLS is a patient-reported measure of functional limitations and impairments of the knee during activities of daily living [29]. The test–retest ICC2,1 was 0.97, and the MDC at 95% confidence level was 8.87. The IKDC2000 is a joint-specific outcome measure for assessing symptoms, function, and sports activity pertinent to a variety of knee conditions [27]. The IKDC2000 has been demonstrated to contain items regarding symptoms and disabilities important to patients with an ACL tear [54]. The IKDC2000 is a valid and reliable self-reported outcome measure [24, 27]. Irrgang et al. [28] demonstrated the responsiveness of the IKDC2000 and a score of 11.5 are necessary to distinguish between those who have improved and those who have not improved. The GRS is a question that asks patients to rate their current knee function on a scale from 0 to 100, with 0 being the inability to perform any activity and 100 being your level of knee function prior to your injury, including sports. Hopper et al. [25] reported the test–retest ICC3,1 for the analogue GRS was 0.96, which corresponds to an MDC at 95% confidence level of 6.49.
Preoperative rehabilitation
Subjects participated in preoperative rehabilitation after the baseline testing [15, 18]. Preoperative rehabilitation consisted of progressive exercise training program in order to restore muscle strength and appropriate neuromuscular responses. This exercise program emphasized specialized perturbation training augmented with aggressive quadriceps strength training. Perturbation training consists of the manipulation of support surfaces directed by physical therapists in order to alter forces and torques in multiple planes in a systematic progression [18]. The three techniques used are the roller board with stationary platform, the roller board, and the rocker board with the objective to either resist the force or to reestablish a balance posture after the perturbation was applied by the therapist. Progression of perturbations was individualized depending upon the subject’s ability to apply appropriate directional and counter-resistive forces, selective muscle activation patterns, and reductions in loss of balance. Quadriceps strength training involved the use of high intensity-low repetition non-weight bearing and weight bearing resisted quadriceps strengthening exercises. Quadriceps strengthening was augmented with neuromuscular electrical stimulation (NMES) if subjects demonstrated a quadriceps strength index of less than 80% [52].
Surgery and post-operative rehabilitation
The surgeon performed either a semitendinosus-gracilis autograft or soft tissue allograft ACL reconstruction. After surgery, the ACL rehabilitation guidelines were followed for all patients [34]. Subjects were systematically progressed through the rehabilitation process based on the clinical milestones outlined in the guidelines. Post-operative rehabilitation guidelines emphasized impairment resolution, aggressive quadriceps strengthening (augmented with NMES if needed), and neuromuscular training [34]. Patients’ progress was monitored using effusion grading and soreness rules [16, 34]. At 8 weeks, if subjects meet the clinical milestones, they received instruction and education on a progressive home exercise prescription consisting of lower extremity strengthening and a walk/jog program [34]. Subjects had to pass predetermined return to sport (RTS) criteria [17, 18] in order to be cleared to progressively return to their sports activities.
Statistical analysis
Frequency counts were used to determine the number of subjects who exhibited greater than 90% in self-reported outcomes and limb symmetry index for quadriceps strength and hop function at 6 and 12 months after reconstruction and to determine those who exhibit IKDC2000 scores within or below normal ranges at 6 and 12 months after reconstruction [22].
To describe the longitudinal outcomes, a mixed model ANOVA with maximum likelihood estimation method was chosen over a general linear model due to its ability to handle missing data [20, 31]. A mixed model repeated measures ANOVA was used to determine the interactions between the limbs over time for quadriceps strength and hop function. If an interaction was significant, post hoc testing included comparisons of limbs at each time period with 90% confidence intervals and the magnitude of the differences between limbs with effect size calculations. The sensitivity to change for involved limb quadriceps strength and hop performance was evaluated over time with a mixed model repeated measures ANOVA with comparison between time intervals using 90% confidence intervals and the magnitude of the differences with effect size calculations [5]. A mixed model repeated measures ANOVA determined the main effects of time for self-reported questionnaires (KOS-ADLS, GRS, IKDC2000). If the main effect is significant, post hoc testing compared the time intervals with 90% confidence intervals and the magnitude of the differences with effect size calculations. Due to the variability in scores that can occur in clinical outcomes research, confidence intervals of 90% were used to detect important differences between limbs or changes over time and to ensure that any differences or changes found that might indicate the need for additional interventions were not excluded.
