
Abstract
The purpose of this study was to evaluate the histologic changes that occur between 3 and 12 weeks in an intra-articular, semitendinosus autograft, which was harvested without detachment of its tibial insertion and was placed through tibial and femoral drill holes, in a rabbit model. About 30 New Zealand white rabbits underwent ACL replacement using a semitendinosus tendon autograft. The normal ACL was transected at its femoral and tibial insertions. The tendon graft was harvested without detachment of its tibial insertion and its free end was secured with sutures. The graft was then passed through one tibial and one femoral tunnel and secured at the lateral femoral condyle. All animals were divided into three groups and were killed at 3, 6 and 12 weeks after surgery. Nine more animals underwent ACL reconstruction using a free semitendinosus tendon autograft. These animals were used as controls. The intra-articular portion of the graft and the interface between the bone tunnel and the graft was evaluated postoperatively for gross morphology and histological appearance. Results of this study showed that in a rabbit model the semitendinosus tendon autograft retained its viability when harvested without detachment of its peripheral insertion. On contrary, at the control group, necrosis of the graft was observed 3 weeks after surgery and progressively revascularization and maturation occurred 6 and 12 weeks after surgery. Retaining the tibial insertion of the semitendinosus autograft seems to preserves its viability and bypasses the stages of avascular necrosis and revascularization that occurs with the use of a free tendon autograft.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Despite the long-lasting research [10] the ideal method of reconstructing the anterior cruciate ligament (ACL) has not been found so far. Iliotibial band, menisci, patellar tendon, hamstrings, allograft tissue, synthetics, and a variety of combinations of these materials, all have been used for the reconstruction of this important human ligament.
During the last decades, studies have shown the superiority of biologic grafts, mainly because of their potential remodeling and integration into the joint [1–3, 9, 11]. Bone patellar tendon bone (BPTB) graft has gained in popularity after Noyes et al. [30] published data on the biomechanical properties of human graft tissue that showed the patellar tendon to be the strongest available autograft. More recently attention has shifted to the increased use of the hamstring tendon graft with its relatively low donor site morbidity [12, 19, 23, 41] and the strong indications for its regeneration potential [28]. On the other hand, harvesting semitendinosus and detaching its peripheral attachment no signs of necrosis were noticed [36]. Many authors have suggested that the success of an intra-articular graft depends on many factors, including the initial mechanical properties of the graft [29, 42], the positioning of the graft [25, 26], the fixation method [20, 28] and the postoperative rehabilitation of the knee. Nevertheless, other authors support that even more important is the biologic behaviour of the graft and especially during the first weeks after its implantation, as it undergoes the process of avascular necrosis and revascularization and maturation [16, 17, 27]. Indeed many studies in animal experiments have shown the detrimental effects, of the graft necrosis (and revascularization process), on the mechanical properties of (the autografts and especially) the free semitendinosus graft (tendon) [14, 24, 39].
The purpose of this study was to evaluate the histologic changes that occur between 3 and 12 weeks in an intra-articular, semitendinosus autograft, which was harvested without detachment of its tibial insertion and was placed through tibial and femoral drill holes, in a rabbit model.
Animals and methods
Thirty male adult New Zealand white rabbits weighing between 3,000 and 3,500 g underwent ACL reconstruction of their right knee using a semitendinosus tendon autograft that was harvested without detachment of its peripheral (tibial) insertion. Additionally nine animals underwent ACL reconstruction of their right knee using a free semitendinosus tendon autograft and these animals were used as controls. The protocol for animal subjects was approved by the ethic committee and is according to the state’s relevant laws and regulations. International directives for handling experimental animals used in medical research were followed [4, 32]. All animals were observed by veterinarian and considered to be free of disease before surgery. The animals of both groups were divided in three groups and were killed 3, 6, and 12 weeks postoperatively. Afterward, histologic evaluation of the grafts was performed.
