
Abstract
Purpose
To evaluate the biomechanical performance of different techniques for CC reconstruction using suture button systems with integrated tendon augmentation. Hypothesis was that (1) reconstructions using a cortical button combined with a biological augmentation (semitendinosus allograft) will demonstrate improved stability than a modified Weaver–Dunn procedure and (2) constructs using two tunnels at the clavicle for fixation will show superior horizontal stability than single-tunnel constructs.
Methods
The acromioclavicular joints of 47 cadaveric shoulders were tested for anterior, posterior, and superior translations (70 N load) and maximal load to failure (superior). Shoulders were assigned to 4 groups: (1) native (n = 18) and after sectioning the AC and CC ligaments; (2) CC reconstruction with 1 clavicular and 1 coracoid tunnel (GR-ST) augmented with semitendinosus graft (n = 15); (3) CC reconstruction augmented with semitendinosus tendon (GR-DT) with 2 clavicular and 1 coracoid tunnel (n = 8); and (4) modified Weaver–Dunn reconstruction (n = 6).
Results
The Weaver–Dunn demonstrated statistically more translation than the native joint for posterior direction (P = 0.038). The GR-ST had significantly less translation than the Weaver–Dunn for anterior and posterior translations (P = 0.003, P = 0.004) and compared to the native for superior translation (P = 0.028). The GR-DT differed significantly in anterior and posterior translations compared to the Weaver–Dunn (P = 0.002, P = 0.001). The modified Weaver–Dunn failed at significantly less load to failure compared to all other groups (P = 0.002, P = 0.002, P = 0.005). There was no significant difference between the native and the other reconstructions.
Conclusion
The evaluated techniques for isolated CC ligament reconstruction (GR-ST) in AC joint dislocation showed biomechanical stability superior to the modified Weaver–Dunn procedure and obtained similar measures compared to the native control. A modified technique (GR-DT), which used two fixation points at the clavicle, did not result in decreased horizontal or vertical translation and therefore no superiority of the GR-DT technique could be shown compared to the GR-ST.
Level of evidence
Controlled laboratory study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A wide range of procedures aiming on a permanent reduction in higher graded acromioclavicular (AC) joint dislocations exist [14]. However, the variability in results and outcome show that none of these can be regarded as the “overall gold standard” [8, 13, 14]. Therefore, biomechanical evaluation of the newer techniques may still contribute to the improvement of current procedures. Techniques aiming on reconstruction of the coracoclavicular (CC) ligaments with cortical button systems or ligament augmentations have the advantage of anatomic positioning and therefore reconstruction of the three-dimensional functions of the AC joint [4, 14, 15, 18, 22, 25]. These techniques can also be performed in a minimally invasive arthroscopic procedure with decreased soft tissue trauma. Although current literature has raised the awareness of the specific role of the AC ligaments for restoring overall horizontal AC joint stability, isolated CC reconstructions have shown sufficient biomechanical and clinical results to rationalize their clinical use, especially if an anatomical procedure was used [5, 15, 18, 22].
The suggested time for surgery to be performed after the injury varies [14]. More recent methods using suture buttons systems without biological augmentation show their best results if reconstructions are performed less than 3 weeks after injury, and if treated at a later time point, these authors suggest a biological augmentation [22]. Specific cortical button systems for such delayed repairs combine a biologic component (e.g., autologous semitendinosus tendon) and the technique of approaching the clavicle and coracoid via the primary fixation (e.g., a cortical button and suture pulley system) [4, 19]. Besides an improved primary stability, this is thought to result in a higher secondary stability when the tendon graft heals into the bone tunnels [21]. In contrast, non-absorbable structures may create too much stiffness of the construct and result in fracture or graft failure.
Debski et al. recommended that the conoid and trapezoid ligaments should not be considered as 1 structure when surgical treatment is considered [6]. With this and the beneficial results of anatomic CC ligament reconstructions (reconstructing the trapezoid and conoid ligament) in mind, a modification of this technique using two bone tunnels at the clavicle was developed [11, 15, 17, 22]. This may potentially improve the overall and specifically the horizontal stability of the reconstruction.
