
Abstract
Purpose
This study was undertaken to evaluate the incidence of bifurcated distal biceps tendons and the tendon’s insertional footprint on the radial tuberosity.
Methods
Twenty-five embalmed cadaveric specimens were dissected. The relationships and orientation of the muscle bellies and distal biceps tendon were examined. The insertional length, width, and footprint area of the distal biceps tendon on the radial tuberosity were evaluated.
Results
In 12 specimens (48%), the distal biceps tendon was in 2 distinct, easily separated parts. The average footprint length, width, and area of the tendon’s insertion on the radial tuberosity were 20.5 mm ± 2.0 mm, 9.7 mm ± 1.3 mm, and 156.3 mm2 ± 29.4 mm2, respectively. We calculated that the tendon’s insertion occupied approximately 35.9% of the area of the radial tuberosity. In the specimens with a bifurcated distal biceps tendon, the long head of the tendon inserted at the posterosuperior portion of the radial tuberosity, and the average area was 71.4 mm2 ± 11.3 mm2. The short head of the distal biceps tendon inserted at the anteroinferior portion, and the average area was 88.3 mm2 ± 24.1 mm2.
Conclusion
This study confirmed that bifurcated distal biceps tendon insertion is not a rare anatomical variation, showed by recent investigations, and found that the short head of the distal biceps tendon was inserted more anteriorly than the long head on the radial tuberosity. These findings may allow functional independence and isolated rupture of each portion. It can make correct diagnosis possible and allow for a more anatomical orientation of the tendon during surgical repair.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
As interest in distal biceps repair has grown, and new techniques for repair have been developed; there has been an increased emphasis on the quantitative and functional anatomy of the distal biceps tendon [11, 13, 14]. A precise understanding of the anatomy of the distal biceps tendon and its relationship to the radial tuberosity is crucial to the successful surgical repair of a ruptured tendon [5, 15, 19, 21]. However, anatomy textbooks provide an ambiguous description of the tendon’s insertion onto the radial tuberosity, and the detailed anatomy of the distal biceps muscle and tendon and its relationship to the radial tuberosity have received little attention. Recent reports have provided details of the anatomy of the distal biceps tendon and have described the shape and size of the footprint of the tendon’s insertion [1, 4, 6, 7, 9, 12, 17, 18]. They have also demonstrated that in some individuals, the tendon may be bifurcated. Several authors have reported isolated rupture of a bifurcated distal biceps tendon [6, 16, 20, 22].
The aim of the present study was to evaluate the incidence of bifurcated distal biceps tendons and its insertional footprint on the radial tuberosity. This study was conducted based on the hypothesis that bifurcated distal biceps tendon insertion is not a rare anatomical variation.
Materials and methods
After obtaining approval from our institutional review board, we dissected 25 embalmed cadaveric specimens under loupe magnification. All specimens were from Koreans; 14 specimens were from men and 11 were from women. The median age of each person at death was 68.7 years (range 45–89 years). The long and short heads of the biceps muscle were detached from their origins and dissected toward its insertion. The proximal radius was then removed en bloc with the biceps muscle. All soft tissue, except for the distal half of the biceps muscle belly and its tendon, was removed.
The relationships and orientation of the muscle bellies and the distal biceps tendon in each specimen were examined. We made note of the dimensions of the tendon insertion and the radial tuberosity, along with the orientation of the insertion and additional features of the radial tuberosity. The distance between the articular margin of the radial head and the upper margin of the radial tuberosity, the length and width of the radial tuberosity, the insertional length, and the width of the distal biceps tendon on the radial tuberosity were measured using calipers with a sensitivity of 0.1 mm. The area of the radial tuberosity and the insertional footprint area of the distal biceps tendon were also measured by using an acetate grid sheet and counting the number of 1 × 1 mm2 occupied by the marked area. To minimize intraobserver and interobserver variations and maximize accuracy, each measurement was repeated 3 times by 2 observers blinded to each other’s results.
Results
Gross findings
In 12 (48%) of 25 specimens, the distal biceps tendon was in 2 distinct and easily separated parts. Each muscle continued as a separated tendon distally. The long head of the distal biceps tendon continued on the radial side of the short head and passed deep to the short head to insert more superiorly on the radial tuberosity. The bicipital aponeurosis was found to originate from the proximal aspect of the short head of the distal tendon in the specimens with a bifurcated distal biceps tendon (Fig. 1).

