
Abstract
Purpose
Both high tibial valgus osteotomy (HTO) and unicompartmental medial knee arthroplasty (UKA) are established methods for the treatment for moderate stages of OA. This is the first global meta-analysis to compare the long-term effects of both methods regarding survival, outcomes and complications of total arthroplasty.
Methods
Literature research was performed using established medical databases: MEDLINE (via PubMed), EMBASE (via OVID) and the Cochrane register. Criteria for inclusion were as follows: English or German papers, a clinical trial with a clear description of survival, an outcome evaluation using a well-described knee score and a follow-up >5 years. Statistical analysis was performed using the special meta-analysis software called “Comprehensive Meta Analysis” (version 2.0; Biostat, Englewood, NJ, USA).
Results
Final meta-analysis after the full-text review included 46 studies about valgus HTO and 43 studies about medial UKA. There were no significant differences between valgus HTO and medial UKA in terms of the number of total required replacements. After a 5- to 8-year follow-up, 91.0% of the valgus HTO patients and 91.5% of medial UKA patients did not need a total replacement. This value was 84.4% for valgus HTOs and 86.9% for medial UKAs after a 9- to 12-year follow-up. Mean survival time to TKA was 9.7 years after valgus HTO and 9.2 years after medial UKA. Clinical outcome was significantly better after medial UKA in a 5- to 12-year follow-up. After more than 12 years, results were comparable in both groups. No significant differences were seen in the complication rates.
Conclusions
This meta-analysis aimed to find the advantages and disadvantages of two established methods for the treatment for medial compartment knee osteoarthritis. Valgus HTO is more appropriate for younger patients who accept a slight decrease in their physical activity. Medial UKA is appropriate for older patients obtaining sufficient pain relief but with reduced physical activity.
Level of evidence
II.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Knee osteoarthritis (OA) is a frequent orthopedic disease [14]. Treatment includes both conservative and operative options that depend on the patient’s individual characteristics and disease stage. The disease is generally staged by a radiological classification, as detailed in Kellgren and Lawrence [51]. Today, total knee arthroplasty (TKA) is the method of choice for the treatment for symptomatic late-stage OA. Moderate-grade stages of the disease require an individualized approach. Both high tibial valgus osteotomy (HTO) and unicompartmental medial knee arthroplasty (UKA) are established methods for the treatment for medial moderate OA.
Valgus HTO was first described in 1960s [18, 22, 61, 86]. This method is used for medial unicompartmental knee OA. It aims for a mild valgus correction and a shift of the mean bearing axis into the non-affected lateral compartment.
Nearly in the same period, unicompartmental arthroplasty was established [39]. This method aims to replace only the damaged compartment and thus protects the unaffected joint compartments.
Valgus HTO is more appropriate for younger patients who accept a slight decrease in their physical activity. Medial UKA is appropriate for older patients obtaining sufficient pain relief but with reduced physical activity.
Consent on the best indication was unknown until now. Many studies and partially controversial results have been published. This is the first meta-analysis to compare the impacts of both methods on the treatment for unicompartmental medial knee OA.
Materials and methods
Retrieval of published studies and inclusion and exclusion criteria
Literature search was performed using the following established medical databases: MEDLINE (via PubMed), EMBASE (via OVID) and the Cochrane register. Retrieval in PubMed was conducted using the following combination: Knee [Mesh] AND Osteotomy [Mesh], Knee [Mesh] and Unicondylar [Mesh] OR Unicompartmental [Mesh] AND Knee.
Criteria for inclusion were as follows: English or German papers, a clinical trial with a clear description of survival, an outcome evaluation using a well-described knee score and a long-term follow-up (minimum 5 years).
In the first step, two investigators (the first and senior authors) independently reviewed the titles and abstracts of all of the retrieved studies. Second, both investigators hold a conference and found a consensus about which studies were to be evaluated with a full-text review. Then, a full-text review was performed independently by the two lead investigators. After determining the results of the second review, the studies were indentified for their final inclusion into the meta-analysis. Data extraction was performed by both investigators. Results were entered into an Excel table. The established and well-described scores were normalized to a 0-to-100 scale. Before the statistical evaluation, both investigators fine-tuned the results once again.
Statistical analysis
Statistical analysis was performed using the special meta-analysis software called “Comprehensive Meta Analysis” (version 2.0; Biostat, Englewood, NJ, USA).
All of the effect sizes were calculated using a random-effects model. Dichotomous effect sizes (rate of survival, rate of complications and a semi-quantitative estimate of the results) were expressed as ERs (event rates). Continuous values (estimates determined from the knee scores) were calculated by comparing their means (t test). Scores (baseline to follow-up) were compared by calculating the standard difference of the means (SDM). All of the results were presented as forest plots. Results of the scores were normalized to a 0-to-100 scale. In other words, results were calculated as [x = (points) × 100/(maximum possible score points)].
A 95% confidence interval was given for each effect size.
Heterogeneity was calculated according to the method of Higgins et al. [44]. Heterogeneity is expressed as I 2. This value ranges from 0% (complete consistency) to 100% (complete inconsistency).
Results
Included studies
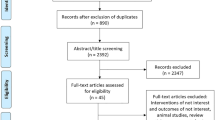
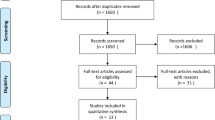
The deadline for evaluation in the databases was July 31, 2010. Primary search resulted in 1,400 studies about valgus HTO and 895 studies about medial UKA.
Final meta-analysis after the full-text review included 46 studies about valgus HTO and 43 studies about medial UKA. Flowcharts describing the study selection are in Figs. 1, 2. Mean age of patients at operation who had undergone valgus HTO was 56.1 years (95% CI, 53.2–58.7 years). Medial UKA patients were significantly (P < 0.001) older. Mean age at operation was 70.1 years (95% CI, 67.3–72.7 years).

