
Abstract
Purpose
To compare the outcomes of arthroscopic ACL reconstruction procedure in 20 middle-aged patients (12 men and 8 women) and 20 subjects younger than 30 years (control group) at a minimum post-operative follow-up of 24 months.
Methods
Pre- and post-operative anterior–posterior laxity was assessed by Lachman test, pivot shift test and KT1000 arthrometer at manual maximum stress. Clinical functional evaluation was assessed according to IKDC Committee (IKDC) subjective knee form, IKDC ligament standard evaluation and Lysholm score.
Results
At 2 years, all variables significantly improved in both groups compared to pre-operative values (P < 0.05), with non-significant intergroup difference.
Conclusions
When faced with ACL deficiency, physiological age, condition of the knee at the time of examination, life expectancy and activity level are probably more important than chronologic age. In the present study, arthroscopic surgery for the management of ACL tear and secondary lesions provides comparable clinical outcomes in middle-aged patients and in patients aged below 30.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The yearly incidence of anterior cruciate ligament (ACL) tears in the United States is about 200,000, with at least 50% of these patients undergoing arthroscopic reconstruction [14]. Although this procedure may reduce the progression of knee osteoarthritis in chronic ACL deficiency [19, 20], the management of knee instability in middle-aged patients is debated. While satisfactory functional outcomes have been reported in patients older than 50 undergoing conservative management [10], at long-term follow-up, reduction in recreational activity level and increased chronic instability have been reported, with good results reported in middle-aged ACL-reconstructed patients with high functional activity level [11].
In the present study, the surgical management for ACL deficiency has been hypothesized to be indicated in healthy subjects older than 50 years to prevent further secondary injuries and to return to pre-injury sport activity performance status. Additionally, comparing pre- and post-operative status, it was hypothesized that patients over 50 who underwent reconstruction of their ACL experience improved post-operative clinical outcomes. For this purpose, the outcomes of 20 middle-aged patients and 20 subjects younger than 30 years (control group) were compared. All patients underwent arthroscopic ACL reconstruction for ACL deficiency and secondary lesions management.
Materials and methods
Patients were included in the study if they were physically active and had been diagnosed with symptomatic ACL deficiency unresponsive to conservative management detected on clinical grounds (positive Lachman and pivot shift tests, KT1000 arthrometer side-to-side anteroposterior displacement difference more than 3 mm) and magnetic resonance imaging. Diagnostic criteria also included a history of activity-related pain and restricted range of motion. Patients requiring surgical management of associated lesions (menisci, cartilage) were also included in the study.
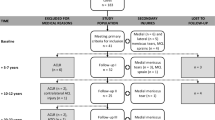
Exclusion criteria included history of previous surgery on either knee, detection of severe osteoarthritic changes (joint space narrowing of more than 50% in any compartment), multi-ligament involvement (posterior cruciate ligament, lateral collateral ligament, medial collateral ligament, posterolateral corner), concomitant lower extremity fracture, cardiovascular disease, workers’ compensation claims or psychiatric illness. Seven active patients diagnosed for combined ACL deficiency and grade II–III valgus laxity were excluded. Finally, a group of 20 consecutive middle-aged patients (ACL over 50 group) who underwent ACL reconstruction between 2004 and 2007 met our inclusion criteria.
The patients were matched for gender and ACL reconstruction technique with a group of 20 subjects younger than 30 years (ACL under 30 group). Twelve men and 8 women were enrolled in both groups. The median age of the patients at presentation was 56 years (50–62) for the ACL over 50 group and 27 years (17–30) for the ACL under 30 group.
Lateral and anteroposterior (AP) weight-bearing radiographs were taken to exclude fractures, for osteoarthritis grading and varus–valgus malalignment assessment. MRI was routinely performed to evaluate lesions to the ACL, cartilage, menisci and other ligaments of the knee.