Results
One hundred and two athletes were recruited for this study. Fourteen subjects chose to pursue non-operative care for their ACL injury. Three subjects were lost to follow-up. One subject did not have ACL surgery due to partial tear identified upon arthroscopy. One subject was transferred to another study. Eighty-three athletes’ data were available for analysis. Table 1 below provides the subject demographic information. Figure 1 shows the reasons for the missing data at each testing period. There were no differences at baseline testing between those who completed the 12-month follow-up (n = 65) and those who did not complete the 12-month follow-up (n = 18), except for baseline QI (P = 0.04) and GRS (P = 0.02). Those who completed the 12-month follow-up had lower QI and GRS compared with those who did not complete the follow-up.
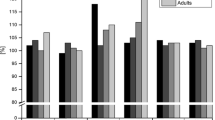
For clinical measurements of quadriceps strength, the involved limb performance was compared with the uninvolved limb performance at each testing period and over time. A significant interaction of limb by time was seen in normalized MVIC (P = 0.02) (Fig. 2). Involved quadriceps strength improved more than the uninvolved quadriceps strength. Post hoc analysis demonstrated that the involved quadriceps improved from baseline to 12 M ACLR (Effect size (ES): 0.6), and the involved quadriceps was weaker than the uninvolved quadriceps at baseline (ES: 0.6).

Performance-based measures at 4 testing periods (Baseline, Post-perturbation, 6 M ACLR, and 12 M ACLR). a Quadriceps strength (MVIC), b Single hop, c Crossover hop, d Triple hop, e 6-m timed hop
For the single, triple, and 6-m timed hop, a significant limb by time interaction was noted (P < 0.007). The involved single and triple hop distance and involved 6-m hop time improved more than the uninvolved single and triple hop distance and uninvolved 6-m hop time, respectively (Fig. 2). Post hoc analysis demonstrated that these three involved limb hop scores improved from baseline to 12 M ACLR (ES: 0.9–1.1). The involved limb hopped less distance than the uninvolved limb at baseline for the single and triple hops (ES: 0.7). For the 6-m timed hop, the involved limb hopped slower at baseline than the uninvolved limb (ES: 0.7). For the crossover hop for distance, a main effect of time was noted (P < 0.001) (Fig. 2). Post hoc analysis found that involved limb crossover hop scores improved from baseline to 12 M ACLR (ES: 1.1). The distances hopped at baseline testing were lower than at post-perturbation testing (ES: 0.8).
For self-reported measures, the outcome scores were evaluated over the testing periods. A main effect for time was seen in KOS-ADLS, GRS, and IKDC2000 (<0.001; Table 2). For the KOS-ADLS, scores at baseline testing were lower than at post-perturbation testing and from post-training testing to 6-m follow-up. For GRS, scores at baseline testing were lower than at post-perturbation testing and from post-perturbation to 6-month follow-up for the GRS. For the IKDC2000, scores were lower at baseline testing compared with post-perturbation testing and post-perturbation to 6-month follow-up.
The percentage of athletes who achieved greater than 90% on self-reported outcome scores improved over time from baseline to 12 months after ACL reconstruction (Table 3). The percentage of subjects who achieved IKDC2000 scores within and below normal ranges improved from 6 months to 12 months after reconstruction (Table 4). Main effects of time were seen in limb symmetry indexes for quadriceps strength and the 4 hop tests (P < 0.04). All mean limb symmetry indexes except single and triple hop limb symmetry indexes were greater than 90% at baseline testing but by the post-perturbation testing, all indexes were greater than 90% (Table 5).
Discussion
The most important findings of this present study are that limb-to-limb asymmetries are reduced, and limb symmetry indexes are restored to greater than 90% after preoperative perturbation training and aggressive quadriceps strengthening. The limb-to-limb differences and indexes return to preoperative levels by 6 months after ACL reconstruction and continue to improve 12 months after ACLR.