Flowchart for the identification of valgus HTO studies

Flowchart for the identification of medial UKA studies
Comparative studies
Only one randomized prospective study was identified. Borjesson et al. [12] reported the 5-year results of 18 valgus HTO patients (closed-wedge technique) versus 22 medial UKAs. During the follow-up, no significant difference in the subjective outcome (BOA Score) was found.
Broughton et al. [13] published the 10-year results of a retrospective comparative study. They found a significant better outcome after a medial UKA. Survival was 0.711 for valgus HTO (n = 49) and 0.913 for medial UKA (n = 42). In HSS, 76.1% of the medial UKAs had good or excellent outcomes. This rate was 42.8% in the valgus HTO group.
Stukenborg-Colsman et al. [94] also retrospectively assessed the 7.5-year outcome after 32 valgus HTOs and 28 medial UKAs. The 5- to 10-year survival after a valgus HTO was 0.688 and 0.800 after a medial UKA. In KSS, 71% of the valgus HTO patients and 65% of the medial UKA patients had an excellent outcome.
Survival
Survival was defined as the time to a total arthroplasty revision. ERs for survival were grouped as follows: 5–8 [mean] years, 9–12 years and more than 12 years of follow-up.
At 5–8 years, 91.0% of the valgus HTO patients and 91.5% of the medial UKA patients did not require a TKA revision (Fig. 3). Within 9–12 years after the operation, 84.4% of the valgus HTO patients and 86.9% of the medial UKA patients did not require revision (Fig. 4). After more than 12 years, valgus HTO tended to be revised more frequently (n.s). Survival to revision was 70.1% in the valgus HTO patients and 77.5% in the medial UKA patients (Fig. 5).

Survival to endpoint total knee arthroplasty after 5–8 years of follow-up. The forest plots present the effect size (ER event rate). Each square represents the individual study’s ER with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 30; medial UKA, n = 26. Survival: valgus HTO, 0.910; medial UKA, 0.915. Heterogeneity (I 2): HTO = 71.1, UKA = 82.3. Significance: P = 0.801

Survival to endpoint total knee arthroplasty after 9–12 years of follow-up. The forest plots present the effect size (ER event rate). Each square represents the individual study’s ER with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 28; medial UKA, n = 25. Survival: valgus HTO, 0.844; medial UKA, 0.869. Heterogeneity (I 2): HTO = 89.5, UKA = 92.0. Significance: P = 0.458

Survival to endpoint total knee arthroplasty after more than 12 years of follow-up. The forest plots present the effect size (ER event rate). Each square represents the individual study’s ER with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 15; medial UKA, n = 9. Survival: valgus HTO, 0.701; medial UKA, 0.775. Heterogeneity (I 2): valgus HTO = 93.7, medial UKA = 95.9, Significance: P = 0.451
In 17 studies, the survival time to revision was calculated according to the method of Kaplan–Meier (Figs. 6, 7). Time of the required revision tended to be sooner in the medial UKA patients than in the valgus HTO patients (n.s). Medial UKA patients were revised after a mean of 8.2 years, while the valgus HTO patients had undergone a revision 1 year later at a mean of 9.7 years (Tables 1, 2).

Mean survival (Kaplan–Maier). The forest plots present the mean survival of each study. Each square represents the individual study’s mean survival with a 95% CI indicated by the horizontal lines. Number of included studies: HTO, n = 12; UKA, n = 5. Mean survival: valgus HTO, 9.7 years; medial UKA, 8.2 years. Heterogeneity (I 2): valgus HTO = 96.0, medial UKA 92.1. Significance: P = 0.374

Mean survival (Kaplan–Meier) funnel plot
Outcome measurement using established knee scores (continuous values)
The papers that were included in this investigation are listed in Table 3. For outcome evaluation, following different scores were used.
BOA (British Orthopaedic Association; n = 2) [1]; Bristol or synonymous Baily score (n = 1) [58]; Conventry score (n = 3) [19]; HSS (Hospital for Special Surgery score; n = 30) [77]; JOA (Japanese Orthopaedic Association; n = 8) [82]; KOOS (Knee Injury And Surgery Outcome score; n = 1) [81]; KSS (Knee Society score) or synonymous Insall score (n = 21) [47]; and the Lysholm score (n = 1) [57]. Each study used a self-created 100-point score. This score was well described and similar to the other scores.
Dates at baseline (Fig. 8) were extracted from 19 papers (for valgus HTO group, the mean score was 60.1 and medial UKA group 55.9; n.s.).