One author (RP) not involved in the surgical procedure performed all the outcome assessments. The pre- and post-operative anterior–posterior laxity was examined by Lachman test [28], pivot shift test [13] and KT1000 (MEDmetric Corp, San Diego, CA) arthrometer at manual maximum stress [12]. The Lachman and pivot shift measures were graded according to IKDC form [16].
Pre- and post-operative clinical function was assessed according to IKDC Committee (IKDC) subjective knee form, IKDC ligament standard evaluation [16] and Lysholm score [27]. The status of the articular cartilage was graded according to Outerbridge classification [9]. The IKDC activity levels were also determined to evaluate the return to pre-injury sport level activity [16].
Operative findings and rehabilitation
All patients were operated on by one experienced orthopaedic surgeon (L.O.) and underwent a routine ACL reconstruction in a trans-tibial technique [11].
At surgery, all 40 patients were found to have complete tears of their ACL. In the ACL over 50 group, of 11 meniscal-injured patients, 10 underwent partial meniscectomies (7 medial and 3 lateral) and 1 received medial meniscus repair for a red–red zone tear. In the ACL under 30 group, 6 patients underwent partial meniscectomies (3 medial and 3 lateral) and 2 a meniscal repair, one for a red-red zone and one for a white-red zone tear.
The list of patients with cartilage lesions is reported in detail in Table 1. While Outerbridge grade 1–2 cartilage lesions were debrided using a radiofrequency ablation device (Arthrocare, Arthrex, Naples, FL, USA), Outerbridge grade 3–4 cartilage lesions were treated using microfractures according to Steadman technique [26].
In both groups, the patients were allowed partial progressive weight bearing with crutches during the first 4 weeks. The patients who received microfractures for grade III–IV cartilage lesions were advised to partial weight bear for 6 weeks. All patients were allowed for early full knee extension using a 0° locked brace [18, 24].
Running was permitted 2 months from the procedure, and it was delayed 1 month in patients with associated cartilage lesions (grade III–IV).
Return to sports was allowed no sooner 6 months after the index procedure for both groups.
Statistical analysis
To calculate intra-observer variation, the coefficient of variance of KT1000 measures of both right and left knee was calculated on a single control subject, repeating the measurements twice a day, every day, for 20 days. The subject was a healthy volunteer, without history of knee pathology or trauma in either knee, who did not practise sport over the 3-week period to avoid injuries or exercise-induced laxity. In these experimental conditions, the kappa statistics varied between 0.7 and 0.85. Statistical analysis was performed with the SPSS software package, version 11.0 (SPSS, Chicago, IL). Descriptive statistics were calculated. The results of surgery in the two groups were compared using the Wilcoxon signed rank test for continuous variables (Lysholm score, KT1000) and by using the χ2 test for categorical variables (IKDC, pivot shift). Significance level was set P < 0.05.
Results
The mean interval from injury to surgery was 86 days (SD 28; 95% CI 72–100) for the ACL over 50 group and 84 days (SD 22; 95% CI 74–94) for the ACL under 30 group (P > 0.005).
All the patients (12 men and 8 women in both groups) attended the last follow-up. Although all the patients were participating in recreational or competitive sport, different age-related sport activities were evident in the two groups. The median follow-up in the ACL over 50 group and in the ACL under 30 group was 32 months (range 24–49) and 33 months (range 24–44), respectively, with non-significant intergroup difference.
In the ACL over 50 group, the subjective IKDC scores improved from a median pre-operative score of 46 (30–60) to an average of 91 (80–100) (P < 0.001) at the last follow-up. In the ACL under 30 group, the median pre-operative score of 50 (39–67) improved to 92 (80–100) at most recent follow-up (P < .001).
In the ACL over 50 group and ACL under 30 group, the median pre-operative Lysholm scores were respectively 49 (14–67) and 53 (18–70). At 24-month follow-up, the median post-operative Lysholm scores was 89 (41–100) in the ACL over 50 group and 92 (80–100) in the ACL under 30 group with non-significant intergroup difference. In the ACL over 50 group, a Lysholm score of 41 was reported by a patient who underwent ACL graft revision surgery (Table 2).