In this specimen, the long head (white arrow) of the distal biceps tendon continues on the radial side of the short head (black arrow) and passes deep to the short head. The bicipital aponeurosis (asterisk) originates from the proximal aspect of the short head of the distal biceps tendon
The remaining 13 specimens (52%) had interdigitation of the muscle bellies and a completely united distal tendon. In all elbows, the biceps tendon twisted externally distal to the bicipital aponeurosis, and the insertion of the distal biceps tendon was located on the posterior rim of the radial tuberosity. Its configuration was semilunar, with concavity of the anterior surface of the footprint on the radial tuberosity (Fig. 2). The bicipital aponeurosis originated from the proximal aspect of the united distal tendon as it passed anterior to the elbow joint and expands medially, blending with the fascia of the forearm.

In this specimen, (a) interdigitation of the biceps muscle bellies and a completely united distal tendon are apparent, and (b) the insertion of the distal biceps tendon is located on the posterior rim of the radial tuberosity in a semilunar configuration
Measurements
The average distance from the articular margin of the radial head to the upper margin of the radial tuberosity was 19.5 mm ± 2.7 mm. The average length, width, and area of radial tuberosity were 25.5 mm ± 2.3 mm, 14.4 mm ± 1.3 mm, and 435.8 mm2 ± 84.6 mm2, respectively. In all specimens, the average footprint length, width, and area of the distal biceps tendon insertion on the radial tuberosity were 20.5 mm ± 2.0 mm, 9.7 mm ± 1.3 mm, and 156.3 mm2 ± 29.4 mm2, respectively (Table 1). On the basis of the dimensions of the tuberosity, the tendon insertion occupied approximately 80.4% of the length, 67.4% of the width, and 35.9% of the area of the radial tuberosity.
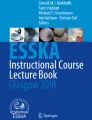
In 12 specimens, the exact dimensions and the area of the short- and long-head tendon insertions could be measured. The long head of the distal biceps tendon inserted at the posterosuperior portion of the radial tuberosity; the average length, width, and area of the long-head tendon insertion were 9.3 mm ± 1.4 mm, 8.4 mm ± 1.3 mm, and 71.4 mm2 ± 11.3 mm2, respectively. The short head biceps tendon inserted at its anteroinferior portion; the average length, width, and area of the short-head tendon insertion were 11.9 mm ± 1.4 mm, 9.1 mm ± 1.7 mm, and 88.3 mm2 ± 24.1 mm2, respectively (Fig. 3; Table 2).

In this specimen, (a) the distal biceps tendon has 2 distinct, bifurcated parts, (b) with the long head of the tendon inserting at the posterosuperior portion and the short head inserting at the anteroinferior portion of the radial tuberosity
Discussion
The most important finding of the present study was that there are 2 independent muscle bellies with a bifurcated distal biceps tendon in a significant proportion (48%) of specimens that confirms findings in another studies, and the short head of the distal biceps tendon was inserted more anteriorly than the long head onto the footprint of the radial tuberosity.
The most common injury to the distal biceps tendon is a complete tear at the insertion site of the radial tuberosity [3, 5, 15]. However, partial tears are being increasingly diagnosed with the use of ultrasound and magnetic resonance imaging [2, 6, 8, 10, 14, 22]. Most anatomical descriptions have suggested that 2 proximal heads of the biceps muscle coalesce into a single distal tendon inserting on the radial tuberosity [1, 7, 17]. As interest in distal biceps repair has grown, the concept of the distal biceps tendon as a simple cylindrical tendon has been challenged. More details about the tendon’s insertion have been revealed in recent years [1, 4, 6, 7, 9, 12, 17, 18, 22].
Several cadaveric and radiologic studies have shown the incidence of bifurcated distal biceps tendons to be anywhere between 11.8 and 58.8% [1, 4, 6, 7, 17, 22]. Athwal et al. [1] reported complete separation of the muscle bellies and distal biceps tendon in 2 (13.3%) of 15 specimens. Eames et al. [7] reported that in 10 (58.8%) of 17 specimens, the distal biceps tendon was in 2 distinct parts, each a continuation of the long head and short head of the muscle. Dirim et al. [6] reported that on visual inspection, confirmed by correlative magnetic resonance images and histology, 2 (25%) of 8 specimens had 2 separate muscle bellies that continued distally as individual tendons. In that group’s magnetic imaging study, the distal biceps tendon appeared bifurcated in 8 (11.8%) of the 68 elbows that had a distal biceps tendon injury. Tagliafico et al. [22] also demonstrated the ultrasound appearance of the distal biceps tendon separation in normal cadavers and volunteers and in those affected by various disease processes. Also, isolated ruptures of a bifurcated distal biceps tendon were recently reported by several authors [6, 16, 20, 22]. Sassmannshausen et al. [20] reported a case of a bifurcated distal biceps tendon with selective disruption of a short-head bundle that was surgically confirmed. This study was the first clinical report that the possibility of a bifurcated distal biceps tendon. Koulouris et al. [16] also reported 2 cases of isolated short-head bundle rupture of a bifurcated distal biceps tendon. They suggested that accurate preoperative detection is paramount because this injury may be confused with a partial-thickness tear of a nonbifurcated distal biceps tendon or a distal musculotendinous junction strain, both which are typically treated conservatively, if the clinical scenario demands surgical restoration because of functional disability.