To the authors’ knowledge, only one recently published study evaluated such a combined technique biomechanically [20]. However, only load to failure measurements were compared to native, a modified Weaver–Dunn, a non-anatomic and an anatomic allograft, and an anatomic suture reconstruction technique [20]. Horizontal and vertical motions are currently seen as additional important factors in biomechanical evaluation of AC joint reconstructions. However, there has been no evaluation of horizontal or vertical translation nor any evaluation of the possible beneficial effects of the modified two-tunnel method in this study [20].
The hypotheses were (1) that reconstructions using a cortical button combined with a biological augmentation (hamstring tendon) will show a higher primary stability than a modified Weaver–Dunn procedure and (2) that constructs using two tunnels at the clavicle for fixation will show a superior horizontal stability than that of single-tunnel reconstructions. The purpose of this study was to evaluate the biomechanical performance of the modified Weaver–Dunn, the single clavicle tunnel graft (GR-ST), and the double clavicle tunnel graft (GR-DT) technique for CC reconstruction and compare it to the equivalent of an uninjured AC joint, which served as a “negative control.” The modified Weaver–Dunn reconstruction was selected as the “positive control” since this a still a widespread technique [14]. The aim was to evaluate specifically the isolated CC reconstruction in which the AC ligaments are not surgically addressed.
Materials and methods
Specimen preparation
Forty-seven fresh frozen cadaveric shoulders (mean age: 56.7 ± 9.6 years) were distributed to one of the four groups (Table 1). The study was performed as an extension of a previous study [1]. Therefore, the controls of this precursor study (native and modified Weaver–Dunn group) were used as the controls, as a high number of controls were thought to be beneficial to use rather than having a smaller new group. This was possible because the identical laboratory, experimental setup, and conditions were used for the testing of all specimens. The testing on the GR-ST and GR-DT was performed on new cadaveric specimen.
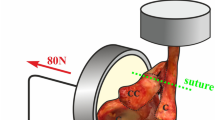
Specimen preparation and biomechanical testing were performed in close accordance with previously published testing protocols [15, 16]. After thawing for 24 h at room temperature, shoulders were dissected free of all soft tissue except the AC joint structures including the CC and AC ligaments. Structures were examined for any degenerative changes or any signs of previous ligamentous injury. Any specimens with suspicion of previous ligamentous injury or degenerative joint disease were excluded from the study. The scapulae were potted in a custom block mold (10 cm × 10 cm) from the inferior angle to the edge of the glenoid using plaster of Paris. The clavicles were fixed in a custom 3.18-cm PVC pipe mold ending just medial to the coracoid process using bone cement [polymethyl methacrylate (PMMA)] [15, 16]. The scapula was allowed to float on a fixture base while the displacement of the actuator was adjusted to a zero load position, thus indicating anatomical origin of the clavicle relative to the scapula. A custom guide was used to drill a 10-mm hole in the potting of the scapula to mate with a permanently mounted bolt on the fixture base [15, 16]. The specimen was then bolted into the prescribed anatomical position, ensuring reproducibility when reinstalling the specimen in the fixture [15]. This configuration allowed the native CC ligaments and reconstructions to be oriented in line with the pull of the MTS machine. Saline solution was applied throughout the experimental protocol to prevent tissue dehydration. Following complete sharp resection of the AC and CC ligaments (trapezoid and conoid) for groups 2, 3, and 4, reconstruction of the CC ligaments was performed according to the specific reconstruction technique.