Surgical procedure
Each animal received preoperatively a single dose of intra-muscular prophylactic antibiosis (second generation cefalosporin). The animals were then anaesthetized with ketamine (35 mg/kg) and silexin (5 mg/kg). The right knee was shaved, scrubbed with betadine and aseptically draped. A medial para-patellar incision was made and after a lateral patellar dislocation the normal ACL was excised at its femoral and tibial origins. A 2 mm drill hole was made at the tibia and the lateral femoral condyle at the footprints of the normal ACL. The semitendinosus tendon was identified and transected at its musculotendinus junction, retaining the peripheral (tibial) insertion. The free end of the autograft was secured with Dexon 3-0 suture and was passed through the tibial and femoral drill holes and secured at the lateral surface of the lateral femoral condyle with intra-osseous sutures. In the control group of the animals that a free semitendinosus tendon autograft was used, both graft ends were secured with Dexon 3-0 sutures at the tibial tuberocity and at the lateral femoral condyle, in a distance less than 1 cm from the drill hole, in order to diminish the bungee effect phenomenon. The incision was closed routinely in layers. Postoperatively knees were immobilized with plastic plaster for 2 weeks and then unrestricted activity was allowed.
Groups
Animals were divided into three groups and were killed 3, 6 and 12 weeks postoperatively. Each group consisted of ten animals that had ACL reconstruction with semitendinosus autograft that retained the tibial origin and three animals that had ACL reconstruction with free semitendinosus autograft.
Histologic analysis
The surgically treated knees were removed and carefully stripped from the surrounding soft tissues except from the autograft itself. The specimens were then fixed in 10% buffered formalin, decalcified and sections of 5 μm thick were taken through the intra-articular portion of the graft and at the level of bony tunnels and stained with haematoxylin–eosin. Histologic evaluation of the samples was performed with light microscope.
Results
Two rabbits died prematurely and were replaced. One animal had septic arthritis and eliminated from the study. All the grafts were intact at the time of the evaluation. Macroscopically, the autografts were white in colour with densely packed fibre bundles but they did not have the pearly appearance of the normal ACL. The shape was cylindrical and the orientation straight. About 12 weeks post-op autografts of both groups were covered with synovial membrane rich in blood vessels.
Three weeks post-op
At 3 weeks, animals (in both groups) displayed intense inflammatory response around the autografts and especially at the level of the sutures. (At the animals that the semitendinosus tendon retained its tibial insertion, the tendons displayed compact parallel fibres and areas of disorganized collagen matrix.) The tendons displayed compact parallel fibres and areas of disorganized collagen matrix, in the animals whose the semitendinosus tendon retained its tibial insertion. Mild or intense vascularity was observed with plentiful new formed vessels. The intra-osseous portion was surrounded by haphazardly arranged trabecular bone. Granulation tissue, rich in young fibroblasts was formed in the tendon–bone interface. Focally, small areas of necrosis were observed (Fig. 1a, b).

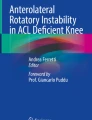
a Third post-op week. Intra-articular portion of the rerouting semitendinosus (graft that retains its tibial origin). Good cellularity and vascularity, compact collagen fibres and small areas of necrosis (long arrows) [Η-Ε, ×100]. b Third post-op week. Intra-articular portion of a free autograft. Avascular–acellular necrosis of the graft. [Η-Ε, ×100]

a Third post-op week. Intra-osseous portion of the rerouting semitendinosus (graft that retains its tibial origin). Good tendon cellularity. Focal osteoblastic reaction at the fringes of the bony tunnel. Smooth junction between the tendon and the bone. [Η-Ε, ×200]. b Third post-op week. Free autograft. Necrotic intra-osseous portion of the graft. Initiation of damage restoration with fibroid infiltration along new formed vessels [Η-Ε, ×400]
On the contrary, at the animals with the free autograft, 3 weeks postoperatively, the tendon graft had the image of avascular necrosis, with small areas of vital disorganized collagen matrix (Fig. 2a, b).
Six weeks post-op
At 6 weeks, irrespective from the surgical technique, the inflammatory reaction was minimized and vascularity sufficient. At the animals that the semitendinosus tendon retained the tibial insertion, the grafts showed disorganized architecture and increased cellularity and vascularization but no signs of necrosis. The bone tendon bonding was by means of loose connective tissue (Fig. 3a). The free tendon graft, 6 weeks postoperatively showed disorganized architecture and signs of neo-vascularization but also small areas of necrosis. There was no direct attachment between tendon and bone and the interface was composed by loose connective tissue (Fig. 3b).