At baseline testing, about half of the patients had a quadriceps and hop indexes less than 90%. Limb-to-limb differences and low indexes in quadriceps strength are pervasive after ACL injury [9] and can persist after ACL reconstruction [43]. Deficits in hop performance are present after ACL injury [15, 37] and can still be evident months after ACL reconstruction. Limb asymmetries can influence functional outcomes and gait after ACL reconstruction [12, 14, 30, 32]. Therefore, the restoration of symmetrical function between limbs remains an important goal of ACL rehabilitation. Our results show that mean limb symmetry indexes were greater than 90% after perturbation training and stayed above this threshold after ACL reconstruction. Early restoration of quadriceps strength can result in higher functional outcomes [12, 30]. Likewise, higher hop symmetry indexes can predict knee function after ACL reconstruction [2, 37, 46]. However, at 6 months after ACL reconstruction, up to 23% of athletes still did not exhibit normal limb symmetry for any one hop test. This high number of individuals not having normal limb symmetry is concerning, as most post-surgical rehabilitation guidelines enable individuals to return to sports-specific activities between 4 and 6 months post-ACL reconstruction [8, 36]. These deficits may be magnified in sports-specific activities in a less controlled environment with opponents, resulting in suboptimal performance and predisposing the ipsilateral or contralateral knee to re-injury [39, 44, 51].
All limb symmetry indexes improved over time from baseline to 1 year after ACL reconstruction but were not sensitive to change between time intervals after ACL reconstruction. Only the single hop symmetry index improved greater than the minimal detectable change (8.09%) reported by Reid et al. [45]. The single, triple, and 6-m timed hop indexes showed improvement between baseline to preoperative perturbation training but no limb symmetry index was sensitive to change after reconstruction. Our patients had high indexes at each time period, and less potential was available for detecting change and clinical improvement based on limb symmetry indexes. Risberg et al. [48] found that the single hop, triple hop, and stair hopple test were sensitive to change between 6 and 12 months after ACL reconstruction. However, the change for the triple hop of 3.5% was much less than the minimal detectable change of 10.02% and, therefore, may not be clinically relevant [45, 48].
The involved limb performance-based measures increased significantly over time from baseline to 12 months after ACL reconstruction. Using the 90% confidence interval as a method to make statistical inferences about the means, the confidence intervals at 12 months after reconstruction fell outside the confidence intervals at baseline testing, indicating that the means are different from one another. The involved limb changes exceeded the clinically meaningful change of 3 N/BMI for quadriceps strength [23] and the minimal detectable changes for hop performance reported by Ross et al. [50]. Along with the effect size to determine the magnitude of the differences [41], these measures are able to detect changes over time [15, 26] and are clinically relevant improvements that were not evident when evaluating limb symmetry indexes.
Self-reported outcomes increased significantly from baseline to 6 months after reconstruction. The KOS-ADLS and IKDC2000 outcome scores are responsive and capable of detecting clinically relevant difference over time in patients with ACL reconstruction [27, 28, 35]. We were not surprised to see the KOS-ADLS show no improvement after 6 months as this questionnaire pertains to activities of daily living that most individuals should be able to perform with little to no difficulty 6 months after surgery. The GRS and IKDC2000 showed no improvement with small-to-moderate effect sizes between 6 months and 12 months. We had expected to see greater changes in IKDC2000 after 6 months. Many athletes are transitioning back to activities that involve jumping, cutting, and pivoting which are relevant questions on the IKDC2000. The lack of significant improvement seen by the three self-reported outcomes may be the result of a ceiling effect at 6 months as more than 15% of the patients achieved the maximum scores on each of the self-reported outcomes. Others have reported no ceiling effects in IKDC2000 scores in patients with various knee pathologies [10, 27]. Their patients were substantially older than our patients, had lower preoperative and post-operative scores, and used 30% as the cutoff for ceiling effects [10].
The largest changes between time intervals for the performance-based measures occurred between baseline testing and after post-perturbation training, whereas the largest changes for the self-reported measured occurred between post-perturbation training and 6 months after ACL reconstruction. As the limb symmetry indexes and involved limb performance-based measures at 6 months after surgery were at similar levels as preoperative values, changes in self-reported values were substantially higher. The discrepancies in change scores just prior to surgery and 6 months after surgery may be the result of patients’ perceived response to surgery and subsequent improvements and not their perception of their knee function relative to before surgery. Surgery is traumatic to the knee, resulting in significant physical impairments, activity limitations, and participation restrictions [49]. The largest extent of quadriceps weakness and hop performance is evident in the first months after reconstruction [1, 12]. Improvements in limb symmetry indexes and self-reported outcomes can occur from 3 months to 6 months after ACL reconstruction [23, 26]. Further research should evaluate functional recovery using performance-based and self-reported outcomes throughout the rehabilitation process to capture important clinical changes.