At 2-year follow-up, the outcomes of clinical examination regarding the Lachman, pivot shift tests and KT1000 side-to-side difference measures were clearly improved when compared to pre-operative status (Table 3).
At the last follow-up, significantly higher IKDC sport activity level rates were observed in the patients aged below 30. Twelve patients (60%) in the ACL over 50 group and 18 (90%) in the ACL under 30 group returned to pre-injury activity levels (P < 0.05) (Table 4). One patient in both groups did not return to sport; the other patients returned to lower pre-injury sport level.
There were no complications, except for one ACL graft failure in the ACL over 50 group. The patient underwent ACL revision surgery 24 months after the first arthroscopic reconstruction.
Discussion
The most important finding of the present study is that good clinical results in terms of anteroposterior stability, Lysholm and IKDC score have been detected in most of the ACL-reconstructed patients regardless of age, with significant improvements compared to pre-surgery status. Although the management of older patients with ACL insufficiency remains controversial [5, 8, 10], in the last few years, surgical management of ACL deficiency has been advocated regardless of age [3, 15, 22, 30]. While high rates of both functional and clinical satisfactory results have been reported in patients over 50 undergoing ACL surgery [29], there is evidence of high satisfaction accompanied by low grade of clinical outcomes in ACL-deficient patients undergoing conservative management, regardless of age [8, 10] (Table 5).
In the present study, side-to-side KT manual maximum difference–related data measured in both groups were comparable with other studies [5, 6, 17] (Table 5).
In accordance with the literature [5, 11], in this study, 85% of patients of the ACL over 50 group and 90% of the other group achieved excellent or good post-operative IKDC scores, with non-significant difference between the two groups.
Barret et al. [4], comparing pre- and post-operative Tegner activity rating scale scores in patients older than 40 years undergoing ACL reconstruction, not pre-operatively involved in high level of sports, found non-significant differences.
In the present study, the IKDC functional outcomes showed that patients’ activity levels improved significantly at the last follow-up compared to the activity level before ACL reconstruction. A remarkable improvement in the quality of life was noted in the over 50 group: 12 patients (60%) returned to their pre-injury activity level, but 8 (40%) patients had a discrepancy between satisfactory outcomes (IKDC score) and returned to lower pre-injury recreational or sport activity. The patients who did not return to pre-injury recreational sport activity had associated injuries, particularly meniscal tears and cartilage damages. As simultaneous ACL reconstruction and meniscectomies give better outcomes than meniscectomies performed in unstable knees [7], almost all the patients with meniscal tears were arthroscopically managed.
At the last examination, while no symptoms were detected in cartilage-injured patients younger than 30 years undergoing radiofrequency debridement, chondral changes influenced negatively the practice of strenuous sport in patients older than 50 years undergoing microfractures. Steadman et al. [26] showed long-term decreased symptoms (pain) and improved function in 95% of patients younger than 45 years undergoing microfracture technique followed by careful rehabilitation; however, chondral changes exert a negative effect on the results of ACL surgery [11]. The pre-operative mild degeneration at imaging in 8 patients (40%) older than 50 years is a cause for concern. Although long-term stability and symptomatic pain relief are obtained by patients (mean age 30 years) undergoing isolated ACL reconstruction for chronic instability with pre-operatively radiographic evidence of degenerative osteoarthritis [25], ACL deficiency or meniscal injuries change the static and dynamic loadings of the knee, with increased deleterious forces on the cartilage and other joint structures [1].
Despite ACL surgery, age and time from injury to surgery have been considered as risk factors for osteoarthritis [21], these parameters cannot be defined as absolute contraindications to surgical management in middle-aged ACL-deficient patients.
A major strength of the present study is that it reports the experience of a single centre, single surgeon, same technique, same graft, independent examiner, homogeneous group of patients, similar rehabilitation programme and 100% follow-up.