a Sixth post-op week. Intra-osseous portion of the rerouting semitendinosus (graft that retains its tibial origin). Disorganized architecture of the graft but no signs of necrosis. Excellent restoration of the bone-graft bonding. [Η-Ε, ×100]. b Sixth post-op week. Intra-osseous portion of a free autograft. Smooth tendon—bone transition. Well vascularized tendon but still hypocellularity in comparison with the graft that retains the tibial attachment [Η-Ε, ×200]
Twelve weeks post-op
Twelve weeks postoperatively, at the animals with the graft that retained the tibial insertion, the tendon grafts showed well preserved architecture and cellularity. Restoration of the bone–graft bonding (a firm attachment) to the well-formed tunnel was observed (Fig. 4a). The whole graft image was similar to that of a normal ligament. At the animals with the free tendon, 12 weeks postoperatively the graft showed good architecture and cellularity, decrease at the size and number of the vessels and restoration of the bone–graft bonding (firm attachment of the graft to the bony tunnel) (Fig. 4b). Focally, there were still areas of disorganized architecture and degenerative alterations.

a The 12th post-op week. Intra-osseous portion of the rerouting semitendinosus (graft that retains its tibial origin). Strong attachment of the graft to the bone. Good architecture, vascullarity and cellularity. b The 12th post-op week. Intra-osseous portion of a free autograft. Good cellularity and vascularity. Good architecture but still correctional type alterations of the graft and osteoblastic reaction [Η-Ε, ×200]
Discussion
From the anatomy, we know that tendons receive their blood supply from vessels in the perimysium, the periosteal insertion, and the surrounding tissue via vessels in the paratenon or mesotenon. Additionally, there are studies confirming that tendons also receive diffusional (synovial) nutrition [6]. Even though gracillis and semitendinosus tendon autografts that retain its peripheral or central origins have been used quite early [8, 21, 22], there are no sufficient studies concerning the biologic behaviour of these “vascularized” autografts.
Numerous previous studies in animal models and in humans as well, have shown that patellar tendon and hamstring autografts undergo the process of avascular necrosis and revascularization the first period after their implantation [1, 3, 5, 9, 13–16, 40]. This process lasts from 3 months to 1 year or even more according to some authors [1]. Additionally, subsequent studies have confirmed the detrimental effects of (revascularization) avascular necrosis on the mechanical properties on the autografts: Kennedy et al. [18] studied semitendinosus reconstructions in a rabbit model and reported that at 26 weeks the graft strength was 40–50% of the original semitendinosus and 15–20% of the normal ACL. Grana et al. [14] investigated a semitendinosus autograft and concluded that failure of the graft occurred by rupture of its intra-articular part and not from pullout from the bone tunnel after 2 weeks. Similar were the conclusions of Blickenstaff et al. [5] who also concluded that even one year after a free semitendinosus autograft implantation large differences persist in strength and stiffness of the graft when compared with the normal tendon or ACL. So, there are strong evidences that the avascular necrosis and the revascularization process are critical for the mechanical properties of the grafts during the first weeks of the ACL reconstruction. (Consequently, it is logical to hypothesize that, irrespective of the fixation method, preserving autografts viability is crucial for a successful ACL reconstruction surgery.)
It was back in the 1980s when the first studies on “vascularized” patellar tendon autografts were made [3, 6, 7, 31, 37]. Nevertheless, results from these studies have shown that preserving the peripheral usually insertion of patellar tendon does not preserve its vitality and the graft undergoes the necrosis–revascularization process. The explanation of this came from studies of Noyes et al. [37] and Paulos et al. [6], who showed that patellar tendon receives the majority of its blood supply from two major sources, the fat pad and the retinaculum and not in continuity from its peripheral or central origins. Similarly, Arnoczky et al. [3] after their animal study with dogs, concluded that “The tibial attachment of the patellar tendon graft did not contribute any vessels to the revascularization process”.