The present study demonstrated that the distal biceps tendon was in 2 distinct, easily separated parts and each muscle continued as a separated tendon distally in 12 (48%) of 25 specimens. From our observations, it can be inferred as other studies [6, 16, 20, 22] that isolated ruptures of bifurcated distal biceps tendons have been misdiagnosed as partial-thickness or full-thickness tears. Therefore, we suggest that awareness of the existence and anatomy of bifurcated tendons is important so that surgeons can correctly diagnose injuries to tendon components.
The variation in length, width, area, and shape of distal biceps footprints and radial tuberosities may be important in anatomical restoration of the distal biceps tendon. The radial tuberosity and distal biceps insertion footprint are critical structures affecting forearm supination mechanics, and anatomical repair of a ruptured tendon is necessary for restoration of power, endurance, and terminal forearm rotation [11]. The supination torque of the biceps is related to its insertion site on the radial tuberosity [7, 11, 13]. Several authors have reported significant loss of supination range and strength after distal biceps tendon repair with an anteriorly located footprint on the radial tuberosity and have noted that a posteriorly located footprint repair is important for restoration of supination torque [7, 11–13].
In all specimens of the present study, the average footprint area of the distal biceps tendon insertion on the radial tuberosity was 156.3 mm2, and it occupied approximately 35.9% of the area of the radial tuberosity. The distal biceps tendon was inserted on the posterior rim of the radial tuberosity. Its configuration was semilunar, with a concavity of the anterior surface of the footprint on the radial tuberosity. Knowledge of the size and location of the normal footprint can assist surgeons during surgical repair of distal biceps tendon ruptures. Familiarity with the normal footprint dimensions can assist with correct suture-anchor and bone-trough placement. Anatomical repair and restoration of the native footprint will maximize clinical outcomes.
As the long-head tendon inserts onto the radial tuberosity proximally and is furthest from the axis of rotation of the radius, it is thought to provide a more stable lever arm for supination. The distal insertion of the short-head tendon, situated further distally, allows for increased power during elbow flexion [1, 7, 16].
In 12 specimens with a bifurcated distal biceps tendon, the long-head tendon inserted at the posterosuperior portion of the radial tuberosity, and the average insertional area was 71.4 mm2. The short-head tendon inserted at its anteroinferior portion, and the average insertional area was 88.3 mm2. The short head of the distal biceps tendon was inserted more anteriorly than the long head on the radial tuberosity. In this point, the current study is differing from previous studies [1, 7, 16]. There is evidence that posterosuperior insertion of the long-head tendon allows to act as forearm supinator and anteroinferior insertion of the short-head tendon allows to act as elbow flexor. These findings suggest that bifurcated distal biceps tendon insertion may allow functional independence as well as isolated rupture of each portion.
In the specimen with an united distal biceps tendon, the bicipital aponeurosis originated from the proximal aspect of the united distal tendon as it passed anterior to the elbow joint and expands medially, blending with the fascia of the forearm. But it originated from the proximal aspect of the short head of the distal tendon in the specimens with a bifurcated distal biceps tendon. Our findings are concordant with those of recent investigations [1, 6, 9]. Tagliafico el al. [22] emphasized that there is an important difference between patients with isolated short-head-component rupture and those with long-head-component rupture: The former did not present with retraction of the muscle belly, whereas the latter presented the typical Popeye sign, mimicking a complete rupture. It is possible that the contiguity of the short head with the bicipital aponeurosis prevented retraction of the muscle belly.
Limitations of this study include the small sample size, the use of embalmed cadaveric specimens, and the lack of consideration of demographic information, such as height, weight, and hand dominance. Furthermore, there was no biomechanical or histological investigation.
The present study provided more precise anatomical data on the dimensions and orientation of distal biceps tendon insertion on the radial tuberosity, including sex-related differences. The existence of 2 individual muscle bellies and a bifurcated distal biceps tendon has not been widely accepted yet, and its clinical implications are yet to be determined. However, the information that we have presented may serve as a baseline for developing techniques to enable anatomical restoration of the footprint in ruptures of the distal biceps tendon.
Conclusion
This study confirmed that bifurcated distal biceps tendon insertion is not a rare anatomical variation, showed by recent investigations, and found that the short head of the distal biceps tendon was inserted more anteriorly than the long head on the radial tuberosity. These findings may allow functional independence and isolated rupture of each portion. It can make correct diagnosis possible and allow for a more anatomical orientation of the tendon during surgical repair.