Reconstruction techniques
Group 1
Native Joint with intact AC and CC ligaments
Group 2
For the single clavicular tunnel (GR-ST) technique, an AC target guide was used to drill a 2.4-mm pin through the center of the clavicle (30 mm medial to the AC joint) and the base of the coracoid. The AC joint was reduced prior to drilling. The pin was overdrilled with a 6-mm cannulated reamer to create a 6-mm tunnel. A 12–15-cm doubled-over semitendinosus graft was prepared and secured to the cortical button and the clavicle washer of a cortical-button-pulley system “Graft Rope®” (Arthrex Inc., Naples, FL) according to the manufacturer’s guidelines. The implantable device consists of two cortical buttons connected by a pulley-cinch mechanism of #5 high-strength suture. A doubled-over semitendinosus allograft is tied to the subcoracoid button using #2 “high-strength” suture. The graft ranged from 4.5 to 5.5 mm in diameter, and approximately 30 mm of each free end was whip-stitched individually starting a point approximately 30 mm from the graft center line. With the help of a passing wire, this construct was passed through the tunnel and the coracoid flip button was blocked under the coracoid. The sutures were tied together over the clavicular button, and a 5.5 × 12-mm PEEK screw (Arthrex Inc., Naples, FL) secured the graft after tensioning it in the clavicle tunnel to complete the reconstruction (Figure 1).

Line drawing of GR-ST reconstruction (Group 2)
Group 3
Similar drilling technique and reamer size (6 mm) was used to place the first tunnel for the double clavicular tunnel (GR-DT) technique The first tunnel was placed 25 mm medial to the AC joint. A second 2.4-mm pin was placed in the clavicle approximately 7 mm medially from the edge of the first 6-mm tunnel and overdrilled using a 6-mm cannulated reamer leaving an approximate 4-mm bone bridge between the tunnels. The graft was assembled with a Graft Rope® according to the single-tunnel technique, but one half of the tendon was not attached to the washer as a free limb. With the distal button seated below the base of the coracoid, the clavicle was reduced and the proximal washer-button was cinched down to the clavicle and tied. The one limb of the semitendinosus allograft was tensioned through the proximal cortical washer-button, and a 5.5 mm × 15 mm biointerference screw was inserted to secure the graft in the clavicle tunnel. The opposing limb was tensioned and fixated in its respective tunnel using a 5.5 mm × 15 mm biointerference screw (Figure 2).

Line drawing of GR-DT reconstruction (Group 3)
Group 4
For the modified Weaver–Dunn Technique, 10 mm of the distal clavicle was excised. Two 1.6-mm drill holes were then made in the superior portion of the clavicle 3 mm from the distal end, exiting into the intramedullary canal. The coracoacromial ligament was then transected sharply from its acromial attachment. A running locking stitch using #2 high-strength suture was weaved into the distal end. The two free ends of the suture were then passed into the drill holes created in the distal clavicle through the medullary canal. The clavicle was then reduced into an anatomical position, and the coracoacromial ligament was secured and tied. Two additional 1.6-mm drill holes, placed 15 mm and 25 mm from the distal end, were created to secure an additional augmentation suture. This suture utilized #2 high-strength suture and was placed to further secure the clavicle to the coracoid by threading the suture around the base of the coracoid and through the drill holes in the distal clavicle.
Biomechanical testing
Biomechanical testing was performed according to previously published methods [15, 16]. In short, the clavicle was fixed to the MTS 858 Bionix II Servohydraulic testing system (MTS Systems Corp, Eden Prairie, MN). The specimen was then bolted into the prescribed anatomical position in the custom fixture. The method used required the clavicle and scapula to remain effectively rigid when they are compared with the soft tissue around the AC joint [15, 16]. On repeated visual inspection before testing, all specimens possessed high-quality cortical bone and were free from any observable disease [11].