On the other hand, things might be different with the use of hamstrings tendons.
Previous studies in our laboratory evaluated the biologic behaviour of semitendinosus tendon autografts 3–22 weeks after ACL reconstruction surgery [36]. The autografts were harvested without detachment of the musculotendinus junction. The histologic evaluation showed that grafts received sufficient blood supply from the central origins and retained their viability in all time periods with no signs of avascullar–acellular necrosis.
In another interesting study, in 2003, Zaffagnini et al. [43] evaluated the neurovascular network of the pes anserinus at its tibial insertion. They concluded that semitendinosus and gracilis tendons receive the majority of their blood supply from a well developed vascular network at the tibial attachment. (Blood vessels from tibia proceeded along the tendons of pes anserinus and decreased in diameter.) Whether or not this amount of blood supply is sufficient to keep viable a hamstring autograft that is harvested without detachment of the tibial attachment remained unknown at the time and in fact was the aim of the present study.
In an animal model, we investigated the histologic changes that occur 3, 6 and 12 weeks after the implantation of an intra-articular semitendinosus tendon autograft that was harvested without detachment of the tibial insertion. A number of control animals were used to compare the histologic behaviour of free semitendinosus tendon autograft at the same time periods.
In the present study, we have compared the effect on tendon viability when is rerouted, preserving its peripheral attachment and when it is used as single bundle free graft. The results of this investigation support our feeling, that retaining peripheral insertion of semitendinosus, preserves enough blood supply to keep the tendon viable during the fist crucial weeks so you might introduce early and intensive rehabilitation.
During the phase of necrosis, there is no doubt, that the strength of the tendon is diminished. In the long term and following revascularization, the strength of the tendon might be increased, but this possibility has not been investigated in the present study. We have also not investigated the effect on revascularization, when the tendons are bundled together. This is out of the purposes of the present study.
Interestingly, at 12 weeks, macroscopic and histologic features were more or less the same for the rerouting semitendinosus and the free graft.
We understand the limitations of the present study, that is: (a) an animal study and (b) absence of a method that actually quantify the histologic changes. Nevertheless, it is clear that in all time periods the autografts that retained the peripheral attachment were viable with no signs of avascular–acellular necrosis in all animals. On the contrary, the free autografts 3 weeks postoperatively were avascular–acellular or hypocelular and signs of revascularization were evident progressively 6 and 12 weeks post-op.
For the past three decades there has been an intensive effort to find a satisfactory intra-articular replacement of the ACL. The results have been the development of better methods of ACL reconstruction with stronger fixation and better graft harvesting techniques. Nevertheless, less attention has been given at the role of the biologic behaviour of the grafts. Increased laxity of the joint after ACL reconstruction may result from attenuation or rupture of the graft during the sensitive period when it undergoes the necrosis and revascularization process.
In conclusion, harvesting semitendinosus without detachment of the tibial attachment preserves a sufficient amount of blood supply to keep it viable. We consider that the developing of an ACL reconstruction technique that use semitendinosus not as a free autograft but as a graft that retains its natural attachment [33–36] may be more effective than the techniques that use free hamstrings autografts.
Based on our results, we are developing in our department a two bundle two tibial tunnel ACL reconstruction technique, using a semitendinosus tendon autograft that retains its musculotendinus origin and a gracilis tendon autograft that retains its peripheral (tibial) insertion [33–35]. The early results of this technique are very promising.
