
Abstract
Irreducible knee dislocation due to incarcerated soft tissue structures in associated fractures is extremely uncommon. We report a case of irreducible, closed dislocation of the knee secondary to incarcerated patellar tendon in a Hoffa fracture (unicondylar fracture of femur in the coronal plane) with associated communited fracture of patella and disruption of both cruciates. We treated this case initially with open reduction and internal fixation of fracture and repair of the patellar tendon. During the total followup period of eighteen months, the patient had restricted joint range of motion with no joint instability despite aggressive physiotherapy and further surgical intervention. The prognosis of such complex knee injuries with combination of ligamentous injuries and associated fractures is much worse when compared to either injuries alone.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Knee dislocation is an uncommon, serious injury with potential long-term implications representing less than 0.2% of all orthopaedic injuries [13]. Closed reduction of this dislocation is usually not difficult and irreducibility is extremely rare with Dubberley et al. [4] finding only 25 such cases reported in English literature. Various structures have been implicated to be the cause of irreducibility including medial retinaculum and capsule, vastus medialis, medial collateral ligament and patella with quadriceps tendon tear [1, 2, 9, 10, 15, 17]. Incidence of fractures of the distal femur associated with knee dislocation is low and has been reported to be around 4.5% [13] and we found only one report in literature of knee dislocation associated with unicondylar fracture of femur in the coronal plane (Hoffa fracture) [7, 14]. The case we present, to our best knowledge is the first to be reported in English literature of an irreducible, closed posterior dislocation of knee joint due to incarceration of patellar tendon in Hoffa fracture.
Case report
A 19-year old male was referred to the emergency department of our hospital following a motorcycle accident. He was treated at another center before the referral for brief loss of consciousness and pain and swelling of his right knee. A diagnosis of knee dislocation was made there and attempts to reduce the joint under sedation had failed. The patient was subsequently put on a long leg splint and referred to out hospital.
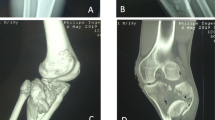
On examination, the patient had several superficial minor bruises and abrasions on the anterior aspect of the knee and there was obvious posterior displacement of the tibia. There was no distal neurovascular deficit of the limb. Emergency Doppler study showed an intact distal vascularity. Another attempt to reduce the knee under sedation was made in the emergency department by an orthopaedic consultant, which failed. On plain radiography, a communited fracture of the patella and coronal fracture of the lateral condyle of distal femur with posterior dislocation of the knee was seen (Fig. 1a). An MRI of the right knee was done, which showed the avulsed patellar tendon from the inferior pole of patella incarcerated in the lateral femoral condyle fracture (Fig. 1b, c). There were no further attempts at closed reduction, and the patient was taken to the operating room for emergent open reduction of his posterior knee dislocation.

a Preoperative lateral radiograph of right knee showing posterior dislocation with coronal fracture of lateral femoral condyle and patellar fracture. b Preoperative sagittal section MRI of knee showing torn patellar ligament incarcerated in the Hoffa fracture. c Preoperative axial section MRI of knee showing torn patellar ligament incarcerated in the Hoffa fracture. d Intraoperative photograph during open reduction showing torn patellar ligament displaced posterolaterally around the lateral femoral condyle. e Postoperative lateral radiograph of right knee at 6 months showing well united patellar and Hoffa fracture
The joint space was approached through an anterior incision and he was found to have a communited fracture of the patella involving the inferior pole and a sagittal split with the torn patellar tendon displaced posteriorly around the lateral aspect of the lateral condyle and incarcerated within the lateral femoral condyle fracture (Fig. 1d). The patellar tendon was freed and the joint was repositioned with flexion. Both the anterior cruciate and posterior cruciate ligaments were found to be torn at their femoral and tibial attachments respectively. No damage to the collateral ligaments or menisci was seen. The coronal fracture of the lateral femoral condyle was reduced and fixed using two Acutrack (Acumed LLC, Hillsboro, Oregon) screws. No repair of the cruciate ligaments was performed at this point. The two large fragments of the patella were fixed with K-wires and the patellar tendon was reattached using nonabsorbable pullout sutures. Associated tear of the medial retinaculum was also repaired. An additional cerclage wiring was done for the patella. Postoperatively the patient was kept on a long leg splint for 1 week after which gradual active joint range of motion exercises was started with non-weight bearing ambulation using crutches. At the end of 8 weeks, the patient had a range of motion of 90° flexion with an extensor lag of 10° and was allowed partial weight bearing using crutches. The patient was subsequently advised active range of motion exercises and quadriceps strengthening exercises at home and monthly follow-up.