After initial specimen preparation, a computer-based random number-generating program was used to assign specimens to 1 of 2 test protocols. Half of the specimens were positioned and first tested in the anterior–posterior (AP) plane, and half were positioned and first tested in the superior plane [15, 16]. After the completion of uniplane testing, specimens were rotated to accommodate testing in the second plane. In this fashion, all specimens were tested for AP and superior displacement. For both AP and superior testing, the clavicle was first fixed perpendicular to the actuator in a non-rigid fashion to allow for calibration of the load cell. The load cell was set at zero, and the clavicle was then rigidly attached [15, 16]. A drill was used to create a path in the scapula-potting fixture, which was then bolted to the frame of the materials testing machine. This allowed precise and consistent repositioning of the scapula fixtures for repeated trials. The scapula was fixed into position and the MTS 858 was adjusted to achieve zero loads, representing the approximate neutral force position [16].
The magnitude of loading selected for this study satisfied the assumption that the scapula and clavicle were rigid bodies with each ligamentous structure located between these two rigid bodies. In preliminary experiments, when a force less than 70 N was applied, bending of the acromion, coracoid process, and clavicle was negligible. These findings are similar to those of Lee et al. who through evaluation of the anteroposterior and superoinferior motion with in situ forces of the ligaments at the AC determined the magnitude of the force vector representing each ligament [12]. This load additionally simulates the weight of the unloaded upper extremity.
Following complete dissection of the AC and CC ligaments, reconstruction of the CC ligaments was performed without addressing the AC ligaments. After reconstruction, specimens were preconditioned from 0 to 25 N for 10 cycles in each direction and then tested to 70 N in three directions: anterior, posterior, and superior. Net actuator displacement values were recorded for each direction. Load to failure testing (120 mm/min) was then performed in superior direction to evaluate maximal loading capacity of the reconstruction [15].
Statistical analysis
Ultimate load to failure, as well as the anterior, posterior, and superior translations in the unpaired specimens, was analyzed for variance (ANOVA) if significant differences were found followed by Bonferroni post hoc analysis. An alpha level of 0.05 was set for all tests for the determination of significance. A power analysis was performed and revealed a minimum of 5 specimens per group for testing. This was calculated using the maximal load to failure for the native joint and the Weaver–Dunn reconstructed joint, since these results were known from a previous study [1]. The difference to detect was set to 260 ± 150 N with an alpha value of .05 (α) and power of 0.80 (1 − β).
Results
Results are demonstrated according to tested translations and final load to failure.
Anterior translation
Anterior translation under load of 70 N was significantly increased for the modified Weaver–Dunn group compared to GR-ST (P = 0.003) and GR-DT (P = 0.002), respectively, but not significantly different compared to the native joint. No significant difference was seen between the other groups (Figure 3).

Anterior translation by the application of a 70 N load for the four groups. GR-ST single clavicle tunnel, GR-DT double clavicle tunnel, WD Weaver–Dunn, * extreme, o outlier
Posterior translation
Posterior translation was significantly increased for the modified Weaver–Dunn group compared to all other groups (P = 0.004, P = 0.001, P = 0.038). No differences were found comparing the native group, GR-ST, or GR-DT (Figure 4).

Posterior translation by the application of a 70 N load for the four groups. GR-ST single clavicle tunnel, GR-DT double clavicle tunnel, WD Weaver–Dunn, o outlier
Superior translation
GR-ST showed significant less superior translation than the native group (P = 0.028). GR-DT and the modified Weaver–Dunn did not differ significantly compared to GR-ST or between each other (Figure 5).

Superior translation by the application of a 70 N load for the four groups. GR-ST single clavicle tunnel, GR-DT double clavicle tunnel, WD Weaver–Dunn, o outlier
Ultimate load to failure
Ultimate load to failure was measured to determine the overall stability against superior displacement. The modified Weaver–Dunn failed at significantly less load to failure compared to all other groups (P = 0.002, P = 0.002, P = 0.005). There was no significant difference when comparing the native to GR-ST or to GR-DT (Figure 6).