This study has some limitations. The results can only be generalized to individuals who sustain an isolated ACL injury or asymptomatic concomitant injuries and should not be generalized to individuals with symptomatic or complex concomitant injuries. This study was observational and did not include a comparison group. Our patients were all Level I and II active individuals [15, 18], and the results of this study should not be generalized to individuals involved in less demanding activities. Data were not collected at initial physical therapy evaluations. Important clinical changes may have been missed that occurred at time intervals other than the ones we tested.
Conclusions
Limb-to-limb asymmetries are reduced, and normal limb symmetry is restored after perturbation training and aggressive quadriceps strengthening before surgery and returns to similar levels 6 months after reconstruction. Performance-based values on the involved limb and self-reported outcomes are sensitive to change over time and were clinically relevant improvements. The clinical relevance of this work is normal limb symmetry can be restored and functional recovery maximized for patients undergoing ACL reconstruction through a rehabilitation program consisting of perturbation training and aggressive quadriceps strength preoperatively and a systematic criteria-based program post-operatively.
References
Andrade MS, Cohen M, Picarro IC, Silva AC (2002) Knee performance after anterior cruciate ligament reconstruction. Isokinetics Exer Sci 10:81–86
Ardern CL, Webster KE, Taylor NF, Feller JA (2011) Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med 45(7):596–606
Ardern CL, Webster KE, Taylor NF, Feller JA (2011) Return to the preinjury level of competitive sport after anterior cruciate ligament reconstruction surgery: two-thirds of patients have not returned by 12 months after surgery. Am J Sports Med 39(3):538–543
Bach BR Jr, Warren RF, Flynn WM, Kroll M, Wickiewiecz TL (1990) Arthrometric evaluation of knees that have a torn anterior cruciate ligament. J Bone Joint Surg Am 72(9):1299–1306
Beaton DE, Hogg-Johnson S, Bombardier C (1997) Evaluating changes in health status: reliability and responsiveness of five generic health status measures in workers with musculoskeletal disorders. J Clin Epidemiol 50(1):79–93
Beynnon BD, Johnson RJ, Abate JA, Fleming BC, Nichols CE (2005) Treatment of anterior cruciate ligament injuries, part I. Am J Sports Med 33(10):1579–1602
Biau DJ, Tournoux C, Katsahian S, Schranz P, Nizard R (2007) ACL reconstruction: a meta-analysis of functional scores. Clin Orthop Relat Res 458:180–187
Cascio BM, Culp L, Cosgarea AJ (2004) Return to play after anterior cruciate ligament reconstruction. Clin Sports Med 23(3):395–408
Chmielewski TL, Stackhouse S, Axe MJ, Snyder-Mackler L (2004) A prospective analysis of incidence and severity of quadriceps inhibition in a consecutive sample of 100 patients with complete acute anterior cruciate ligament rupture. J Orthop Res 22(5):925–930
Crawford K, Briggs KK, Rodkey WG, Steadman JR (2007) Reliability, validity, and responsiveness of the IKDC score for meniscus injuries of the knee. Arthroscopy 23(8):839–844
Daniel DM, Stone ML, Dobson BE, Fithian DC, Rossman DJ, Kaufman KR (1994) Fate of the ACL-injured patient. A prospective outcome study. Am J Sports Med 22(5):632–644
de Jong SN, van Caspel DR, van Haeff MJ, Saris DB (2007) Functional assessment and muscle strength before and after reconstruction of chronic anterior cruciate ligament lesions. Arthroscopy 23(1):21–28
Dye SF, Wojtys EM, Fu FH, Fithian DC, Gillquist J (1999) Factors contributing to function of the knee joint after injury or reconstruction of the anterior cruciate ligament. Instr Course Lect 48:185–198
Eitzen I, Holm I, Risberg MA (2009) Preoperative quadriceps strength is a significant predictor of knee function two years after anterior cruciate ligament reconstruction. Br J Sports Med 43(5):371–376
Eitzen I, Moksnes H, Snyder-Mackler L, Risberg MA (2010) A progressive 5-week exercise therapy program leads to significant improvement in knee function early after anterior cruciate ligament injury. J Orthop Sports Phys Ther 40(11):705–721
