
Abstract
We present a case with an unusual and late cyst development after use of a biogradable femoral transfixation for ACL reconstruction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Graft fixation in ACL surgery has improved over the last decades. Particular the use of close-to-joint fixation with the result of a stiffer graft-fixation complex is thought to improve the postoperative stability. Use of biogradable fixation is often preferred instead of metallic devices [4, 6] to avoid later removal of implants in case of need for revision and because biomaterial does not create artifacts on magnetic resonance imaging (MRI). Complication after use of biogradable material in surgery has been described as pretibial bone resorption and cyst formation [2, 7] and intraarticular migration of broken fixation devices [1, 5]. With this case, we want to shed light on possible development of a cyst caused by a degradable fixation device but not emanated from where it is placed. To our knowledge, there has been no similar report in the literature.
Case report
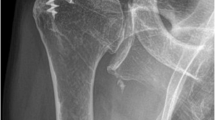
A 19-year-old male college student was 4.5 years ago operated for a ruptured ACL. For femoral fixation of the hamstring graft was a 50-mm Biotransfix©, Arthrex, used, and tibial fixation was secured by a Delta screw©, Arthrex. There were no intra- or postoperative complications. At routine one-year follow-up, the patient described a stable knee, without swelling but an expected discrete anterior knee pain during kneeling and staircase walking. After 1.5 years, the patient was back to his preinjury soccer level. After 4.2 years, the patient started to feel a slightly painful swelling at the medial side of the knee during exercise. At 4.4 years postoperatively, there was a permanent swelling for which he attended the emergency ward. He was found to have a soft, diffusely placed swelling medial and superior at the knee with normal overlying intact skin. The knee was found to have flexion deficit of 30 degrees, but full extension. The patient had no fever, and laboratory test result was without sign of systemic infection. There was no side-to-side difference measured with KT-1000. A radiograph of the knee was taken (Fig. 1). The radiographs revealed soft tissue swelling at the supero-medial side of the knee, and a still visible trace from the transfixation.

Radiograph of the knee indicating a large soft tissue swelling at the medial side superior of the knee and a still visible transfemoral canal
A subsequent MRI revealed a cyst formation originating from a cortical defect of the medial aspect of the femur communicating with a widened tunnel from the inserted transfix system. Furthermore, a solid degradation product from the Biotransfix implant inside the cyst is seen. (Figs. 2 and 3).

MRI of the knee with cyst formation at the medial aspect of the knee, originating from the inserted transfemoral fixation

Cyst formation at medial side of femur. A part of the degraded Biotransfix is seen in the cyst
Two days after the clinical and radiological examination, the cyst penetrated through the skin, and a gelatinous product could be exprimed.
The following day, the patient was scheduled for surgery. At arthroscopic evaluation, an unaffected knee joint and an intact ACL graft was seen. There was no intra-articular sign of the cyst as expected.
An incision posterior to the head of vastus medialis was made, and the cyst was identified and removed. The cyst was filled with gelatinous liquor, and several products with up to a length of 5 mm from the now degraded Transfix pin were found.
A guide pin was placed transfemoral through the tunnel of the former fixation device and a 6-mm drill was used in order to remove remnants from the Transfix pin.
Culture from the cyst material came out negative.
The patient recovered without further swelling and 2 months later was back to his former soccer level.
Discussion
Pretibial cyst formation after ACL reconstruction using both absorbable and non-absorbable fixation material has been described in several case reports [2, 8].
There has been one report of a postoperative cyst formation originating from the femoral site [3]. This was associated with a non-absorbable traction suture left in place at the lateral site of the thigh.
In our case, the cyst formed after more than 4 years at the medial site of the knee despite that the fixation device was inserted from the lateral site. However, a small penetration of the medial femoral cortex is made during placement of the guide wire, before introducing the actual fixation pin.
Inside the cyst, we found several pieces of the degraded and now broken Transfix pin, and based on the history of this patient we believe that the cyst is caused by the degradation products.
Being the first presentation of such a case, it is concluded that this is a very rare complication after the use of bioabsorbable femoral fixation.
References
Baums MH, Zelle BA, Schultz W, Ernstberger T, Klinger H-M (2006) Intraarticular migration of a broken biodegradable interference screw after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Artrosc 14:865–868
Busfeld BT, Anderson LJ (2007) Sterile pretibial abscess after anterior cruciate ligament reconstruction from bioabsorbable interference screws: a report of 2 cases. Arthroscopy 23:911.el–911.e4
Feldmann DD, Fanelli GC (2001) Development of a synovial cyst following anterior cruciate ligament reconstruction. Arthroscopy 17:200–202
McGuire DA, Barber FA, Elrod BF, Paulos LE (1999) Bioabsorbable interference screws for graft fixation in anterior cruciate ligament reconstruction. Arthroscopy 15:463–473
Pelfort X, Monllau JC, Puig LL, Càceres E (2006) Iliotibial band friction syndrome after anterior curciate ligament reconstruction using the transfix device: report of two cases and review of the literature. Knee Surg Sports Traumatol Artrosc 14:586–589
Stähelin AC, Südkamp NP, Weiler A (2001) Anatomic double-bundle posterior cruciate ligament reconstruction using hamstring tendons. Arthroscopy 17:88–97
Tsuda E, Ishibashi Y, Tazawa K, Sato H, Kusumi T, Toh S (2006) Pretibial cyst formation after cruciate ligament reconstruction with hamstring tendon autograft. Arthroscopy 22:691.el–691.e6
Victoroff BN, Paulos L, Beck C, Goodfellow DB (1995) Subcutaneous pretibial cyst formation associated with anterior cruciate ligament allograft: a report of four cases and literature review. Arthroscopy 11:486–494
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Faunø, P., Christiansen, S.E., Lund, B. et al. Cyst formation 4 years after ACL reconstruction caused by biogradable femoral transfixation: a case report. Knee Surg Sports Traumatol Arthrosc 18, 1573–1575 (2010). https://doi.org/10.1007/s00167-010-1182-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-010-1182-5