
Abstract
Oral contraceptive use and menstrual cycle phase are suggested to influence the risk of anterior cruciate ligament (ACL) injuries in female athletes. However, only few data are available for recreational sports. Therefore, female recreational skiers with a non-contact ACL injury and age-matched controls completed a self-reported questionnaire relating to menstrual history, oral contraceptive use and previous knee injuries. Menstrual history data were used to group subjects into either preovulatory or postovulatory phases of menstrual cycle. Our findings suggest that oral contraceptive use did not show any protective effect against ACL injuries nor did self-reported previous knee injuries show any association with ACL injury rate in recreational alpine skiing. Analysis of menstrual history data revealed that recreational skiers in the preovulatory phase were significantly more likely to sustain an ACL injury than were skiers in the postovulatory phase.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Alpine skiing is the most popular winter sport in the Alps. About 8 million recreational skiers visit the Austrian Alps annually, accounting for more than 500 million ski lift transports [10, 11]. The Austrian ski accident survey 2002/2003 showed an overall incidence of alpine ski injuries of 1.30 per 1,000 skier days [12]. The overall incidence rate, also as a result of the introduction of carving skis, has decreased in the last decade [12]. In contrast, severe knee injuries have increased significantly since the early 1970s [8, 21]. Female recreational skiers and competitive female skiers have a twofold greater incidence in knee injuries and a threefold higher risk to sustain an ACL injury than male skiers [8, 12, 24]. The cause of this gender difference may be related to anatomical, neuromuscular and hormonal factors [14]. Regarding hormonal factors, recent studies indicate possible associations of menstrual cycle phase on the ACL-injury risk in female athletes of various sports [1, 3, 4, 7, 19, 20, 23, 25, 26]. Injuries seem to occur more frequently than expected in the preovulatory phase compared to the postovulatory phase [15], but the influence of hormone fluctuations on ACL injury risk seems inconsistent [15, 20, 23]. Additionally, oral contraceptive (OC) use has been suggested to decrease ACL injury rate by stabilizing the hormonal fluctuation over the menstrual cycle. Moller-Nielson and Hammar [18] reported that athletes on OC had a lower injury rate. However, a cause–effect relationship has not been established [22]. To the best of our knowledge, no study has yet investigated the influence of OC use and menstrual cycle phase on the ACL injury risk in recreational female skiers. We hypothesize a modulating influence of hormonal factors on this risk. Therefore, the objective of this study is twofold: (1) to investigate a possible protective effect of oral contraceptive use against ACL injuries in recreational skiers and (2) to compare the frequencies of non-contact ACL injuries in the preovulatory phase with that in the postovulatory phase of the menstrual cycle in recreational skiers.
Materials and methods
This study was conducted as a case–control study of female recreational alpine skiers in the 2006/2007 and 2007/2008 winter seasons in a ski resort in the western part of Austria. The study was performed in conformity with the ethical standards of the 1964 Declaration of Helsinki. Informed consent was obtained from all subjects prior to the beginning of this research.
Subjects
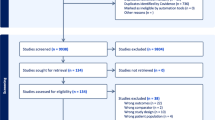
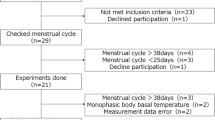
Many of the injured female recreational alpine skiers are treated in a ski clinic, which is located in close proximity to the ski resort studied. Only non-contact ACL injuries were included. MRI was used for the diagnosis of ACL injury. On and off pill users were included. We only recorded frequencies of OC use and not the different types of pills. Subjects were excluded if they were in menopause or used other hormone-stimulating medications. Out of 136 females with non-contact ACL injuries 102 fulfilled the inclusion criteria. Because of some missing data, we were able to classify the menstrual cycle in only 93 patients.
Controls
Uninjured female skiers were randomly selected in the same ski area on five different days over a period of 2 months in the 2007/2008 winter season. Persons were invited to participate in this study as controls. Out of 277 interviewed female skiers, 157 fulfilled the inclusion criteria; 93 controls were randomly matched to the subjects with regard to age.