Fees M, Decker T, Snyder-Mackler L, Axe MJ (1998) Upper extremity weight-training modifications for the injured athlete. A clinical perspective. Am J Sports Med 26(5):732–742
Fitzgerald GK, Axe MJ, Snyder-Mackler L (2000) A decision-making scheme for returning patients to high-level activity with nonoperative treatment after anterior cruciate ligament rupture. Knee Surg Sports Traumatol Arthrosc 8(2):76–82
Fitzgerald GK, Axe MJ, Snyder-Mackler L (2000) The efficacy of perturbation training in nonoperative anterior cruciate ligament rehabilitation programs for physical active individuals. Phys Ther 80(2):128–140
Fitzgerald GK, Lephart SM, Hwang JH, Wainner RS (2001) Hop tests as predictors of dynamic knee stability. J Orthop Sports Phys Ther 31(10):588–597
Gadbury GL, Coffey CS, Allison DB (2003) Modern statistical methods for handling missing repeated measurements in obesity trial data: beyond LOCF. Obes Rev 4(3):175–184
Griffin LY, Albohm MJ, Arendt EA, Bahr R, Beynnon BD, Demaio M, Dick RW, Engebretsen L, Garrett WE, Jr., Hannafin JA, Hewett TE, Huston LJ, Ireland ML, Johnson RJ, Lephart S, Mandelbaum BR, Mann BJ, Marks PH, Marshall SW, Myklebust G, Noyes FR, Powers C, Shields C, Jr., Shultz SJ, Silvers H, Slauterbeck J, Taylor DC, Teitz CC, Wojtys EM, Yu B (2006) Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January 2005. Am J Sports Med 34(9):1512–1532
Grindem H, Logerstedt D, Eitzen I, Moksnes H, Axe MJ, Engebretsen L, Snyder-Mackler L, Risberg MA (2011) Single-legged hop tests as predictors of self-reported knee function in nonoperately treated individuals with anterior cruciate ligament injury. Am J Sports Med 39(11):2347–2354
Hartigan EH, Axe MJ, Snyder-Mackler L (2010) Time line for noncopers to pass return-to-sports criteria after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther 40(3):141–154
Higgins LD, Taylor MK, Park D, Ghodadra N, Marchant M, Pietrobon R, Cook C (2007) Reliability and validity of the international knee documentation committee (IKDC) subjective knee form. Joint Bone Spine 74(6):594–599
Hopper DM, Goh SC, Wentworth LA, Chan DYK, Chau JHW, Wootton GJ, Strauss GR, Boyle JJW (2002) Test-retest reliability of knee rating scales and functional hop tests one year following anterior cruciate ligament reconstruction. Phys Ther in Sport 3:10–18
Hopper DM, Strauss GR, Boyle JJ, Bell J (2008) Functional recovery after anterior cruciate ligament reconstruction: a longitudinal perspective. Arch Phys Med Rehabil 89(8):1535–1541
Irrgang JJ, Anderson AF, Boland AL, Harner CD, Kurosaka M, Neyret P, Richmond JC, Shelborne KD (2001) Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med 29(5):600–613
Irrgang JJ, Anderson AF, Boland AL, Harner CD, Neyret P, Richmond JC, Shelbourne KD (2006) Responsiveness of the international knee documentation committee subjective knee form. Am J Sports Med 34(10):1567–1573
Irrgang JJ, Snyder-Mackler L, Wainner RS, Fu FH, Harner CD (1998) Development of a patient-reported measure of function of the knee. J Bone Joint Surg Am 80(8):1132–1145
Keays SL, Bullock-Saxton J, Keays AC, Newcombe P (2001) Muscle strength and function before and after anterior cruciate ligament reconstruction using semitendinosus and gracilis. Knee 8(3):229–234
Krueger C, Tian L (2004) A comparison of the general linear mixed model and repeated measures ANOVA using a dataset with multiple missing data points. Biol Res Nurs 6(2):151–157
Lewek M, Rudolph K, Axe M, Snyder-Mackler L (2002) The effect of insufficient quadriceps strength on gait after anterior cruciate ligament reconstruction. Clin Biomech (Bristol, Avon) 17(1):56–63
Majewski M, Susanne H, Klaus S (2006) Epidemiology of athletic knee injuries: a 10-year study. Knee 13(3):184–188
Manal T, Snyder-Mackler L (1996) Practice guidelines for anterior cruciate ligament rehabilitation: a criterion-based rehabilitation progression. Oper Tech Orthop 6(3):190–196
Marx RG, Jones EC, Allen AA, Altchek DW, O’Brien SJ, Rodeo SA, Williams RJ, Warren RF, Wickiewicz TL (2001) Reliability, validity, and responsiveness of four knee outcome scales for athletic patients. J Bone Joint Surg Am 83-A(10):1459–1469
