
Abstract
Intra-articular synovial lipoma is rare and clinically manifested mostly by mass effect and occasionally by torsion of the stalk. Patellar dislocation rarely occurs owing to a mass effect of intra-articular tumor of the knee joint. The authors present a case of large intra-articular synovial lipoma at the lateral gutter of the knee joint, which presents as patellar dislocation. A 19-year-old man visited our clinic due to pain and limitation of motion owing to mass at his left knee. MRI revealed an intra-articular soft tissue mass at the lateral gutter of the knee joint with considerable mass effect displacing patella from the trochlear groove. Excisional biopsy confirmed the diagnosis of lipoma, and the final diagnosis was intra-articular synovial lipoma with clinical information. The final radiograph showed well-aligned patella on the trochlear groove. After marginal excision, there was no recurrence or tumor-related morbidity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Intra-articular synovial lipoma (IASL) is a rare tumorous entity with several case reports [4, 11, 12, 19, 24–27, 31, 34–36]. IASL is clinically manifested mostly by mass effect and occasionally by torsion of the stalk. The etiology of patellar dislocation is multifactorial including osseous or soft tissue abnormalities, and the malalignment of the extensor mechanism is often cited as a major component in dynamic imbalance in patellofemoral articulation [6, 28]. In addition, static mass effect by intra-articular tumor of the knee joint is rarely recognized as an offender in the pathomechanism of patellar dislocation [3]. The authors present a case of large IASL at the lateral gutter of the knee joint, which manifests as patellar dislocation.
Case report
A 19-year-old man visited our clinic due to the left knee discomfort and limitation of motion. He had detected a mass in the lateral aspect of his left knee several years before, which gradually increased over the past years. On physical examination, a non-tender, boggy mass sized 7 cm × 8 cm with soft tissue consistency was palpated on the anterolateral aspect of the knee. The patella was displaced laterally from the trochlear groove. There was no erythema or local heating, and there was no gross instability of the joint. The laboratory blood tests were also negative.
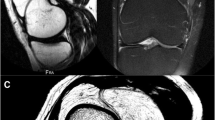
Plain radiographs showed a large soft tissue density on the anterolateral aspect of left knee joint with patellar displacement (Fig. 1). MRI revealed an intra-articular soft tissue mass in the lateral gutter of the knee joint with considerable mass effect displacing patella from the trochlear groove (Fig. 2). With a diagnosis of intra-articular lipoma, operative excision was performed through anterolateral skin incision (Fig. 3). The histopathologic diagnosis was lipoma, and the final diagnosis of intra-articular synovial lipoma was established with clinical information (Fig. 4).

Skyline radiograph of the knee joint showed large soft tissue density on the anterolateral aspect of left knee joint with patellar dislocation from the trochlear groove

Coronal (a) and axial (b) MRI revealed a large soft tissue mass at the lateral gutter of the knee joint displacing patella. The signal intensity of the mass was similar to the subcutaneous fat tissue

The mass was excised through anterolateral longitudinal skin incision (a). The excised mass was 13 cm × 5 cm × 6 cm in size, and the fibrous capsule enclosed mature fat tissue (b)

Microscopic photographs showing mature adipose cells with fibrous septae. There were no lipoblasts or atypical cells. The histopathologic diagnosis was lipoma. (a hematoxylin and eosin, ×20, b hematoxylin and eosin, ×200)
Postoperative rehabilitation was uneventful, and he could participate in any sports activities without any discomfort in the involved knee at postoperative 1 year. The final radiograph showed well-aligned patella on the trochlear groove.
Discussion
The most important finding of the present study was that the rare IASL can pose a considerable mass effect on the patellofemoral articulation and may present as patellar dislocation. IASL could be included as a differential diagnosis in the cause of patellar dislocation.
While lipomas constitute nearly half of all the soft tissue tumors [4, 12, 19], IASL is rarely seen. The etiology of IASL is unknown, and the clinical manifestation usually encompasses mass effect. Symptomatic IASL can be excised by open procedure [19, 25, 34] or arthroscopy [4, 12, 26, 27, 34, 35], and no recurrence or malignant transformation has been reported, although osseous metaplasia was once reported [31]. Clinical symptoms of IASL originate from mechanical causation including interposition of the tumor mass between the articular surfaces and strangulation of the tumor as it strands around its stalk [27, 31]. Catching, interruption of normal motion, snapping, non-tender swelling with or without locking of the joint are usually presented by impingement [4, 11, 12, 24, 26, 27, 34, 36], whereas severe painful swelling with pseudo-locking often accompanies the torsion of the stalk, or volvulus [19, 35]. The current case deserves attention in that the long-standing large mass can elicit overt mass effect that even displaces patella.