It was difficult to conduct a matched pair study, and it was only possible to match for gender and ACL reconstruction technique a group of 20 consecutive middle-aged patients with a group of 20 subjects younger than 30 years. The observation that the two groups in the present study had age-related exposures to different sport activities could influence the sport activity-related outcomes. Comparing the groups, a lower return to pre-injury sport activity level was evident among the older patients [2], but middle-aged patients reported to be subjectively more pleased with the overall results than the younger. In fact, a given outcome in a patient older than 50 could be unsatisfactory in a patient younger than 30. Obviously, surgical expectations should be tailored to age and level of activity.
We are aware that we did not perform an a priori power analysis. However, ACL tears requiring surgical management in middle-aged individuals are not common, and we did not have enough variables to inform a power analysis. The relatively small sample size limited the statistical power of the study, but we point out that, within these limitations, the results of the present study are scientifically sound. Another bias is that a group of patients with ACL deficiency managed conservatively was not included. However, the chronic instability of these patients did not allow us to perform this kind of treatment. Strict inclusion and exclusion criteria and a larger sample would be needed to make more definite recommendations. Despite these weaknesses, the results of our study were univocal with the numbers of patients treated and, in active patients over 50 with chronic ACL insufficiency, the clinical results of ACL reconstruction are similar to those in a younger population [23, 30].
Conclusions
Age itself is not a contraindication to ACL surgery. When faced with patients with ACL instability, physiological age, condition of the knee at the time of examination, expectancy of life and activity level are probably more important than chronologic age. In addition, ACL reconstruction is indicated to manage ACL-related secondary injury and prevent further lesions.
References
Andriacchi TP, Mundermann A, Smith RL, Alexander EJ, Dyrby CO, Koo S (2004) A framework for the in vivo pathomechanics of osteoarthritis at the knee. Ann Biomed Eng 32:447–457
Arbuthnot JE, Brink RB The role of anterior cruciate ligament reconstruction in the older patients, 55 years or above. Knee Surg Sports Traumatol Arthrosc 18:73–78. doi:10.1007/s00167-009-0864-3
Barber FA, Elrod BF, McGuire DA, Paulos LE (1996) Is an anterior cruciate ligament reconstruction outcome age dependent? Arthroscopy 12:720–725
Barrett G, Stokes D, White M (2005) Anterior cruciate ligament reconstruction in patients older than 40 years: allograft versus autograft patellar tendon. Am J Sports Med 33:1505–1512
Blyth MJ, Gosal HS, Peake WM, Bartlett RJ (2003) Anterior cruciate ligament reconstruction in patients over the age of 50 years: 2- to 8-year follow-up. Knee Surg Sports Traumatol Arthrosc 11:204–211
Brandsson S, Kartus J, Larsson J, Eriksson BI, Karlsson J (2000) A comparison of results in middle-aged and young patients after anterior cruciate ligament reconstruction. Arthroscopy 16:178–182
Burks RT, Metcalf MH, Metcalf RW (1997) Fifteen-year follow-up of arthroscopic partial meniscectomy. Arthroscopy 13:673–679
Buss DD, Min R, Skyhar M, Galinat B, Warren RF, Wickiewicz TL (1995) Nonoperative treatment of acute anterior cruciate ligament injuries in a selected group of patients. Am J Sports Med 23:160–165
Cameron ML, Briggs KK, Steadman JR (2003) Reproducibility and reliability of the outerbridge classification for grading chondral lesions of the knee arthroscopically. Am J Sports Med 31:83–86