Mean normalized knee scores at baseline. The forest plots present the mean score of each study. Each square represents the individual study’s mean score with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 14; medial UKA, n = 5. Mean: valgus HTO, 60.1; medial UKA, 55.9. Heterogeneity (I 2): valgus HTO = 98.5, medial UKA = 99.6, Significance: P = 0.496
There was a significant difference between valgus HTO and medial UKA in the 5- to 8-year follow-up (P < 0.001). Mean score was 83.4 in the valgus HTO patients and 91.2 in the medial UKA patients (Fig. 9).

Mean normalized knee score after 5–8 years of follow-up. The forest plots present the mean score of each study. Each square represents the individual study’s mean score with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 7; medial UKA, n = 5. Mean: valgus HTO, 83.4; medial UKA, 91.2. Heterogeneity (I 2): valgus HTO = 94.2, medial UKA = 96.6. Significance: P < 0.001
Only one study reported 10-year results after medial UKA. In this study, mean score was 90.0. Mean score in the 9 valgus HTO papers was 79.9. Results from Price et al. [75, 76] were significantly better (P < 0.001) than results from the valgus HTO papers (Fig. 10).

Mean normalized knee score after 9–12 years of follow-up. The forest plots present the mean score of each study. Each square represents the individual study’s mean score with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 9; medial UKA, n = 1. Mean: valgus HTO, 79.9; medial UKA, 90.0. Heterogeneity (I 2): valgus HTO = 85.9; medial UKA is not adjustable. Significance: P < 0.001
A total of 5 papers (2 valgus HTO and 3 medial UKA) reported results beyond 12 years. The outcome of medial UKA (mean 65.6) tended to be better than the outcome of valgus HTO (mean, 58.8; n.s). Results are shown in Fig. 11.

Mean normalized knee score after more than 12 years of follow-up. The forest plots present the mean score of each study. Each square represents the individual study’s mean score with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 2; medial UKA, n = 3. Mean valgus HTO, 58.8; medial UKA, 65.6. Heterogeneity (I 2): valgus HTO = 89.2, medial UKA = 92.3. Significance: P = 0.331
Whenever possible, the baseline score was compared to the score at the 5- to 8-year follow-up, 9- to 12-year follow-up or the >12-year follow-up. SDM after valgus HTO tended to increase more in the valgus HTO studies (SDM = 5.0) compared with the medial UKA studies (4.1) after a 5- to 8-year follow-up (Fig. 12; n.s.).

Weighted (standardized) mean (SDM) of the score from baseline to 5–8 years of follow-up. The forest plots present the SDMs of each study. Each square represents the individual study’s SDM with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 7; medial UKA, n = 3. SDM: valgus HTO, 5.0; medial UKA, 4.1. Heterogeneity (I 2): valgus HTO = 97.5; medial UKA = 60.1. Significance: P = 0.359
Only the study by Price et al. [76] was available to compare the valgus HTO results (n = 8 studies) between baseline and the 9- to 12-year follow-up. In this study, the 9- to 12-year SDM was 10.7, whereas the SDM of the 8 valgus HTO studies was only 1.7 (Fig. 13). This difference was significant (P < 0.001).

Weighted (standardized) mean (SDM) of the score from baseline to 9–12 years of follow-up. The forest plots present the SDMs of each study. Each square represents the individual study’s SDM with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO: n = 8; medial UKA: n = 1. SDM: valgus HTO, 1.7; medial UKA, 10.7. Heterogeneity (I 2): valgus HTO = 95.4. Heterogeneity (I 2) was not adjustable. Significance: P < 0.001
Only 2 studies with very long-term results (>12-year follow-up) were identified. Mercier et al. [64] reported an SDM of approximately 1.2 after valgus HTO. Sprenger and Doerzbacher [88] found an SDM of −0.2 after 12 years. The difference between these studies was not significant (n.s; Fig. 14).

Weighted (standardized) mean (SDM) of the score from baseline to more than 12 years of follow-up. The forest plots present the SDMs of each study. Each square represents the individual study’s SDM with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 1; medial UKA, n = 1. SDM: valgus HTO, −0.2; medial UKA, 1.2. Heterogeneity was not adjustable. Significance: P = 0.603
Outcome measurement using established knee scores (semi-quantitative estimation)
In some papers, the result was estimated by establishing knee scores, and the results were expressed as semi-quantitative estimates. No significant differences between valgus HTO and medial UKA were observed (Table 3, Fig. 15).

Semi-quantitative estimation of the clinical outcome based on the evaluation using clinical scores. The detailed ESs are given in Table 4
Complications
In general, there were more complications after a valgus HTO (13.8%) than after a medial UKA (11.3%; n.s). Forest plots are shown in Fig. 16.