IASL should be differentiated from other lipomatoid conditions including lipoma arborescens or Hoffa’s disease [12, 19, 27]. Lipoma arborescens is characterized by ‘villous lipomatous proliferation of the synovial membrane [10] and is considered as a pseudotumor [27]. Macroscopic villous or frond-like appearance of lipoma arborescens also distinguished itself from the small round or oval contour of IASL [11, 21, 32]. Lipoma arborescens is supposed to occur in association with degenerative joint disease, rheumatoid arthritis, diabetes mellitus, gout, psoriasis, or trauma, and often followed by osteoarthritis [1, 10, 12, 15, 17, 20, 21, 27, 32, 33], whereas IASL is supposed to occur de novo without arthritic changes [24, 25]. Absence of degenerative changes in the current case even with the large mass also supported the diagnosis of IASL rather than lipoma arborescens. Both IASL and lipoma arborescens most commonly involve the knee joint. In addition, lipoma arborescens has been reported to occur in glenohumeral joint [5, 17], subdeltoid bursa [7, 29], elbow joint [8, 9, 22], and ankle [2, 14], while only hip [23] and lumbar spine [16] are the only reported loci of IASL other than the knee joint. Hoffa’s disease is a syndrome of infrapatellar fat pad impingement, mostly at the patellofemoral joint, causing anterior knee pain syndrome [13, 18, 30], which is discerned from the current case by the location of origin.
A case of large IASL of the knee joint manifested as patellar dislocation is presented, which deserved the attention of clinicians on the mass effect of the IASL. Elimination of the mass effect by excision of the IASL restored the normal patellar tracking. After marginal excision, there was no recurrence or tumor-related morbidity.
References
Armstrong SJ, Watt I (1989) Lipoma arborescens of the knee. Br J Radiol 62:178–180
Babar SA, Sandison A, Mitchell AW (2008) Synovial and tenosynovial lipoma arborescens of the ankle in an adult: a case report. Skeletal Radiol 37:75–77
Bartlett MJ, Lavelle J (2000) Localized pigmented villonodular synovitis presenting as recurrent dislocation of the patella. Arthroscopy 16:767–769
Bernstein AD, Jazrawi LM, Rose DJ (2001) Arthroscopic treatment of an intra-articular lipoma of the knee joint. Arthroscopy 17:539–541
Chae EY, Chung HW, Shin MJ, Lee SH (2009) Lipoma arborescens of the glenohumeral joint causing bone erosion: MRI features with gadolinium enhancement. Skeletal Radiol 38:815–818
Colvin AC, West RV (2008) Patellar instability. J Bone Joint Surg Am 90:2751–2762
Dawson JS, Dowling F, Preston BJ, Neumann L (1995) Case report: lipoma arborescens of the sub-deltoid bursa. Br J Radiol 68:197–199
Dinauer P, Bojescul JA, Kaplan KJ, Litts C (2002) Bilateral lipoma arborescens of the bicipitoradial bursa. Skeletal Radiol 31:661–665
Doyle AJ, Miller MV, French JG (2002) Lipoma arborescens in the bicipital bursa of the elbow: MRI findings in two cases. Skeletal Radiol 31:656–660
Hallel T, Lew S, Bansal M (1988) Villous lipomatous proliferation of the synovial membrane (lipoma arborescens). J Bone Joint Surg Am 70:264–270
Hill JA, Martin WR 3rd, Milgram JW (1993) Unusual arthroscopic knee lesions: case report of an intra-articular lipoma. J Natl Med Assoc 85:697–699
Hirano K, Deguchi M, Kanamono T (2007) Intra-articular synovial lipoma of the knee joint (located in the lateral recess): a case report and review of the literature. Knee 14:63–67
Hoffa A (1904) The influence of the adipose tissue with regard to the pathology of the knee joint. JAMA 43:795–796
Huang GS, Lee HS, Hsu YC, Kao HW, Lee HH, Chen CY (2006) Tenosynovial lipoma arborescens of the ankle in a child. Skeletal Radiol 35:244–247