At 3 months follow-up, the patient presented with complaints of limited knee range of motion and had fixed flexion deformity of 30° with further flexion of upto 80° with no obvious ligament laxity clinically. Plain radiographs of the right knee showed union of both fractures (Fig. 1e). An arthroscopic evaluation of the knee was subsequently performed, which showed no irregularity of patellar surface or any patellofemoral arthritic changes but severe fibrosis in the suprapatellar pouch, medial and lateral gutters for which an adhesiolysis was performed. The torn cruciates were debrided to their stumps and both the menisci were found to be intact and stable. On table, flexion of upto 110° from full extension was achieved. One month after this procedure with regular supervised physiotherapy, the patient had upto 90° of flexion. However, this did not improve and at the end of 18 months after the index open reduction procedure, the knee range of motion had decreased to 10°–80° flexion with no pain or joint instability and no signs of laxity.
Discussion
This is a first case report of irreducible, closed posterior dislocation of the knee associated with fracture of the lateral femoral condyle and patella. The patient also had associated tear of the patellar tendon and medial retinaculum, anterior and posterior cruciate ligaments. The torn patellar tendon, which was incarcerated in the Hoffa fracture was the cause of irreducibility of the dislocation.
Literature review did not reveal any case with this type of associated fractures and this cause of irreducibility of knee dislocation. The commonest soft tissue obstacle for closed reduction has been reported as interposition or buttonholing of the medial capsule or retinaculum and is clinically characterised by the dimple sign (medial puckering or furrowing of skin along the medial joint line) [2, 4, 9, 15]. This clinical sign was absent in our patient. The exact mechanism of trauma in our patient is not known and a direct force acting on a flexed knee at the time of motorcycle riding with the lateral femoral condyle receiving a shearing force from the posteriorly displaced tibia is the probable cause of communited fracture of patella and Hoffa fracture with disruption of the patellar tendon and cruciates [7, 8]. Cady et al. [2] reported a case of irreducible posterior dislocation of the knee in a 53-year old male in which the patella, following complete tear of the quadriceps tendon got incarcerated in the joint and prevented reduction with associated disruption of both cruciates and the posterolateral corner. Ashkan et al. [1] reported a similar case in a 37-year old male with identical soft tissue disruption. Both were treated with open reduction and repair of the extensor tendon.
The major concern in the absence of neurovascular injury following knee dislocation is the sequelae of soft tissue disruption. Disruption of ligamentous structures of the knee is not only associated with instability but also limit knee range of motion. The definitive approach to treatment of ligamentous injury in knee dislocation is controversial with some reporting good results with nonoperative management and ligament reconstruction only in the presence of significant instability [3–5, 10] and other reports suggesting better functional outcome with surgical reconstruction [6, 11, 12]. However, early surgical treatment is associated with increased risk of arthrofibrosis and heterotrophic ossification [11] and in patients in whom ligament reconstruction has been performed, post traumatic arthritis may be expected in up to 50% of patients in the long term [13, 16]. Most reports in literature of knee dislocation with ligament injuries mentioned above do not include cases with associated fracture around the knee joint.
Schenck et al. [14] reported a series of four patients with femoral-sided fracture-dislocation of the knee out of which only one patient had disruption of both cruciates with an associated medial Hoffa fracture. This patient underwent open reduction and internal fixation of the fracture with reattachment of the avulsed posterior cruciate ligament. However, in spite of aggressive physiotherapy postoperatively, the patient developed knee stiffness and was treated with arthroscopic synovectomy and manipulation. The final range of motion in this patient at 26 months follow-up was −5 to 100°. Schenck et al. [14] concluded that despite early fracture fixation and ligament repair the patients had significant functional deficit. Stability after knee dislocation with both cruciate disruption and associated fractures of distal femur or patella is not the disabling problem as compared to joint stiffness as illustrated by our case and cases reported in other series [8, 14].