Complication rates. The forest plots present the effect sizes (ER event rate). Each square represents the individual study’s ER with a 95% CI indicated by the horizontal lines. Number of included studies: valgus HTO, n = 31; medial UKA, n = 13. Complications: valgus HTO, 0.138; medial UKA, 0.113. Heterogeneity (I 2): valgus HTO = 82.0, medial UKA = 70.2. Significance: P = 0.369
Discussion
The most important finding of this study was both valgus HTO and medial UKA are sufficient operative treatment options for symptomatic medial knee osteoarthritis.
This meta-analysis was undertaken to compare the impacts of valgus HTO and medial UKA on the treatment for symptomatic unicondylar medial knee osteoarthritis. Survival rates to total knee replacement were not different. Over time, both groups exhibited increased revision rates. Clinical outcome of medial UKA is better than that of valgus HTO. After more than 12 postoperative years, patients in both groups exhibited worsening clinical outcomes.
Both methods are clinically very interesting. This is reflected by the large number of published studies on this topic. In this meta-analysis, we excluded studies with follow-ups >5 years and studies that did not enable the evaluation of concrete effect sizes. Furthermore, clear duplicates were excluded from this evaluation. This was also considered for the results of the central arthroplasty registers [28, 53, 55, 60]. An important limitation is the large heterogeneity of the studies (range, 70–95%). Only 3 comparative [12, 13, 94] studies were found on this topic. The survival and outcome results of these studies are contradictory.
Both valgus HTO and medial UKA are, in principle, sufficient for the treatment for medial knee osteoarthritis.
A valgus HTO corrects varus malalignment by transferring the load to the relatively unaffected lateral compartment. This can be accompanied by pain relief and improvements in gait and function. Mechanical release alone or a combination of HTO with arthroscopic measures (debridement, synovectomy or microfracture), chondral resurfacing or meniscal transplantation can also improve these results [25, 83]. The main benefit for the patient is the preservation of the natural joint. The main advantage for the patient is that potential physical loading (professional or sports-related) is almost entirely unaffected. The limits of valgus HTO are failure of medial compartment restoration, progression of medial degeneration, progression of degeneration in the patellofemoral or lateral compartment and development of pathological valgus. However, in most patients, this method is generally sufficient for avoiding a TKA for about 10 years. Moreover, a revision to a TKA generally does not cause problems [33, 97].
With the proviso that very excellent results are seldom achieved, the valgus HTO can be considered to be the method of choice for younger and physically active patients who are suffering from unicompartmental knee osteoarthritis.
Unlike medial UKA, this treatment addresses the reconstruction of the joint surface by replacing the degenerated joint part and preserving the unaffected joint. A correction of axial misalignment is seldom possible. The main limitation of medial UKA is partially similar to that of valgus HTO (progression of osteoarthritis). The method is comparable to valgus HTO but with a slightly lower complication rate and a shorter rehabilitation time. This outcome is associated with a better 12-year knee score outcome. However, this method also has important disadvantages. Medial UKA requires restricted physical activity. This may be a reason for the higher mean age of the patients who undergo medial UKA. If needed, a revision from medial UKA to total arthroplasty causes more problems and worsens the worse result [7].
Conclusions
This meta-analysis examined the advantages and disadvantages of two established methods for treatment for medial compartment knee osteoarthritis. Valgus HTO is more appropriate for younger patients who accept slight decreases in physical activity in their lifestyles. Medial UKA is a good method for older patients who need painless but reduced physical activity.
References
Aglietti P, Buzzi R, Vena LM, Baldini A, Mondaini A (2003) High tibial valgus osteotomy for medial gonarthrosis: a 10- to 21-year study. J Knee Surg 16:21–26
Akizuki S, Shibakawa A, Takizawa T, Yamazaki I, Horiuchi H (2008) The long-term outcome of high tibial osteotomy: a ten- to 20-year follow-up. J Bone Joint Surg Br 90:592–596