References
Abe S, Kurosaka M, Iguchi T, Yoshiya S, Hirohata K (1993) Light and electron microscopic study of remodeling and maturation process in autogenous graft for anterior cruciate ligament reconstruction. Arthroscopy 9:394–405
Amiel D, Kleiner JB, Roux RD, Harwood FL, Akeson WH (1986) The phenomenon of ‘ligamentization’: anterior cruciate ligament reconstruction with autogenous patellar tendon. J Orthop Res 4:162–172
Arnoczky SP, Tarvin GB, Marshall JL (1982) Anterior cruciate ligament replacement using patellar tendon. An evaluation of graft revascularization in the dog. J Bone Joint Surg 64A:217–224
Besch EL (1980) Environmental quality within animal facilities. Lab Anim Sci 30:385–406
Blickenstaff KR, Grana WA, Egle D (1997) Analysis of a semitendinosus autograft in a rabbit model. Am J Sports Med 25(4):554–559
Buckwalter JA et al (2000) Orthopaedic basic science. Biology and biomechanics of the Muskuloskeletal system, 2nd edn. American Academy of Orthopaedic Surgeons
Chiroff RT (1975) Experimental replacement of the anterior cruciate ligament. A histological and microradiographic study. J Bone Joint Surg Am 57(8):1124–1127
Cho KO (1975) Reconstruction of the anterior cruciate ligament by semitendinosus tenodesis. Bone joint Surg 57A:608–612
Clancy WR Jr, Rajesh GN, Rosemberg TD (1981) Anterior and posterior cruciate ligament reconstruction in rhesus monkeys. J Bone Joint Surg 63A:1270–1284
Dandy DJ (1996) Historical overview of operations for anterior cruciate ligament rupture. Knee Surg Sports Traumatol Arthrosc 3(4):256–261
Frank C, Amiel D, Woo SL-Y, et al (1985) Normal ligament properties and ligament healing. Clin Orthop 196:15–25
Fu HF, Bennett HC, Ma CB, Menetrey J, Lattermann C (2000) Current trends in anterior cruciate ligament reconstruction. Part II: operative procedures and clinical correlations. Am J Sports Med 28(1):124–130
Goradia VK, Rochat MC, Kida M, Grana WA (2000) Natural history of a hamstring tendon autograft used for anterior cruciate ligament reconstruction in a sheep model. Am J Sports Med 28(1):40–46
Grana WA, Egle DA, Mahnken R, et al (1994) An analysis of autograft fixation after anterior cruciate ligament reconstruction in a rabbit model. Am J Sports Med 22:344–351
Horstman JK, Ahmandu-Suka F, Norrdin RW (1993) Anterior cruciate ligament fascia lata allograft reconstruction: progressive histologic changes toward maturity. Arthroscopy 9:509–518
Howell SM, Knox KE, Farley TE, Taylor MA (1995) Revascularization of a human anterior cruciate ligament graft during the first two years of implantation. Am J Sports Med 23(1):42–49
Johnson LL (1993) The outcome of a free autogenous semitendinosus tendon graft in human anterior cruciate reconstructive surgery: a histological study. Arthroscopy 9(2):131–142
Kennedy JC, Roth JH, Mendenhall HV, et al (1980) Intraarticular replacement in the anterior cruciate ligament-deficient knee. Am J Sports Med 8:1–8
Kohn D, Sander-Beuermann A (1994) Donor-site morbidity after harvest of a bone-tendon-bone patellar tendon autograft. Knee Surg Sports Traumatol Arthrosc 2:219–223
Kurosaka M, Yoshiya S, Andrish JT (1987) A biomechanical comparison of different surgical techniques of graft fixation in anterior cruciate ligament reconstruction. Am J Sports Med 15:225–229
Lindemann K (1950) Uber den plastischen Ersatz Kreutzbander durch gιtaitielte Sshnenverp-flanzung. Z Orthop 79:316–334
Macey HB (1939) A new operative procedure for repair of ruptured cruciate ligament of the knee joint. Surg Gynecol Obstet 69:108–109
Marcacci M, Molgora AP, Zaffagnini S, Vascellari A, Iacono F, Presti ML (2003) Anatomic double-bundle anterior cruciate ligament reconstruction with hamstrings. Arthroscopy 19(5):540–546 (review)
McFarland EG, Morrey BF, An KN, et al (1986) The relationship of vascularity and water content to tensile strength in a patellar tendon replacement of the anterior cruciate in dogs. Am J Sports Med 14:436–448