Maximal load to failure (N) in superior direction for the four groups. GR-ST single clavicle tunnel, GR-DT double clavicle tunnel, WD Weaver–Dunn
Discussion
The most important finding of this study was that both tested techniques (GR-ST and GR-DT) demonstrated biomechanical stability superior to the modified Weaver–Dunn procedure and obtained similar measures compared to the native control. This was seen for horizontal and vertical translations as well as maximal load to failure according to the first hypothesis. The second hypothesis was that a modification of the GR-ST technique, which used two fixation points at the clavicle, would result in an improved horizontal stability with less translation. This could not be proven and no significant biomechanical superiority of the GR-DT technique could be shown compared to the GR-ST.
The GR-ST technique was chosen for this study because it enables the surgeon to implant a combined device with the potential of an arthroscopically assisted one-step procedure. It joins the advantages known for primary fixation devices (e.g., high primary stability, easy handling, and arthroscopic procedure) with the advantages of adding biologic material to the reconstruction (e.g., ingrowth of tendon graft into bone tunnels, improved secondary stability, reconstruction of “native” ligaments) [4, 18, 19]. To the authors’ knowledge, this was the first study to show an equal biomechanical property with regard to both stability and translation of the GR-ST compared to the native joint. With regard to significant lesser superior translation compared to the native joint, a possible over-constraint has to be discussed [18, 22]. Consequently, the possibility of overstraining should be considered when tensioning and finally fixing the device.
Besides the knowledge of the importance of the AC ligaments for horizontal stability, a possible improvement of 3D stability of the reconstructed AC joint may be realized in reconstructing the conoid and trapezoid ligaments each individually [7, 9, 15, 18, 26]. Walz et al. and Scheibel et al. have published such techniques previously [9, 19, 22]. However, two tunnels of 6 mm diameter at the coracoid may lead to a predetermined breaking point. A possible modification would be the use of the modified GR-DT technique with a single tunnel at the coracoid and fixing the graft limps into two tunnels at the clavicle [22]. Interestingly, the modified technique using two tunnels at the clavicle (GR-DT) showed no superiority compared to the GR-ST in terms of horizontal or vertical translation. A previous study comparing a modified cortical button device with two tunnels at the clavicle showed a tendency of improvement although there have also been no significant advantages seen [1].
The modified Weaver–Dunn was chosen as the “positive control” in accordance with previously published studies because it is a widely used technique that serves as a reference for subsequent development of current procedures [2, 10, 15, 23]. Previously the integration of biologic material was an advantage reserved to the Weaver–Dunn procedure as well as other techniques, just using a tendon graft without additional non-biologic stabilization. The tested modification of the Weaver–Dunn technique addresses its known inferiority of this technique in terms of primary stability by combining transfer of the CA ligament with an additional fixation using a non-resorbable suture system [24, 27]. Previous studies have demonstrated that combining a CA ligament transfer with a CC ligament reconstruction (tendon graft) did not result in superior biomechanical properties of the construct [3].
There are obvious weaknesses in this study. The in vitro nature of biomechanical evaluation can be a limiting factor in translating findings to the in vivo conditions of the shoulder complex. This is particularly true in the AC joint with its specific 3D forces and complex contributions to multiple shoulder motions, and replicating these forces accurately in a cadaveric study might be difficult. Additionally, biomechanical testing with cadaveric specimen does not allow inclusion of biological healing in testing and therefore conclusions can only be drawn for the time zero findings of the joint at a time point immediately following surgical reconstruction. This is of specific importance, since the augmentation with a biologic graft is intended to improve further stability by healing into the bone tunnels. Stabilization techniques commonly include a discussion of possibly resulting over-constraint. Direct joint pressure or friction inside the AC joint could not be measured due to the setup of this study. However, it has to be recognized that the biomechanical properties of the tested reconstructions may be too stiff and may lead to coracoid or clavicle fractures.
The aim of this study was to present biomechanical data of a newer surgical technique featuring a cortical suspension button and pulley system. These data give additional information to surgeons and that from a biomechanical perspective appear to control anterior, posterior, and superior translations in a satisfactory manner. In addition, this procedure has the potential to be done in an arthroscopic-assisted manner [4].