Questionnaire
We recorded information on age, height, weight and previous knee injuries of either leg for all persons. Injured subjects received and answered the questionnaire within 2 days of the occurrence of injury. We classified self-reported previous knee injuries according to their severity. Only grade II and III injuries to the knee ligaments and injuries of the meniscus and cartilage were attributed to previous knee injuries. Additionally, the phase of menstrual cycle was recorded using a questionnaire developed and validated by Wojtys et al. [25]. This questionnaire included questions on the age at the start of menstruation, date of last menstruation, average length of menstruation and the use of OC.
The menstrual cycle was divided into preovulatory and postovulatory phases according to other studies [7, 15]. We assumed that the postovulatory (luteal) phase of menstrual cycle is constant in length (14 days) regardless of the different length (21–36 days) of menstrual cycle in women. For example, for a 21-day cycle the split would be 7/14 (preovulatory/postovulatory) and for a 32-day cycle the split would be 18/14. Knowing the date of the last menses and the average length of an individual cycle, we could allocate the date of the injury into preovulatory or postovulatory phase of the menstrual cycle.
Statistical analysis
Power analysis based on the results of Beynnon et al. [7] revealed a 90% power for the used sample size. In addition, Hewett et al. [15] revealed in their review article that for 90% power the number of subjects must have been at least 48. Unpaired t tests and Mann–Withney U test, as appropriate, were used to compare subjects and controls with regard to age, height, weight, age at onset of menses and mean length of menstrual cycle. χ2 tests were used to assess different frequencies between groups with regard to previous knee injuries, oral contraceptive use and phase of menstrual cycle. All P values were two-tailed and values less than 0.05 were considered to indicate statistical significance.
Results
A total of 93 female recreational skiers with a non-contact ACL injury and 93 age matched controls participated in this study. Persons in the ACL-injured and control groups did not differ significantly in age, height and weight. Both groups were similar with regard to the age of onset of menstruation and mean length of their menstrual cycle (Table 1).
χ2 tests (Table 2) showed no differences between subjects and controls with regard to previous knee injuries and oral contraceptive use. A reinjury of the same knee was seen in 9.4% of subjects.
Analysis of the menstrual history data indicated a statistical difference between phases in the combined group (P < 0.03). Of the ACL-injured skiers, 57% were in the preovulatory phase at the time of injury, whereas 41% of the controls were in the preovulatory phase at the time of questioning (Table 2). An odds ratio of 1.92 (CI: 1.07–3.44) was calculated.
Regarding subjects and controls without OC use, only a trend (P = .084) toward a 1.88 (CI: 0.92–3.88) increase in ACL injuries in the preovulatory phase was detected.
Discussion
The principal findings of the present study were that OC use showed no protective effect against ACL injuries, while the preovulatory phase is associated with a twofold elevated ACL injury risk. To our knowledge, only one study investigated the ACL-injury risk related to menstrual cycle phase in recreational skiers [7]. However, these authors excluded female skiers on OC and those with previous knee injuries. According to the recommendations of Hewett et al. [15], we investigated a larger spectrum of female recreational skiers regardless of OC use and previous injuries.
We found similar OC use rates of 34.4 and 35.5% in subjects and controls, respectively. In comparison, Agel et al. [2] reported an OC use rate of 32.5% in 3,150 female soccer and basketball players. Lebrun [16] stated that in the general population, 20–30% of women of reproductive age (15–44 years) use OC, whereas the current OC use in Germany is about 40% [13]. In our study, no significant association between ACL injuries and OC use could be detected. These findings are well in accordance with the study by Agel et al. [2] where no difference in the rate of ACL and ankle injuries between those athletes using hormonal therapy and those not using hormonal therapy was found. In contrast, Moller-Nielson and Hammar [18] reported that athletes taking OC had a lower ACL injury rate. They speculated that OC may have significant influences on neuromuscular coordination and joint laxity [18]. Similarly, injured runners were less likely to use OC during their training programs [17]. However, other studies showed no preventive effects of OC use on soft tissue injuries [5, 9]. To date, a strong evidence for the preventive effect of the oral contraceptive pill against ACL injuries is missing [6, 15, 22]. Furthermore, most studies investigating OC use and injury risk focused on athletes in sports such as soccer and basketball [2], whereas we investigated recreational skiers. Although ACL injury mechanisms in alpine skiing [21] are different from other sports, our findings also indicate that OC did not have any protective effect against ACL injuries in recreational skiers.