Ciccotti MG, Lombardo SJ, Nonweiler B, Pink M (1994) Non-operative treatment of ruptures of the anterior cruciate ligament in middle-aged patients. Results after long-term follow-up. J Bone Joint Surg Am 76:1315–1321
Dahm DL, Wulf CA, Dajani KA, Dobbs RE, Levy BA, Stuart MA (2008) Reconstruction of the anterior cruciate ligament in patients over 50 years. J Bone Joint Surg Br 90:1446–1450
Daniel DM, Malcom LL, Losse G, Stone ML, Sachs R, Burks R (1985) Instrumented measurement of anterior laxity of the knee. J Bone Joint Surg Am 67:720–726
Fetto JF, Marshall JL (1979) Injury to the anterior cruciate ligament producing the pivot-shift sign. J Bone Joint Surg Am 61:710–714
Griffin LY, Agel J, Albohm M (2000) Non contact anterior cruciate ligament injuries: risks factors and prevention strategies. J Am Acad Orthop Surg 8:141–150
Hawkins RJ, Misamore GW, Merritt TR (1986) Followup of the acute nonoperated isolated anterior cruciate ligament tear. Am J Sports Med 14:205–210
Hefti F, Muller W, Jakob RP, Staubli HU (1993) Evaluation of knee ligament injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc 1:226–234
Heier KA, Mack DR, Moseley JB, Paine R, Bocell JR (1997) An analysis of anterior cruciate ligament reconstruction in middle-aged patients. Am J Sports Med 25:527–532
Melegati G, Tornese D, Bandi M, Volpi P, Schonhuber H, Denti M (2003) The role of the rehabilitation brace in restoring knee extension after anterior cruciate ligament reconstruction: a prospective controlled study. Knee Surg Sports Traumatol Arthrosc 11:322–326
Murray MM (2009) Current status and potential of primary ACL repair. Clin Sports Med 28:51–61
Noyes FR, Barber SD, Mangine RE (1991) Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. Am J Sports Med 19:513–518
Oiestad BE, Engebretsen L, Storheim K, Risberg MA (2009) Knee osteoarthritis after anterior cruciate ligament injury: a systematic review. Am J Sports Med 37:1434–1443
Plancher KD, Steadman JR, Briggs KK, Hutton KS (1998) Reconstruction of the anterior cruciate ligament in patients who are at least forty years old. A long-term follow-up and outcome study. J Bone Joint Surg Am 80:184–197
Seng K, Appleby D, Lubowitz JH (2008) Operative versus nonoperative treatment of anterior cruciate ligament rupture in patients aged 40 years or older: an expected-value decision analysis. Arthroscopy 24:914–920
Shelbourne KD, Klootwyk TE, Wilckens JH, De Carlo MS (1995) Ligament stability two to six years after anterior cruciate ligament reconstruction with autogenous patellar tendon graft and participation in accelerated rehabilitation program. Am J Sports Med 23:575–579
Shelbourne KD, Stube KC (1997) Anterior cruciate ligament (ACL)-deficient knee with degenerative arthrosis: treatment with an isolated autogenous patellar tendon ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 5:150–156
Steadman JR, Briggs KK, Rodrigo JJ, Kocher MS, Gill TJ, Rodkey WG (2003) Outcomes of microfracture for traumatic chondral defects of the knee: average 11-year follow-up. Arthroscopy 19:477–484
Tegner Y, Lysholm J (1985) Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 198:43–49
Torg JS, Conrad W, Kalen V (1976) Clinical diagnosis of anterior cruciate ligament instability in the athlete. Am J Sports Med 4:84–93
Trojani C, Sane JC, Coste JS, Boileau P (2009) Four-strand hamstring tendon autograft for ACL reconstruction in patients aged 50 years or older. Orthop Traumatol Surg Res 95:22–27
Viola R, Vianello R (1999) Intra-articular ACL reconstruction in the over-40-year-old patient. Knee Surg Sports Traumatol Arthrosc 7:25–28
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Osti, L., Papalia, R., Del Buono, A. et al. Surgery for ACL deficiency in patients over 50. Knee Surg Sports Traumatol Arthrosc 19, 412–417 (2011). https://doi.org/10.1007/s00167-010-1242-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-010-1242-x