Amin AK, Patton JT, Cook RE, Gaston M, Brenkel IJ (2006) Unicompartmental or total knee arthroplasty? Results from a matched study. Clin Orthop Relat Res 451:101–106
Aoki Y, Yasuda K, Mikami S, Ohmoto H, Majima T, Minami A (2006) Inverted V-shaped high tibial osteotomy compared with closing-wedge high tibial osteotomy for osteoarthritis of the knee. Ten-year follow-up result. J Bone Joint Surg Br 88:1336–1340
Barck AL (1989) 10-year evaluation of compartmental knee arthroplasty. J Arthroplast 4(Suppl:S49–S54)
Becker R, John M, Neumann WH (2004) Clinical outcomes in the revision of unicondylar arthoplasties to bicondylar arthroplasties. A matched-pair study. Arch Orthop Trauma Surg 124:702–707
Benzakour T, Hefti A, Lemseffer M, El Ahmadi JD, Bouyarmane H, Benzakour A (2010) High tibial osteotomy for medial osteoarthritis of the knee: 15 years follow-up. Int Orthop 34:209–215
Berger RA, Nedeff DD, Barden RM, Sheinkop MM, Jacobs JJ, Rosenberg AG, Galante JO (1999) Unicompartmental knee arthroplasty. Clinical experience at 6- to 10-year followup. Clin Orthop Relat Res 367:50–60
Bert JM (1998) 10-year survivorship of metal-backed, unicompartmental arthroplasty. J Arthroplast 13:901–905
Billings A, Scott DF, Camargo MP, Hofmann AA (2000) High tibial osteotomy with a calibrated osteotomy guide, rigid internal fixation, and early motion. Long-term follow-up. J Bone Joint Surg Am 82:70–79
BOA (1978) A knee function assessment chart. From the British Orthopaedic Association Research Sub-Committee. J Bone Joint Surg Br 60-B:308–309
Borjesson M, Weidenhielm L, Mattsson E, Olsson E (2005) Gait and clinical measurements in patients with knee osteoarthritis after surgery: a prospective 5-year follow-up study. Knee 12:121–127
Broughton NS, Newman JH, Baily RA (1986) Unicompartmental replacement and high tibial osteotomy for osteoarthritis of the knee. A comparative study after 5–10 years’ follow-up. J Bone Joint Surg Br 68:447–452
Buckwalter JA, Saltzman C, Brown T (2004) The impact of osteoarthritis: implications for research. Clin Orthop Relat Res 427:S6–S15
Cartier P, Khefacha A, Sanouiller JL, Frederick K (2007) Unicondylar knee arthroplasty in middle-aged patients: a minimum 5-year follow-up. Orthopedics 30:62–65
Choi HR, Hasegawa Y, Kondo S, Shimizu T, Ida K, Iwata H (2001) High tibial osteotomy for varus gonarthrosis: a 10- to 24-year follow-up study. J Orthop Sci 6:493–497
Christodoulou NA, Tsaknis RN, Sdrenias CV, Galanis KG, Mavrogenis AF (2005) Improvement of proximal tibial osteotomy results by lateral retinacular release. Clin Orthop Relat Res 441:340–345
Coventry MB (1965) Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee. A preliminary report. J Bone Joint Surg Am 47:984–990
Coventry MB (1973) Osteotomy about the knee for degenerative and rheumatoid arthritis. J Bone Joint Surg Am 55:23–48
Coventry MB, Ilstrup DM, Wallrichs SL (1993) Proximal tibial osteotomy. A critical long-term study of eighty-seven cases. J Bone Joint Surg Am 75:196–201
Daniilidis K, Skwara A, Skuginna A, Fischer F, Tibesku CO (2009) Comparison of medium-term clinical and radiological outcome between cemented and cementless medial unicompartmental knee arthroplasty. Z Orthop Unfall 147:188–193
De MP, Maquet P, Simonet J (1963) Biomechanical consideration of arthrosis of the knee. 1. Introduction. Some remarks on radiographs. Rev Rhum Mal Osteoartic 30:775–776
Devgan A, Marya KM, Kundu ZS, Sangwan SS, Siwach RC (2003) Medial opening wedge high tibial osteotomy for osteoarthritis of knee: long-term results in 50 knees. Med J Malaysia 58:62–68
Eickmann TH, Collier MB, Sukezaki F, McAuley JP, Engh GA (2006) Survival of medial unicondylar arthroplasties placed by one surgeon 1984–1998. Clin Orthop Relat Res 452:143–149
Elattar M, Dhollander A, Verdonk R, Almqvist KF, Verdonk P (2011) Twenty-six years of meniscal allograft transplantation: is it still experimental? A meta-analysis of 44 trials. Knee Surg Sports Traumatol Arthrosc 19:147–157
Emerson RH Jr, Higgins LL (2008) Unicompartmental knee arthroplasty with the oxford prosthesis in patients with medial compartment arthritis. J Bone Joint Surg Am 90:118–122
Endres S, Steinheiser E, Wilke A (2005) Minimally Invasive Stryker-Osteonics unicondylar knee prosthesis with metal-backed tibia component: a 5-year follow-up. Z Orthop Ihre Grenzgeb 143:573–580
Espehaug B, Furnes O, Havelin LI, Engesaeter LB, Vollset SE, Kindseth O (2006) Registration completeness in the Norwegian Arthroplasty Register. Acta Orthop 77:49–56
Flamme CH, Ruhmann O, Schmolke S, Wichmann R (2003) Long-term outcome following high tibial osteotomy with tension bend principle. Arch Orthop Trauma Surg 123:12–16