Therefore, we divided the combined group of OC users and non-user in the preovulatory and postovulatory groups and compared the subjects and controls. Our results showed a significantly statistical association between the phase of the menstrual cycle and ACL injury. Significantly more ACL-injured subjects were in the preovulatory phase than control subjects (57 vs. 41%, P = 0.028). In accordance with our findings, Hewett et al. [15] showed a significant effect of the preovulatory phase for increased ACL injuries with OC users and non-users together when analyzing seven studies concerning menstrual phase and ACL injury risk in female athletes. Recreational female skiers in our study were estimated to be about 1.9 times more likely to tear their ACL in the preovulatory phase. In comparison, Beynnon et al. [7] revealed that the likelihood of recreational female skiers without OC use is estimated to be three times greater in the preovulatory phase of the menstrual cycle when analyzing serum concentrations of progesterone and estradiol. Interestingly, we found a striking similarity between our menstrual history data and the questionnaire data by Beynnon et al. [7]. In our investigation, 57% of ACL-injured subjects were in the preovulatory phase and 43% in the postovulatory phase. Exactly the same distribution was seen in the questionnaire data by Beynnon et al. [7]. Regarding the analysis of the menstrual history data by Beynnon et al. [7], they showed only a trend (P = .086) toward a 2.4 increase in ACL injuries in the preovulatory phase. Similarly, we showed also a statistical trend (P = .084) toward a 1.9 increase in ACL injury in the preovulatory phase when analyzing OC non-users only.
In accordance with other studies, our findings show an increase in non-contact ACL injuries in the preovulatory phase of menstrual cycle, i.e., the time period between menses and ovulation, but the influence of hormone fluctuations on ACL injury risk seems inconsistent. In women not using OC, the hormonal fluctuation of the estrogen concentration with a peak just before ovulation has been thought to be associated with greater ACL injury risk in the ovulatory phase (day 10–14 within an average cycle length of 28 days) [1, 26]. In contrast, Slauterbeck et al. [23] and Myklebust et al. [20] reported a significantly greater number of ACL injuries during the menstrual phase (day 1–7) when estrogen and progesterone concentrations are both low. Hewett et al. [15] showed that OC users are more prone to ACL injuries in the preovulatory phase as oral contraceptives stabilize hormone fluctuations during the menstrual cycle. Additionally, Wojtys et al. [26] reported that the estrogen levels at the time of the injury did not vary between OC users and non-users. Thus, the influence of hormone concentrations and fluctuations on ACL injury rate in the preovulatory phase remains unclear. It is speculated that the high-risk interval of suffering a non-contact ACL injury might be the phase with low progesterone level [1].
There are at least five limitations, which have to be considered. Firstly, due to the restriction of our patients to the ski clinic, we cannot exclude a possible selection of ACL-injured skiers. But most of the knee injuries occurring in the study area were treated in the ski clinic and there are no indications of any source of selection. Secondly, concern may arise regarding the classification of menstrual cycle phase using a questionnaire, because the accuracy of menstrual history data seems unclear [15]. The analysis of the menstrual history data by Beynnon et al. [7] found similar results as the analyzed blood sample, but the difference was not statistically significant. Additionally, Wojtys et al. [26] showed a large discrepancy between urine assay and questionnaire. However, Wojtys et al. [26] divided the menstrual cycle into three main phases: follicular, ovulatory and luteal. If we summarize the ACL-injured subjects from the follicular and ovulatory phases in the study by Wojtys et al. [26], menstrual history data contain 42 subjects in the preovulatory phase, whereas the urine assay contains 43 subjects indicating a good accordance between the two methods. Furthermore, Slauterbeck et al. [23] reported a 95% correlation between the questionnaire and hormone level estimation. Thus, we concluded that menstrual history data are accurate when classifying preovulatory and postovulatory phases in a large sample of subjects and controls. Thirdly, we did not record the various types of OC. Different oral contraceptives have different means of preventing ovulation [6]. These may lead to different associations with the ACL injury. However, Agel et al. [2] did not use classification of OC when analyzing the association of OC use on the rate of noncontact ACL injury and ankle sprains, although their subjects classified the OC in mono or triphasic pills. Fourthly, we used pooled data of OC users and non-users. Although subjects on OC do not ovulate, we divided subjects and controls into preovulatory and postovulatory phases according to other studies in this research area [15]. Fifthly, we studied a relatively low number of subjects (less than 100), which might be insufficient to draw a firm conclusion. Nevertheless, this investigation used the highest sample size in this research area [1, 7, 15] and represents one of only two case control studies [7].