References
Athwal GS, Steinmann SP, Rispoli DM (2007) The distal biceps tendon: footprint and relevant clinical anatomy. J Hand Surg Am 32:1225–1229
Belli P, Costantini M, Mirk P, Leone A, Pastore G, Marano P (2001) Sonographic diagnosis of distal biceps tendon rupture: a prospective study of 25 cases. J Ultrasound Med 20:587–595
Bell RH, Wiley WB, Noble JS, Kuczynski DJ (2000) Repair of distal biceps brachii tendon ruptures. J Should Elb Surg 9:223–226
Cucca YY, McLay SV, Okamoto T, Ecker J, McMenamin PG (2010) The biceps brachii muscle and its distal insertion: observations of surgical and evolutionary relevance. Surg Radiol Anat 32:371–375
Davis WM, Yassine Z (1956) An etiological factor in tear of the distal tendon of the biceps brachii: report of two cases. J Bone Jt Surg Am 3:1365–1368
Dirim B, Brouha SS, Pretterklieber ML, Wolff KS, Frank A, Pathria MN, Chung CB (2008) Terminal bifurcation of the biceps brachii muscle and tendon: anatomic considerations and clinical implications. AJR Am J Roentgenol 191:245–255
Eames MH, Bain GI, Fogg QA, van Riet RP (2007) Distal biceps tendon anatomy: a cadaveric study. J Bone Jt Surg Am 89:1044–1049
Festa A, Mulieri PJ, Newman JS, Spitz DJ, Leslie BM (2010) Effectiveness of magnetic resonance imaging in detecting partial and complete distal biceps tendon rupture. J Hand Surg Am 35:77–83
Forthman CL, Zimmerman RM, Sullivan MJ, Gabel GT (2008) Cross-sectional anatomy of the bicipital tuberosity and biceps brachii tendon insertion: relevance to anatomic tendon repair. J Should Elb Surg 17:522–526
Frazier MS, Boardman MJ, Westland M, Imbriglia JE (2010) Surgical treatment of partial distal biceps tendon ruptures. J Hand Surg Am 35:1111–1114
Henry J, Feinblatt J, Kaeding CC, Latshaw J, Litsky A, Sibel R, Stephens JA, Jones GL (2007) Biomechanical analysis of distal biceps tendon repair methods. Am J Sports Med 35:1950–1954
Hutchinson HL, Gloystein D, Gillespie M (2008) Distal biceps tendon insertion: an anatomic study. J Should Elb Surg 17:342–346
Jobin CM, Kippe MA, Gardner TR, Levine WN, Ahmad CS (2009) Distal biceps tendon repair: a cadaveric analysis of suture anchor and interference screw restoration of the anatomic footprint. Am J Sports Med 37:2214–2221
Kelly EW, Steinmann S, O’Driscoll SW (2003) Surgical treatment of partial distal biceps tendon ruptures through a single posterior incision. J Should Elb Surg 12:456–461
Koch S, Tillmann B (1995) The distal tendon of the biceps brachii. Structure and clinical correlations. Ann Anat 177:467–474
Koulouris G, Malone W, Omar IM, Gopez AG, Wright W, Kavanagh EC (2009) Bifid insertion of the distal biceps tendon with isolated rupture: magnetic resonance findings. J Should Elb Surg 18:e22–e25
Kulshreshtha R, Singh R, Sinha J, Hall S (2006) Anatomy of the distal biceps brachii tendon and its clinical relevance. Clin Orthop Relat Res 456:117–120
Mazzocca AD, Cohen M, Berkson E, Nicholson G, Carofino BC, Arciero R, Romeo AA (2007) The anatomy of the bicipital tuberosity and distal biceps tendon. J Should Elb Surg 16:122–127
Morrey BF, Askew LJ, An KN, Dobyns JH (1985) Rupture of the distal tendon of the biceps brachii. A biomechanical study. J Bone Jt Surg Am 67:418–421
Sassmannshausen G, Mair SD, Blazar PE (2004) Rupture of a bifurcated distal biceps tendon. A case report. J Bone Jt Surg Am 86:2737–2740
Seiler JG III, Parker LM, Chamberland PD, Sherbourne GM, Carpenter WA (1995) The distal biceps tendon. Two potential mechanisms involved in its rupture: arterial supply and mechanical impingement. J Should Elb Surg 4:149–156
Tagliafico A, Michaud J, Capaccio E, Derchi LE, Martinoli C (2010) Ultrasound demonstration of distal biceps tendon bifurcation: normal and abnormal findings. Eur Radiol 20:202–208
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cho, CH., Song, KS., Choi, IJ. et al. Insertional anatomy and clinical relevance of the distal biceps tendon. Knee Surg Sports Traumatol Arthrosc 19, 1930–1935 (2011). https://doi.org/10.1007/s00167-011-1586-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-011-1586-x