Flecher X, Parratte S, Aubaniac JM, Argenson JN (2006) A 12–28-year followup study of closing wedge high tibial osteotomy. Clin Orthop Relat Res 452:91–96
Frey P, Muller M, Munzinger U (2008) Closing-wedge high tibial osteotomy with a modified Weber technique. Oper Orthop Traumatol 20:75–88
Gall N, Fickert S, Puhl W, Gunther KP, Stove J (2005) Predictors of tibial head transposition in the therapy of varus knee osteoarthritis. Z Orthop Ihre Grenzgeb 143:551–555
Gill T, Schemitsch EH, Brick GW, Thornhill TS (1995) Revision total knee arthroplasty after failed unicompartmental knee arthroplasty or high tibial osteotomy. Clin Orthop Relat Res 321:10–18
Gstottner M, Pedross F, Liebensteiner M, Bach C (2008) Long-term outcome after high tibial osteotomy. Arch Orthop Trauma Surg 128:111–115
Gulati A, Pandit H, Jenkins C, Chau R, Dodd CA, Murray DW (2009) The effect of leg alignment on the outcome of unicompartmental knee replacement. J Bone Joint Surg Br 91:469–474
Ha’eri GB, Wiley AM (1980) High tibial osteotomy combined with joint debridement: a long-term study of results. Clin Orthop Relat Res 151:153–159
Hasegawa Y, Ooishi Y, Shimizu T, Sugiura H, Takahashi S, Ito H, Iwata H (1998) Unicompartmental knee arthroplasty for medial gonarthrosis: 5 to 9 years follow-up evaluation of 77 knees. Arch Orthop Trauma Surg 117:183–187
Hassenpflug J, von Haugwitz A, Hahne HJ (1998) Long-term results of tibial head osteotomy. Z Orthop Ihre Grenzgeb 136:154–161
Heaton KT, Dorr LD (2003) History of knee arthroplasty. In: Callaghan JJ, Rosenberg AG, Rubash HE, Simonian PT, Wickeewicz TL (eds) The adult knee. Lipincott Williams and Wilkins, Philadelphia, pp 15–24
Heck DA, Marmor L, Gibson A, Rougraff BT (1993) Unicompartmental knee arthroplasty. A multicenter investigation with long-term follow-up evaluation. Clin Orthop Relat Res 286:154–159
Hendel D, Beloosesky Y, Garti A, Weisbort M (2003) Medial unicompartmental replacement for tricompartmental disease in the elderly. Knee 10:363–365
Hernigou P, Deschamps G (2004) Posterior slope of the tibial implant and the outcome of unicompartmental knee arthroplasty. J Bone Joint Surg Am 86-A:506–511
Hernigou P, Ma W (2001) Open wedge tibial osteotomy with acrylic bone cement as bone substitute. Knee 8:103–110
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Holden DL, James SL, Larson RL, Slocum DB (1988) Proximal tibial osteotomy in patients who are fifty years old or less. A long-term follow-up study. J Bone Joint Surg Am 70:977–982
Huang TL, Tseng KF, Chen WM, Lin RM, Wu JJ, Chen TH (2005) Preoperative tibiofemoral angle predicts survival of proximal tibia osteotomy. Clin Orthop Relat Res 432:188–195
Insall JN, Dorr LD, Scott RD, Scott WN (1989) Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res 248:13–14
Ivarsson I, Myrnerts R, Gillquist J (1990) High tibial osteotomy for medial osteoarthritis of the knee. A 5 to 7 and 11 year follow-up. J Bone Joint Surg Br 72:238–244
Johnell O, Sernbo I, Gentz CF (1985) Unicompartmental knee replacement in osteoarthritis: an 8-year follow-up. Arch Orthop Trauma Surg 103:371–374
Keblish PA, Briard JL (2004) Mobile-bearing unicompartmental knee arthroplasty: a 2-center study with an 11-year (mean) follow-up. J Arthroplast 19:87–94
Kellgren JH, Lawrence JS (1957) Radiological assessment of osteo-arthrosis. Ann Rheum Dis 16:494–502
Keys GW, Ul-Abiddin Z, Toh EM (2004) Analysis of first forty Oxford medial unicompartmental knee replacement from a small district hospital in UK. Knee 11:375–377
Knutson K, Robertsson O (2010) The Swedish Knee Arthroplasty Register (http://www.knee.se). Acta Orthop 81:5–7
Koshino T, Yoshida T, Ara Y, Saito I, Saito T (2004) Fifteen to twenty-eight years’ follow-up results of high tibial valgus osteotomy for osteoarthritic knee. Knee 11:439–444
Koskinen E, Paavolainen P, Eskelinen A, Pulkkinen P, Remes V (2007) Unicondylar knee replacement for primary osteoarthritis: a prospective follow-up study of 1,819 patients from the Finnish Arthroplasty Register. Acta Orthop 78:128–135
Larsson SE, Larsson S, Lundkvist S (1988) Unicompartmental knee arthroplasty. A prospective consecutive series followed for six to 11 years. Clin Orthop Relat Res 232:174–181
Lysholm J, Gillquist J (1982) Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med 10:150–154
Mackinnon J, Young S, Baily RA (1988) The St Georg sledge for unicompartmental replacement of the knee. A prospective study of 115 cases. J Bone Joint Surg Br 70:217–223