Hubscher O, Costanza E, Elsner B (1990) Chronic monoarthritis due to lipoma arborescens. J Rheumatol 17:861–862
Husson JL, Chales G, Lancien G, Pawlotsky Y, Masse A (1987) True intra-articular lipoma of the lumbar spine. Spine (Phila Pa 1976) 12:820–822
In Y, Chun KA, Chang ED, Lee SM (2008) Lipoma arborescens of the glenohumeral joint: a possible cause of osteoarthritis. Knee Surg Sports Traumatol Arthrosc 16:794–796
Jacobson JA, Lenchik L, Ruhoy MK, Schweitzer ME, Resnick D (1997) MR imaging of the infrapatellar fat pad of Hoffa. Radiographics 17:675–691
Keser S, Bayar A, Numanoglu G (2005) An unusual cause for anterior knee pain: strangulated intra-articular lipoma. Knee Surg Sports Traumatol Arthrosc 13:585–588
Kim RS, Song JS, Park SW, Kim L, Park SR, Jung JH, Park W (2004) Lipoma arborescens of the knee. Arthroscopy 20:e95–e99
Kloen P, Keel SB, Chandler HP, Geiger RH, Zarins B, Rosenberg AE (1998) Lipoma arborescens of the knee. J Bone Joint Surg Br 80:298–301
Levadoux M, Gadea J, Flandrin P, Carlos E, Aswad R, Panuel M (2000) Lipoma arborescens of the elbow: a case report. J Hand Surg Am 25:580–584
Margheritini F, Villar RN, Rees D (1998) Intra-articular lipoma of the hip. A case report. Int Orthop 22:328–329
Marui T, Yamamoto T, Kimura T, Akisue T, Nagira K, Nakatani T, Hitora T, Kurosaka M (2002) A true intra-articular lipoma of the knee in a girl. Arthroscopy 18:E24
Matsumoto K, Okabe H, Ishizawa M, Hiraoka S (2001) Intra-articular lipoma of the knee joint. A case report. J Bone Joint Surg Am 83-A:101–105
Mine T, Ihara K, Taguchi T, Tanaka H, Suzuki H, Hashimoto T, Kawai S (2003) Snapping knee caused by intra-articular tumors. Arthroscopy 19:E21
Motsis E, Vasiliadis HS, Xenakis TA (2005) Intraarticular synovial lipoma of the knee located in the intercondylar notch, between ACL and PCL: a case report and review of the literature. Knee Surg Sports Traumatol Arthrosc 13:683–688
Mulford JS, Wakeley CJ, Eldridge JD (2007) Assessment and management of chronic patellofemoral instability. J Bone Joint Surg Br 89:709–716
Nisolle JF, Blouard E, Baudrez V, Boutsen Y, De Cloedt P, Esselinckx W (1999) Subacromial-subdeltoid lipoma arborescens associated with a rotator cuff tear. Skeletal Radiol 28:283–285
Ogilvie-Harris DJ, Giddens J (1994) Hoffa’s disease: arthroscopic resection of the infrapatellar fat pad. Arthroscopy 10:184–187
Pudlowski RM, Gilula LA, Kyriakos M (1979) Intraarticular lipoma with osseous metaplasia: radiographic-pathologic correlation. AJR Am J Roentgenol 132:471–473
Ryu KN, Jaovisidha S, Schweitzer M, Motta AO, Resnick D (1996) MR imaging of lipoma arborescens of the knee joint. AJR Am J Roentgenol 167:1229–1232
Vilanova JC, Barcelo J, Villalon M, Aldoma J, Delgado E, Zapater I (2003) MR imaging of lipoma arborescens and the associated lesions. Skeletal Radiol 32:504–509
Yamaguchi S, Yamamoto T, Matsushima S, Yoshiya S, Matsubara N, Matsumoto T (2003) Solitary intraarticular lipoma causing sudden locking of the knee: a case report and review of the literature. Am J Sports Med 31:297–299
Yeomans NP, Robertson A, Calder SJ (2003) Torsion of an intra-articular lipoma as a cause of pseudo locking of the knee. Arthroscopy 19:E27
Yilmaz E, Karakurt L, Yildirim H, Ozercan R (2007) Intra-articular lipoma causing snapping in the patellofemoral joint. Saudi Med J 28:955–958
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Min, K.D., Yoo, J.H., Song, H.S. et al. A case of intra-articular synovial lipoma of the knee joint causing patellar dislocation. Knee Surg Sports Traumatol Arthrosc 18, 1094–1097 (2010). https://doi.org/10.1007/s00167-009-1005-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-009-1005-8