Conclusions
The tested techniques for isolated CC ligament reconstruction (GR-ST) in AC joint dislocation showed biomechanical stability superior to the modified Weaver–Dunn procedure and obtained similar measures compared to the native control. A modified technique (GR-DT), which used two fixation points at the clavicle, did not result in decreased horizontal or vertical translation and therefore no superiority of the GR-DT technique could be shown compared to the GR-ST.
References
Beitzel K, Obopilwe E, Chowaniec DM, Niver GE, Nowak MD, Hanypsiak BT, Guerra JJ, Arciero RA, Mazzocca AD (2011) Biomechanical comparison of arthroscopic repairs for acromioclavicular joint instability: suture button systems without biological augmentation. Am J Sports Med 39(10):2218–2225
Boileau P, Old J, Gastaud O, Brassart N, Roussanne Y (2010) All-arthroscopic Weaver-Dunn-Chuinard procedure with double-button fixation for chronic acromioclavicular joint dislocation. Arthroscopy 26(2):149–160
Clevenger T, Vance RE, Bachus KN, Burks RT, Tashjian RZ (2011) Biomechanical comparison of acromioclavicular joint reconstructions using coracoclavicular tendon grafts with and without coracoacromial ligament transfer. Arthroscopy 27(1):24–30
DeBerardino TM, Pensak MJ, Ferreira J, Mazzocca AD (2010) Arthroscopic stabilization of acromioclavicular joint dislocation using the AC graftrope system. J Should Elbow Surg 19(2 Suppl):47–52
Debski RE, Parsons IM III, Fenwick J, Vangura A (2000) Ligament mechanics during three degree-of-freedom motion at the acromioclavicular joint. Ann Biomed Eng 28(6):612–618
Debski RE, Parsons IMt, Woo SL, Fu FH (2001) Effect of capsular injury on acromioclavicular joint mechanics. J Bone Joint Surg Am 83-A(9):1344–1351
Fukuda K, Craig EV, An KN, Cofield RH, Chao EY (1986) Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 68(3):434–440
Geaney LE, Miller MD, Ticker JB, Romeo AA, Guerra JJ, Bollier M, Arciero RA, DeBerardino TM, Mazzocca A (2010) Management of the failed AC joint reconstruction: causation and treatment. Sports Med Arthrosc 18(3):167–172
Gerhardt C, Kraus N, Pauly S, Scheibel M (2011) Arthroscopically assisted stabilization of acute injury to the acromioclavicular joint with the double TightRope technique: One-year results. Unfallchirurg. PMID: 21766203
Hosseini H, Friedmann S, Troger M, Lobenhoffer P, Agneskirchner JD (2009) Arthroscopic reconstruction of chronic AC joint dislocations by transposition of the coracoacromial ligament augmented by the Tight Rope device: a technical note. Knee Surg Sports Traumatol Arthrosc 17(1):92–97
Lee KW, Debski RE, Chen CH, Woo SL, Fu FH (1997) Functional evaluation of the ligaments at the acromioclavicular joint during anteroposterior and superoinferior translation. Am J Sports Med 25(6):858–862
Lee SJ, Nicholas SJ, Akizuki KH, McHugh MP, Kremenic IJ, Ben-Avi S (2003) Reconstruction of the coracoclavicular ligaments with tendon grafts: a comparative biomechanical study. Am J Sports Med 31(5):648–655
Lizaur A, Sanz-Reig J, Gonzalez-Parreno S (2011) Long-term results of the surgical treatment of type III acromioclavicular dislocations: an update of a previous report. J Bone Joint Surg Br 93(8):1088–1092
Mazzocca AD, Arciero RA, Bicos J (2007) Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med 35(2):316–329
Mazzocca AD, Santangelo SA, Johnson ST, Rios CG, Dumonski ML, Arciero RA (2006) A biomechanical evaluation of an anatomical coracoclavicular ligament reconstruction. Am J Sports Med 34(2):236–246