Conclusion
The results of this study showed that the likelihood to sustain an ACL injury in recreational female skiers is greater in the preovulatory phase of the menstrual cycle, while OC use and previous knee injuries showed no association with the ACL injury rate. Therefore, female skiers, especially in the preovulatory phase of their menstrual cycle, should consider general recommendations to reduce the incidence of knee injuries, e.g., appropriate warming up, skiing at speeds conforming to individual skills and stopping skiing before the occurrence of muscle fatigue.
References
Adachi N, Nawata K, Maeta M, Kurozawa Y (2008) Relationship of the menstrual cycle phase to anterior cruciate ligament injuries in teenaged female athletes. Arch Orthop Trauma Surg 128:473–478. doi:10.1007/s00402-007-0461-1
Agel J, Bershadsky B, Arendt EA (2006) Hormonal therapy: ACL and ankle injury. Med Sci Sports Exerc 38:7–12. doi:10.1249/01.mss.0000194072.13021.78
Arendt EA, Agel J, Dick R (1999) Anterior cruciate ligament injury patterns among collegiate men and women. J Athl Train 34:86–92
Arendt EA, Bershadsky B, Agel J (2002) Periodicity of noncontact anterior cruciate ligament injuries during the menstrual cycle. J Gend Specif Med 5:19–26
Bennell K, Crossley K (1996) Muscoloskeletal injuries in track and field: incidence, distribution and risk factors. Aust J Sci Med Sport 28:69–75
Bennell K, White S, Crossley K (1999) The oral contraceptive pill: a revolution for sportswomen? Br J Sports Med 33:231–238. doi:10.1136/bjsm.33.4.231
Beynnon BD, Johnson RJ, Braun S, Sargent M (2006) The relationship between menstrual cycle phase and anterior cruciate ligament injury: a case–control study of recreational alpine skiers. Am J Sports Med 34:757–764. doi:10.1177/0363546505282624
Beynnon BD, Ettlinger CF, Johnson RJ (2007) Epidemiology and mechanisms of ACL injury in alpine skiing. In: Hewett TE, Shultz SJ, Griffin LY (eds) Understanding and preventing noncontact ACL injuries. American Orthopaedic Society for Sports Medicine, Human Kinetics, Champaign, pp 183–188
Brynhildsen JO, Hammer J, Hammer ML (1997) Does the menstrual cycle and use of oral contraceptives influence the risk of low back pain? A prospective study among female soccer players. Scand J Med Sci Sports 7:348–353
Burtscher M, Nachbauer W (1999) Injury risk of Austrian skiers and comparison of the injury pattern of traditional and carving skiers (German). In: Österreichisches Kuratorium für Alpine Sicherheit (eds) Sicherheit im Bergland, Innsbruck, Austria, pp 107–115
Burtscher M, Pachinger O, Mittleman MA, Ulmer H (2000) Prior myocardial infarction is the major risk factor associated with sudden cardiac death during downhill skiing. Int J Sports Med 21:613–615. doi:10.1055/s-2000-8481
Burtscher M, Gatterer H, Flatz M, Sommersacher R, Woldrich T, Ruedl G, Hotter B, Lee A, Nachbauer W (2008) Effects of modern ski equipment on the overall injury rate and the pattern of injury location in Alpine skiing. Clin J Sport Med 18:355–357. doi:10.1097/MJT.0b013e31815fd0fe
Heinemann K, Moehner S, Lewis M, Assmann A, Garbe E, Heinemann LA (2002) Trends of OC use 1980–1999 in a German cohort of women. Zentralbl Gynakol 124(2):128–131. doi:10.1055/s-2002-24241 (German)