Marx RG, Jones EC, Angel M, Wickiewicz TL, Warren RF (2003) Beliefs and attitudes of members of the American Academy of Orthopaedic Surgeons regarding the treatment of anterior cruciate ligament injury. Arthroscopy 19(7):762–770
Moksnes H, Risberg MA (2008) Performance-based functional evaluation of non-operative and operative treatment after anterior cruciate ligament injury. Scand J Med Sci Sports 19(3):345–355
Myer GD, Paterno MV, Ford KR, Hewett TE (2008) Neuromuscular training techniques to target deficits before return to sport after anterior cruciate ligament reconstruction. J Strength Cond Res 22(3):987–1014
Myer GD, Paterno MV, Ford KR, Quatman CE, Hewett TE (2006) Rehabilitation after anterior cruciate ligament reconstruction: criteria-based progression through the return-to-sport phase. J Orthop Sports Phys Ther 36(6):385–402
Myklebust G, Holm I, Maehlum S, Engebretsen L, Bahr R (2003) Clinical, functional, and radiologic outcome in team handball players 6–11 years after anterior cruciate ligament injury: a follow-up study. Am J Sports Med 31(6):981–989
Nakagawa S, Cuthill IC (2007) Effect size, confidence interval and statistical significance: a practical guide for biologists. Biol Rev Camb Philos Soc 82(4):591–605
Noyes FR, Barber SD, Mangine RE (1991) Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. Am J Sports Med 19(5):513–518
Palmieri-Smith RM, Thomas AC, Wojtys EM (2008) Maximizing quadriceps strength after ACL reconstruction. Clin Sports Med 27 (3):405–424, vii–ix
Paterno MV, Schmitt LC, Ford KR, Rauh MJ, Myer GD, Huang B, Hewett TE (2010) Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med 38(10):1968–1978
Reid A, Birmingham TB, Stratford PW, Alcock GK, Giffin JR (2007) Hop testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Phys Ther 87(3):337–349
Reinke EK, Spindler KP, Lorring D, Jones MH, Schmitz L, Flanigan DC, An AQ, Quiram AR, Preston E, Martin M, Schroeder B, Parker RD, Kaeding CC, Borzi L, Pedroza A, Huston LJ, Harrell FE Jr, Dunn WR (2011) Hop tests correlate with IKDC and KOOS at minimum of 2 years after primary ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 19(11):1806–1816
Risberg MA, Holm I (2009) The long-term effect of 2 postoperative rehabilitation programs after anterior cruciate ligament reconstruction: a randomized controlled clinical trial with 2 years of follow-up. Am J Sports Med 37(10):1958–1966
Risberg MA, Holm I, Steen H, Beynnon BD (1999) Sensitivity to changes over time for the IKDC form, the Lysholm score, and the Cincinnati knee score. A prospective study of 120 ACL reconstructed patients with a 2-year follow-up. Knee Surg Sports Traumatol Arthrosc 7(3):152–159
Risberg MA, Holm I, Tjomsland O, Ljunggren E, Ekeland A (1999) Prospective study of changes in impairments and disabilities after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther 29(7):400–412
Ross MD, Langford B, Whelan PJ (2002) Test-retest reliability of 4 single-leg horizontal hop tests. J Strength Cond Res 16(4):617–622
Shelbourne KD, Klotz C (2006) What I have learned about the ACL: utilizing a progressive rehabilitation scheme to achieve total knee symmetry after anterior cruciate ligament reconstruction. J Orthop Sci 11(3):318–325
Snyder-Mackler L, Delitto A, Bailey SL, Stralka SW (1995) Strength of the quadriceps femoris muscle and functional recovery after reconstruction of the anterior cruciate ligament. A prospective, randomized clinical trial of electrical stimulation. J Bone Joint Surg Am 77(8):1166–1173
Sturgill LP, Snyder-Mackler L, Manal TJ, Axe MJ (2009) Interrater reliability of a clinical scale to assess knee joint effusion. J Orthop Sports Phys Ther 39(12):845–849
Tanner SM, Dainty KN, Marx RG, Kirkley A (2007) Knee-specific quality-of-life instruments: which ones measure symptoms and disabilities most important to patients? Am J Sports Med 35(9):1450–1458
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Logerstedt, D., Lynch, A., Axe, M.J. et al. Symmetry restoration and functional recovery before and after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 21, 859–868 (2013). https://doi.org/10.1007/s00167-012-1929-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-012-1929-2