Majima T, Yasuda K, Katsuragi R, Kaneda K (2000) Progression of joint arthrosis 10 to 15 years after high tibial osteotomy. Clin Orthop Relat Res 381:177–184
Malik MH, Chougle A, Pradhan N, Gambhir AK, Porter ML (2005) Primary total knee replacement: a comparison of a nationally agreed guide to best practice and current surgical technique as determined by the North West Regional Arthroplasty Register. Ann R Coll Surg Engl 87:117–122
Maqut P (1963) A biomechanical treatment of femoro-patellar arthrosis: advancement of patellar tendon. Rev Rhum Mal Osteoartic 30:779–783
Marmor L (1988) Unicompartmental arthroplasty of the knee with a minimum ten-year follow-up period. Clin Orthop Relat Res 228:171–177
Matsunaga D, Akizuki S, Takizawa T, Yamazaki I, Kuraishi J (2007) Repair of articular cartilage and clinical outcome after osteotomy with microfracture or abrasion arthroplasty for medial gonarthrosis. Knee 14:465–471
Mercier N, Wimsey S, Saragaglia D (2010) Long-term clinical results of the Oxford medial unicompartmental knee arthroplasty. Int Orthop 34:1137–1143
Murray DW, Goodfellow JW, O’Connor JJ (1998) The Oxford medial unicompartmental arthroplasty: a ten-year survival study. J Bone Joint Surg Br 80:983–989
Nagi ON, Kumar S, Aggarwal S (2007) Combined lateral closing and medial opening-wedge high tibial osteotomy. J Bone Joint Surg Am 89:542–549
Naudie D, Bourne RB, Rorabeck CH, Bourne TJ (1999) The Install Award. Survivorship of the high tibial valgus osteotomy. A 10- to -22-year followup study. Clin Orthop Relat Res 367:18–27
Naudie D, Guerin J, Parker DA, Bourne RB, Rorabeck CH (2004) Medial unicompartmental knee arthroplasty with the Miller-Galante prosthesis. J Bone Joint Surg Am 86-A:1931–1935
Omori G, Koga Y, Miyao M, Takemae T, Sato T, Yamagiwa H (2008) High tibial osteotomy using two threaded pins and figure-of-eight wiring fixation for medial knee osteoarthritis: 14 to 24 years follow-up results. J Orthop Sci 13:39–45
O’Rourke MR, Gardner JJ, Callaghan JJ, Liu SS, Goetz DD, Vittetoe DA, Sullivan PM, Johnston RC (2005) The John Insall Award: unicompartmental knee replacement: a minimum twenty-one-year followup, end-result study. Clin Orthop Relat Res 440:27–37
Papachristou G, Plessas S, Sourlas J, Levidiotis C, Chronopoulos E, Papachristou C (2006) Deterioration of long-term results following high tibial osteotomy in patients under 60 years of age. Int Orthop 30:403–408
Parratte S, Argenson JN, Pearce O, Pauly V, Auquier P, Aubaniac JM (2009) Medial unicompartmental knee replacement in the under-50 s. J Bone Joint Surg Br 91:351–356
Pennington DW, Swienckowski JJ, Lutes WB, Drake GN (2003) Unicompartmental knee arthroplasty in patients sixty years of age or younger. J Bone Joint Surg Am 85-A:1968–1973
Polyzois D, Stavlas P, Polyzois V, Zacharakis N (2006) The oblique high tibial osteotomy technique without bone removal and with rigid blade plate fixation for the treatment of medial osteoarthritis of the varus knee: medium and long-term results. Knee Surg Sports Traumatol Arthrosc 14:940–947
Price AJ, Dodd CA, Svard UG, Murray DW (2005) Oxford medial unicompartmental knee arthroplasty in patients younger and older than 60 years of age. J Bone Joint Surg Br 87:1488–1492
Price AJ, Waite JC, Svard U (2005) Long-term clinical results of the medial Oxford unicompartmental knee arthroplasty. Clin Orthop Relat Res 435:171–180
Ranawat CS, Shine JJ (1973) Duo-condylar total knee arthroplasty. Clin Orthop Relat Res 94:185–195
Ridgeway SR, McAuley JP, Ammeen DJ, Engh GA (2002) The effect of alignment of the knee on the outcome of unicompartmental knee replacement. J Bone Joint Surg Br 84:351–355
Rinonapoli E, Mancini GB, Corvaglia A, Musiello S (1998) Tibial osteotomy for varus gonarthrosis. A 10- to 21-year followup study. Clin Orthop Relat Res 353:185–193
Romanowski MR, Repicci JA (2002) Minimally invasive unicondylar arthroplasty: eight-year follow-up. J Knee Surg 15:17–22
Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD (1998) Knee Injury and Osteoarthritis Outcome Score (KOOS)—development of a self-administered outcome measure. J Orthop Sports Phys Ther 28:88–96
Sasaki T, Yagi T, Monji J, Yasuda K, Tsuge H (1986) High tibial osteotomy combined with anterior displacement of the tibial tubercle for osteoarthritis of the knee. Int Orthop 10:31–40
Schultz W, Gobel D (1999) Articular cartilage regeneration of the knee joint after proximal tibial valgus osteotomy: a prospective study of different intra- and extra-articular operative techniques. Knee Surg Sports Traumatol Arthrosc 7:29–36