Melhorn JM, Henning CE (1987) The relationship of the femoral attachment site to the isometric tracking of the anterior cruciate ligament graft. Am J Sports Med 15:539–542
Muneta T, Yamamoto H, Sakai H, Ishibashi T, Furuya K (1993) Relationship between changes in length and force in in vitro reconstructed anterior cruciate ligament. Am J Sports Med 21:299–304
Nebelung W, Becker R, Urbach D, Ropke M, Roessner A (2003) Histological findings of tendon-bone healing following anterior cruciate ligament reconstruction with hamstring grafts. Arch Orthop Trauma Surg 123(4):158–163
Nikolaou VS, Efstathopoulos N, Wredmark T (2006) Hamstring tendons regeneration after ACL reconstruction: an overview. Knee Surg Sports Traumatol Arthrosc 15(2):153–160
Noyes FR, Butler D, Grood ES, Zernicke R, Hefzy M (1984) Biomechanical analysis of human ligament grafts used in knee ligament repairs and reconstruction. J Bone Joint Surg 66A:344–352
Noyes FR, Butler DL, Grood ES, et al (1984) Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg 66A:344–352
Noyes FR, Butler DL, Paulos LE, Grood ES (1983) Intra-articular cruciate reconstruction. I: perspectives on graft strength, vascularization, and immediate motion after replacement. Clin Orthop Relat Res 172:71–77
Olfert ED, Cross BM, Mc William AA (1993) Guide to the care and use of experimental animals: canadian council on animal care (CCAC), vol 1. Odario Canada. Appendix XV-A
Papachristou G, Kalliakmanis A, Papachristou K, Magnissalis EA, Sourlas J, Plessas S (2007) Comparison of fixation methods of double-bundle double-tibial tunnel ACL reconstruction and double-bundle single-tunnel technique. Int Orthop [Epub ahead of print]
Papachristou G, Nikolaou V, Frangia K, Sourlas J, Lazarettos J, Efstathopoulos N (2005) ACL reconstruction using autologous semitendinosus tendon graft retaining the tibial insertion. Histologic study in rabbit model. In: Proceedings of the 3rd biomechanic congress. IASTED, Spain
Papachristou G, Sourlas J, Magnissalis EA, Plessas Sp, Papachristou K (2006) ACL reconstruction and the implication of its tibial attachment for the stability of the joint: anthropometric and biomechanical study. Int Orthop [Epub ahead of print]
Papachristou G, Tilentzoglou A, Efstathopoulos N, Khaldi L (1998) Reconstruction of anterior Cruciate ligament using the doubled tendon graft technique: an experimental study in rabbits. Knee Surg Sports Traumatol Arthrosc 6(4):246–252
Paulos LE, Butler DL, Noyes FR, Grood ES (1983) Intra-articular cruciate reconstruction. II: replacement with vascularized patellar tendon. Clin Orthop Relat Res 172:78–84
Pyne J, Gottlieb D, Beynnon BD, et al (1992) Semitendinosus and gracilis, tendon graft fixation in ACL reconstruction. Trans Orthop Res Soc 17:245
Rodeo SA, Arnoczky SP, Torzilli PA, et al (1993) Tendon-healing in a bone tunnel. A biomechanical and histological study in the dog. J Bone Joint Surg 75A:1795–1803
Rougraff B, Shelbourne D, Gerth PK, Warner J (1993) Arthroscopic and histologic analysis of human patellar tendon autografts used for anterior cruciate ligament reconstruction. Am J Sports Med 21:277–284
Sachs RA, Daniel DM, Stone ML, Garfein RF (1989) Patellofemoral problems after anterior cruciate ligament reconstruction. Am J Sports Med 17:760–765
Woo SL-Y, Gomez MA, Seguechi Y (1983) Measurement of mechanical properties of ligament substance from a bone-ligament-bone preparation. J Orthop Res 1:22–29
Zaffagnini S, Golano P, Farinas O, Depasquale V, Strocchi R, Cortecchia S, Marcacci M, Visani A (2003) Vascularity and neuroreceptors of the pes anserinus: anatomic study. Clin Anat 16(1):19–24
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Papachristou, G., Nikolaou, V., Efstathopoulos, N. et al. ACL reconstruction with semitendinosus tendon autograft without detachment of its tibial insertion: a histologic study in a rabbit model. Knee Surg Sports Traumatol Arthr 15, 1175–1180 (2007). https://doi.org/10.1007/s00167-007-0374-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-007-0374-0