Hewett TE (2000) Neuromuscular and hormonal factors associated with knee injuries in female athletes. Sports Med 29:313–327. doi:10.2165/00007256-200029050-00003
Hewett TE, Zazulak BT, Myer GD (2007) Effects of the menstrual cycle on anterior cruciate ligament injury risk: a systematic review. Am J Sports Med 35:659–668. doi:10.1177/0363546506295699
Lebrun CM (1994) The effect of the phase of menstrual cycle and the birth control pill in athletic performance. Clin Sports Med 13:419–441
Lloyd T, Triantafyllou SJ, Baker ER, Houts PS, Whiteside JA, Kalenak A, Stumpf PG (1986) Women athletes with menstrual irregularity have increased musculoskeletal injuries. Med Sci Sports Exerc 18:374–379. doi:10.1249/00005768-198608000-00002
Moller-Nielson J, Hammar M (1991) Sports injuries and oral contraceptive use: is there a relationship? Sports Med 12:152–160. doi:10.2165/00007256-199112030-00002
Myklebust G, Maehlum S, Holm I, Bahr R (1998) A prospective cohort study of anterior cruciate ligament injuries in elite Norwegian team handball. Scand J Med Sci Sports 8:149–153
Myklebust G, Engebretsen L, Braekken IH, Skjolberg A, Olsen OE, Bahr R (2003) Prevention of anterior cruciate ligament injuries in female team handball players: a prospective intervention study over three seasons. Clin J Sport Med 13:71–78. doi:10.1097/00042752-200303000-00002
Natri A, Beynnon BD, Ettlinger CF, Johnson RJ, Shealy JE (1999) Alpine ski bindings and injuries: current findings. Sports Med 28:35–48. doi:10.2165/00007256-199928010-00004
Renstrom P, Ljungqvist A, Arendt E, Beynnon B, Fukubayashi T, Garrett W, Georgoulis T, Hewett TE, Johnson R, Krosshaug T, Mandelbaum B, Micheli L, Myklebust G, Roos E, Roos H, Schamasch P, Shultz S, Werner S, Wojtys E, Engebretsen L (2008) Non-contact ACL injuries in female athletes: an International Olympic Committee current concepts statement. Br J Sports Med 42:394–412. doi:10.1136/bjsm.2008.048934
Slauterbeck JR, Fuzie SF, Smith MP, Clark RJ, Xu K, Starch DW, Hardy DM (2002) The menstrual cycle, sex hormones, and anterior cruciate ligament injury. J Athl Train 37:275–278
Stevenson H, Webster J, Johnson RJ, Beynnon B (1998) Gender differences in knee injury epidemiology among competitive alpine ski racers. Iowa Orthop J 18:64–66
Wojtys EM, Huston LJ, Lindenfeld TN, Hewett TE, Greenfield ML (1998) Association between the menstrual cycle and anterior cruciate ligament injuries in female athletes. Am J Sports Med 26:614–619
Wojtys EM, Huston LJ, Boynton MD, Spindler KP, Lindenfeld TN (2002) The effect of the menstrual cycle on anterior cruciate ligament injuries in women as determined by hormone levels. Am J Sports Med 30:182–188
Acknowledgments
The authors gratefully acknowledge the support for this study from the Tiroler Wissenschaftsfond (TWF).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ruedl, G., Ploner, P., Linortner, I. et al. Are oral contraceptive use and menstrual cycle phase related to anterior cruciate ligament injury risk in female recreational skiers?. Knee Surg Sports Traumatol Arthrosc 17, 1065–1069 (2009). https://doi.org/10.1007/s00167-009-0786-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-009-0786-0