Scott RD, Cobb AG, McQueary FG, Thornhill TS (1991) Unicompartmental knee arthroplasty. Eight- to 12-year follow-up evaluation with survivorship analysis. Clin Orthop Relat Res 271:96–100
Sen C, Kocaoglu M, Eralp L (2003) The advantages of circular external fixation used in high tibial osteotomy (average 6 years follow-up). Knee Surg Sports Traumatol Arthrosc 11:139–144
Simonet J, Maquet P, De MP (1963) Biomechanical considerations on arthrosis of the knee. Study of forces. Osteotomy. Rev Rhum Mal Osteoartic 30:777–778
Skyrme AD, Mencia MM, Skinner PW (2002) Early failure of the porous-coated anatomic cemented unicompartmental knee arthroplasty: A 5- to 9-year follow-up study. J Arthroplast 17:201–205
Sprenger TR, Doerzbacher JF (2003) Tibial osteotomy for the treatment of varus gonarthrosis. Survival and failure analysis to twenty-two years. J Bone Joint Surg Am 85-A:469–474
Squire MW, Callaghan JJ, Goetz DD, Sullivan PM, Johnston RC (1999) Unicompartmental knee replacement. A minimum 15 year followup study. Clin Orthop Relat Res 367:61–72
Steele RG, Hutabarat S, Evans RL, Ackroyd CE, Newman JH (2006) Survivorship of the St Georg Sled medial unicompartmental knee replacement beyond ten years. J Bone Joint Surg Br 88:1164–1168
Sterett WI, Steadman JR, Huang MJ, Matheny LM, Briggs KK (2010) Chondral resurfacing and high tibial osteotomy in the varus knee: survivorship analysis. Am J Sports Med 38:1420–1424
Stewart HD, Newton G (1992) Long-term results of the Manchester knee. Surface arthroplasty of the tibiofemoral joint. Clin Orthop Relat Res 278:138–146
Stockelman RE, Pohl KP (1991) The long-term efficacy of unicompartmental arthroplasty of the knee. Clin Orthop Relat Res 271:88–95
Stukenborg-Colsman C, Wirth CJ, Lazovic D, Wefer A (2001) High tibial osteotomy versus unicompartmental joint replacement in unicompartmental knee joint osteoarthritis: 7–10-year follow-up prospective randomised study. Knee 8:187–194
Svard UC, Price AJ (2001) Oxford medial unicompartmental knee arthroplasty. A survival analysis of an independent series. J Bone Joint Surg Br 83:191–194
Tabor OB Jr, Tabor OB (1998) Unicompartmental arthroplasty: a long-term follow-up study. J Arthroplast 13:373–379
Takai S, Yoshino N, Hirasawa Y (1997) Revision total knee arthroplasty after failed high tibial osteotomy. Bull Hosp Jt Dis 56:245–250
Tang WC, Henderson IJ (2005) High tibial osteotomy: long term survival analysis and patients’ perspective. Knee 12:410–413
Tateishi H, Maruoka T, Yoh K, Iwata Y, Futani H, Yamada H, Maruo S (1991) A long-term follow-up study of unicompartmental replacement with a Marmor knee prosthesis and the introduction of a new ceramic prosthesis. Bull Hosp Jt Dis Orthop Inst 51:132–139
Trieb K, Cetin E, Stulnig T, Wanivenhaus A (2003) Long-term results after uni- and bilateral high tibial osteotomies. Z Orthop Ihre Grenzgeb 141:33–36
Vainionpaa S, Laike E, Kirves P, Tiusanen P (1981) Tibial osteotomy for osteoarthritis of the knee. A five to ten-year follow-up study. J Bone Joint Surg Am 63:938–946
van Raaij T, Reijman M, Brouwer RW, Jakma TS, Verhaar JN (2008) Survival of closing-wedge high tibial osteotomy: good outcome in men with low-grade osteoarthritis after 10–16 years. Acta Orthop 79:230–234
Vorlat P, Putzeys G, Cottenie D, Van IT, Pouliart N, Handelberg F, Casteleyn PP, Gheysen F, Verdonk R (2006) The Oxford unicompartmental knee prosthesis: an independent 10-year survival analysis. Knee Surg Sports Traumatol Arthrosc 14:40–45
Wada M, Imura S, Nagatani K, Baba H, Shimada S, Sasaki S (1998) Relationship between gait and clinical results after high tibial osteotomy. Clin Orthop Relat Res 354:180–188
Weale AE, Murray DW, Crawford R, Psychoyios V, Bonomo A, Howell G, O’Connor J, Goodfellow JW (1999) Does arthritis progress in the retained compartments after ‘Oxford’ medial unicompartmental arthroplasty? A clinical and radiological study with a minimum ten-year follow-up. J Bone Joint Surg Br 81:783–789
Yasuda K, Majima T, Tsuchida T, Kaneda K (1992) A ten- to 15-year follow-up observation of high tibial osteotomy in medial compartment osteoarthrosis. Clin Orthop Relat Res 282:186–195
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Spahn, G., Hofmann, G.O., von Engelhardt, L.V. et al. The impact of a high tibial valgus osteotomy and unicondylar medial arthroplasty on the treatment for knee osteoarthritis: a meta-analysis. Knee Surg Sports Traumatol Arthrosc 21, 96–112 (2013). https://doi.org/10.1007/s00167-011-1751-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-011-1751-2