Mazzocca AD, Spang JT, Rodriguez RR, Rios CG, Shea KP, Romeo AA, Arciero RA (2008) Biomechanical and radiographic analysis of partial coracoclavicular ligament injuries. Am J Sports Med 36(7):1397–1402
Rios CG, Arciero RA, Mazzocca AD (2007) Anatomy of the clavicle and coracoid process for reconstruction of the coracoclavicular ligaments. Am J Sports Med 35(5):811–817
Salzmann GM, Paul J, Sandmann GH, Imhoff AB, Schottle PB (2008) The coracoidal insertion of the coracoclavicular ligaments: an anatomic study. Am J Sports Med 36(12):2392–2397
Scheibel M, Ifesanya A, Pauly S, Haas NP (2008) Arthroscopically assisted coracoclavicular ligament reconstruction for chronic acromioclavicular joint instability. Arch Orthop Trauma Surg 128(11):1327–1333
Thomas K, Litsky A, Jones G, Bishop JY (2011) Biomechanical comparison of coracoclavicular reconstructive techniques. Am J Sports Med 39(4):804–810
Tsukada H, Ishibashi Y, Tsuda E, Kusumi T, Kohno T, Toh S (2010) The actual tendon-bone interface strength in a rabbit model. Arthroscopy: the journal of arthroscopic & related surgery: official publication of the Arthroscopy Association of North America and the International Arthroscopy Association 26(3):366-374
Walz L, Salzmann GM, Fabbro T, Eichhorn S, Imhoff AB (2008) The anatomic reconstruction of acromioclavicular joint dislocations using 2 TightRope devices: a biomechanical study. Am J Sports Med 36(12):2398–2406
Weaver JK, Dunn HK (1972) Treatment of acromioclavicular injuries, especially complete acromioclavicular separation. J Bone Joint Surg Am 54(6):1187–1194
Wellmann M, Lodde I, Schanz S, Zantop T, Raschke MJ, Petersen W (2008) Biomechanical evaluation of an augmented coracoacromial ligament transfer for acromioclavicular joint instability. Arthroscopy 24(12):1395–1401
Wellmann M, Zantop T, Petersen W (2007) Minimally invasive coracoclavicular ligament augmentation with a flip button/polydioxanone repair for treatment of total acromioclavicular joint dislocation. Arthroscopy 23(10):1132.e1–e5
Yoo YS, Tsai AG, Ranawat AS, Bansal M, Fu FH, Rodosky MW, Smolinski P (2010) A biomechanical analysis of the native coracoclavicular ligaments and their influence on a new reconstruction using a coracoid tunnel and free tendon graft. Arthroscopy 26(9):1153–1161
Zooker CC, Parks BG, White KL, Hinton RY (2010) TightRope versus fiber mesh tape augmentation of acromioclavicular joint reconstruction: a biomechanical study. Am J Sports Med 38(6):1204–1208
Acknowledgments
The University of Connecticut Health Center/New England Musculoskeletal Institute has received direct funding and material support for this study from Arthrex Inc. (Naples, Fl). The company had no influence on study design, data collection or interpretation of the results or the final manuscript. Dr Mazzocca receives research support and is a consultant for Arthrex Inc. Dr Hanypsiak receives royalties from Franz Medical Group (Mentor, Ohio) and Arthrex Inc. Dr Guerra is a consultant for Arthrex Inc. The authors would like to thank Mr. Marco Marchionni for the technical illustrations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Beitzel, K., Obopilwe, E., Chowaniec, D.M. et al. Biomechanical properties of repairs for dislocated AC joints using suture button systems with integrated tendon augmentation. Knee Surg Sports Traumatol Arthrosc 20, 1931–1938 (2012). https://doi.org/10.1007/s00167-011-1828-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-011-1828-y