We did not perform repair or early reconstruction of the cruciate ligaments in view of the associated fractures and swelling initially to avoid subsequent arthrofibrosis. Our initial plan was to perform a ligament reconstruction after fracture union but our patient developed knee stiffness by the time the fractures united in spite of arthroscopic adhesiolysis, aggressive physiotherapy and initial good response; the final improvement in joint motion was not considerable. The ligament reconstruction procedure was deferred subsequently in view of limited joint motion and no joint laxity. Though he is able to carry out his daily activities, the functional deficit caused by restricted joint motion still remains.
We have presented a case of posterior dislocation of knee, which was irreducible due to an extremely rare cause with associated Hoffa and patellar fractures. Literature is lacking regarding such cases and the treatment guidelines in this situation is unclear. The initial good results of early fracture fixation and aggressive physiotherapy may not necessarily give subsequent good joint range of motion. The prognosis of such complex knee injuries with combination of ligamentous injuries and associated fractures is much worse when compared to either injuries alone.
References
Ashkan K, Shelly RW, Barlow IW (1998) An unusual case of irreducible knee dislocation. Injury 29:383–384
Cady CE, Cardoni AL, Berger MJ (2007) An irreducible posterior knee dislocation. Am J Emerg Med 25:240–242
Dedmond BT, Almekinders LC (2001) Operative versus nonoperative treatment of knee dislocations: a meta-analysis. Am J Knee Surg 14:33–38
Dubberley J, Burnell C, Longstaffe A et al (2001) Irreducible knee dislocation treatedby arthroscopic debridement. Arthroscopy 17:316–319
Giannoudis PV, Roberts CS, Parikh AR et al (2005) Knee dislocation with ipsilateral femoral shaft fracture: a report of five cases. J Orthop Trauma 19:205–210
Harner CD, Waltrip RL, Bennett CH et al (2004) Surgical management of knee dislocations. J Bone Joint Surg Am 86:262–273
Holmes SM, Bomback D, Baumgaertner MR (2004) Coronal fractures of the femoral condyle: a brief report of five cases. J Orthop Trauma 18:316–319
Kasanovic M, Komadina R, Batista M (1998) Patella fractures associated with injuries of the knee ligament. Arch Orthop Trauma Surg 117:108–109
Kilicoglu O, Akman S, Demirhan M et al (2001) Muscular buttonholing: an unusual cause of irreducible knee dislocation. Arthroscopy 17:E22
Kontakis GM, Christoforakis JJ, Katonis PG et al (2003) Irreducible knee dislocation due to interposition of the vastus medialis associated with neurovascular injury. Orthopedics 26:645–646
Liow RY, McNicholas MJ, Keating JF et al (2003) Ligament repair and reconstruction in traumatic dislocation of the knee. J Bone Joint Surg Br 85:845–851
Richter M, Bosch U, Wippermann U et al (2002) Comparison of surgical repair or reconstruction of the cruciate ligaments versus nonsurgical treatment in patients with traumatic knee dislocations. Am J Sports Med 30:718–727
Robertson A, Nutton RW (2006) The dislocated knee. Curr Orthop 20:95–102
Schenck RC, MacGanity PLJ, Heckman JD (1997) Femoral-sided fracture-dislocation of the knee. J Orthop Trauma 11:416–421
Urguden M, Bilbasar H, Ozenci AM et al (2004) Irreducible posterolateral knee dislocation resulting from a low-energy trauma. Arthroscopy 20(Suppl 2):50–53
Werier J, Keating JF, Meek RN (1998) Complete dislocation of the knee—the long-term results of ligamentous reconstruction. Knee 5:255–266
Wilson TC, Talwalkar J, Johnson DL (2005) Lateral patella dislocation associated with an irreducible posterolateral knee dislocation: literature review. Orthopedics 28:459–461
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shetty, G.M., Wang, J.H., Kim, S.K. et al. Incarcerated patellar tendon in Hoffa fracture: an unusual cause of irreducible knee dislocation. Knee Surg Sports Traumatol Arthr 16, 378–381 (2008). https://doi.org/10.1007/s00167-007-0431-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-007-0431-8