
Abstract
We report one case of mid-substance injury of the posterior cruciate ligament and two cases of mid-substance injuries of the anterior cruciate ligament in children. Surgical repair with augmentation using the iliotibial band was performed on these patients without the use of transphyseal drill holes. A small strip of the iliotibial band was sutured onto the end of the cruciate ligament stump to augment the remnant. At the most recent follow-up examinations, conducted 5–11 years after surgery, no restriction or discomfort in daily and sport activities was reported, and acceptable levels of function in the injured knees were noted in all patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mid-substance tears of the anterior cruciate ligament (ACL) or posterior cruciate ligament (PCL) in skeletally immature children are rare. Such injuries have been successfully treated in adults by intra-articular reconstruction of the ACL and PCL; however, in children, this treatment strategy is still controversial because of the risk of physeal damage [8]. We report one case of mid-substance PCL injury and two cases of mid-substance ACL injuries in children, including the results of surgical repair with augmentation using strips of the iliotibial band.
Case reports
Case 1 (PCL injury)
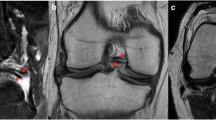
A 6-year-old boy presented to an orthopaedic clinic with a left knee injury following a fall from a tree. PCL injury was suspected, and a cast was applied with his knee in extension. Three days after the accident, he was referred to our clinic for further treatment. Physical examination of his left knee revealed signs of effusion, significant posterior sag, a false-positive anterior drawer sign, and no varus/valgus laxity. The Lachman test was negative, and 5° passive hyperextension of the left knee was observed. Radiographs did not reveal osseous lesions; however, the radiographic posterior drawer test showed obvious posterior laxity of the left knee. The side-to-side difference for the radiographic posterior drawer test was 11 mm. Computed tomography (CT) imaging also did not reveal osseous lesions. Magnetic resonance imaging (MRI) revealed a complete mid-substance tear of the PCL with intact ACL and menisci (Fig. 1) [7]. The boy underwent surgery 2 weeks after injury. Prior to the operation, the patient was encouraged to perform range-of-motion exercises of the left knee.

Magnetic resonance imaging shows a complete mid-substance tear of the posterior cruciate ligament (arrow)
The presence of a 2+ posterior sag was observed under general anaesthesia. Arthroscopy was performed via the standard infrapatellar portals. The ACL, menisci, and articular cartilages of the femoral condyle and tibial plateau were intact. A complete mid-substance tear of the PCL was detected on palpation using a probe. Considering the severe knee posterior laxity and subjective symptoms (completely torn ligament), surgical repair of the PCL tear was recommended. Arthrotomy was performed through a posterior S-shaped skin incision, and the capsule was exposed. The partially torn capsule was incised, and the stump of the PCL was exposed. The PCL was ruptured at a distance of about 10 mm from the tibial attachment, and the remnant stump did not contain any osseous tissue. The femoral end of the ruptured PCL appeared to comprise normal ligamentous tissue; however, this portion could not be attached to the original site of tibial insertion, because its length was insufficient and its distal end was thin. Therefore, a small, 10 × 25 mm strip of the iliotibial band was harvested and sutured onto the distal end of the PCL remnant to augment its length (Fig. 2). Two small (2 mm in diameter) posterioanterior holes were then drilled into the tibial attachment of the PCL. These holes were drilled parallel and proximal to the tibial growth-plate under fluoroscopic guidance, to avoid the danger of growth-plate injury. The augmented PCL remnant was then attached to the tibial insertion site by passing non-absorbable sutures (Ethibond No. 2) through the holes. Then, the sutures were tied together on the anterior aspect of the tibia.

Posterior aspect of the knee in Case 1. A small strip of the iliotibial band (arrow) was sutured onto the distal side of the posterior cruciate remnant to augment the length of the remnant ligament
At a follow-up examination 5 years after the surgery, no restriction or discomfort associated with daily and sport activities was detected. Physical examination of the knee revealed normal range of motion and a slightly positive posterior drawer sign. The follow-up stress radiographs of both knees showed a mild posterior tibial displacement of approximately 5 mm more in the left knee (left) than in the other knee. The side-to-side difference for the radiographic gravity sag was also 5 mm.
Cases 2 and 3 (ACL injuries)
We present two cases of ACL injury: an 11-year-old boy (Case 2) who injured his right knee while playing soccer, and a 5-year-old girl (Case 3) who fell from a swing. On physical examination in both cases, a large effusion in the injured knee was detected and the Lachman test was positive. Radiographic examination of the injured knees did not reveal any osseous lesions. In Case 2, ACL repair was performed 11 days after the accident, whereas in Case 3, it was performed 24 days after the injury. The operative procedures were identical in both cases.
Arthroscopy was performed via the standard infrapatellar portals and it revealed a complete mid-substance tear of the ACL in both cases. Although the ACL remnants at the tibial side appeared to comprise normal ligamentous tissue, their length was insufficient for attachment to the femoral origin. Arthrotomy was performed through a medial parapatellar incision. A small, 10 × 20 mm strip of the iliotibial band was harvested and sutured to the end of the ACL stump (Fig. 3). Thus, sufficient length of the ACL was established. Five sutures (Ethibond No. 2) were placed at the end of the ACL stump and iliotibial band. In Case 2, the sutures were passed through 2 small holes drilled into the femur, whereas in Case 3, they were passed through a hole drilled into the femur, via the over-the-top route. Finally, the sutures were tied together on the lateral femoral epicondyle.

Anterior aspect of the knee in Case 3. A small piece of the iliotibial band was harvested and sutured onto the end of the anterior cruciate ligament stump
The follow-up period was 10 years and 11 years in Cases 2 and 3, respectively. The side-to-side difference in anterior displacement at 133 N was measured after 6 months and then every year after surgery, and was determined by using a KT-2000 knee ligament arthrometer (Med Metric, San Diego, CA, USA). At the most recent follow-up visit, the results were 2.2 mm for Case 2, and 1.2 mm for Case 3. At this time, the pivot shift test was negative and no limitation of knee motion was noted in either case. The repaired ACLs were represented as low-signal-intensity bands in normal size and normal figuration. Both patients returned to a normal level of healthy children’s activities and did not report any giving-way sensation whilst playing with their friends or doing sports activities such as baseball.
Discussion
The principal finding of the present study was that the surgical repair of ACL or PCL acute mid-substance tear injuries in children can correct the severe laxity of injured knees without complications.
ACL or PCL tears in children are often caused by a fracture or physeal injury rather than by ligament disruption, because the resilience and strength of a ligament are greater than those of bones or physes [1, 2].
Several studies on ACL failure in children have shown that there is a higher prevalence of tibial spine avulsion fractures than mid-substance ACL injuries in children who are skeletally immature. Hughston et al. [3] reported avulsions of the femoral site more commonly at 55%, and mid-substance tears at 28%, whereas avulsion fractures located on the tibial site were reported to be less frequent at 17%. Kellenberger and Von Laer [4] showed that mid-substance injury of the ACL was seen in 20% of patients under the age of 12 years. In contrast, mid-substance injury of the PCL is extremely rare in children [1]. To the best of our knowledge, this is the only documented report of surgical treatment for children with mid-substance PCL injury.
We performed surgical repairs in pediatric patients with mid-substance cruciate ligament injuries, without the drilling of transphyseal holes. The clinical results of surgical ligament repair with augmentation using the iliotibial band were found to be favorable. One of the reasons for the success of our method might be attributed to the high potential of tissue remodeling in children. Physeal sparing reconstruction of the cruciate ligament in skeletally immature children can provide a good outcome in the case of chronic ACL tears [5]. In the case of mid-substance injury of the PCL in children, however, the treatment is controversial. Many orthopaedic surgeons may recommend delaying surgical treatment until bone growth in children is complete. Although conservative management for PCL injury was reported in a 6-year-old child, the patient developed anterior knee pain and a partial tear of the medial meniscus 5 years after injury [6]. In addition, restricting the activities of otherwise healthy children for a long period until surgical reconstruction is undesirable in terms of mental health.
The 5 to 11-year follow-up examinations of our patients suggest that the surgical repair of acute ACL or PCL injuries in children can correct the abnormal laxity of severely injured knees, with minimal risk of growth disturbances, and they also suggest that a relatively high functional level can be restored. We advise that surgical repair for young patients with radiographic documentation of wide open growth plates should be performed by a method that does not damage these growth plates.
References
Goodrich A, Ballard A (1988) Posterior cruciate ligament avulsion associated with ipsilateral femur fracture in a 10-year-old child. J Trauma 28:1393–1396. doi:10.1097/00005373-198809000-00016
Hesse E, Bastian L, Zeichen J, Pertschy S, Bosch U, Krettek C (2006) Femoral avulsion fracture of the posterior cruciate ligament in association with a rupture of the popliteal artery in a 9-year-old boy: a case report. Knee Surg Sports Traumatol Arthrosc 14:335–339. doi:10.1007/s00167-005-0677-y
Hughston JC, Bowden JA, Andrews JR, Norwood LA (1980) Acute tears of the posterior cruciate ligament. Results of operative treatment. J Bone Joint Surg Am 62:438–450
Kellenberger R, von Laer L (1990) Nonosseous lesions of the anterior cruciate ligaments in childhood and adolescence. Prog Pediatr Surg 25:123–131
Kocher MS, Garg S, Micheli LJ (2006) Physeal sparing reconstruction of the anterior cruciate ligament in skeletally immature prepubescent children and adolescents. Surgical technique. J Bone Joint Surg Am 88(Suppl 1 Pt 2):283–293. doi:10.2106/JBJS.F.00441
MacDonald PB, Black B, Old J, Dyck M, Davidson M (2003) Posterior cruciate ligament injury and posterolateral instability in a 6-year-old child. A case report. Am J Sports Med 31:135–136
Prince JS, Laor T, Bean JA (2005) MRI of anterior cruciate ligament injuries and associated findings in the pediatric knee: changes with skeletal maturation. AJR Am J Roentgenol 185:756–762
Salter R, Harris W (1963) Injuries involving the epiphyseal plate. J Bone Joint Surg Am 45:587–622
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kongcharoensombat, W., Nakamae, A., Adachi, N. et al. Mid-substance tear of the anterior and posterior cruciate ligaments in children: a report of three patients. Knee Surg Sports Traumatol Arthrosc 17, 964–967 (2009). https://doi.org/10.1007/s00167-009-0806-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-009-0806-0