
Abstract
Although the treatment of anterior cruciate ligament (ACL) tears in skeletally immature patients is still controversial, several studies have advocated ACL reconstruction in selected patients to prevent secondary injury. The proximal tibial physis is a structure at risk during ACL reconstruction in young patients, and physeal growth complications have been reported after surgery in this area. The relationship between the ACL and the proximal tibial physeal/apophyseal regions is poorly understood. This study examined the MRI anatomy of the ACL and the proximal tibia apophysis and epiphysis. MRIs of 59 skeletally immature knees were reviewed (Average age = 12.75 years, range 6–15) to define the anatomy of the epiphyseal and apophyseal regions. Measurements were recorded in three parasagittal planes: (1) at the lateral border of the patellar tendon, (2) the lateral edge of the ACL insertion, and (3) the medial edge of the ACL insertion. A single three-dimensional (3D) computed tomography (CT) scan was used to evaluate the position of standard drill holes used in ACL reconstruction to assess for potential degree of injury to the epiphyseal and apophyseal growth plates. In the parasagittal planes, the average height of the epiphysis was 19.6, 20.7, and 21.5 mm at the lateral border of the patellar tendon, the lateral border of the ACL, and the medial border of the ACL, respectively. At the level of the same landmarks, the apophysis extended below the physis at an average of 20.2, 16.8, and 7.0 mm, respectively. Expressed as a percentage of epiphysis height this was an average of 104, 82, and 33%, respectively. Examination of 3D CT images revealed that variations in drill hole placement had effects on the volume of injury to the proximal tibial physis and apophysis. Drill holes that started more medial, distal, and with a steeper angle of inclination reduced the amount of physis and apophysis violated when compared with holes placed more lateral, proximal, and with a shallow angle of inclination. The proximal tibial physis and apophysis is vulnerable to injury by drill hole placement during ACL reconstruction in skeletally immature patients. This paper defines the anatomic relationship of the apophyseal and epiphyseal regions of the physis in the proximal tibia. The volume of injury to the physis can be reduced by avoiding tunnel placement that is too lateral or too proximal on the tibia. A better understanding of these relationships may guide the placement of tibial drill holes, which have a lower risk of producing significant physeal damage.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The incidence of mid-substance anterior cruciate ligament (ACL) tears in children is unknown, although studies have provided evidence that this injury is now recognized more frequently in children and adolescents [1–4]. Historically, ACL reconstruction in children has not been recommended because of concerns about potential physeal injuries from placement of transphyseal drill holes. Theoretically, these physeal injuries could lead to premature physeal closure with subsequent leg length discrepancy and/or angular deformity.
Recent studies of skeletally immature patients with ACL tears have demonstrated that non-operative treatment results in poor outcomes, especially in children that return to sports [5–7]. Because of the poor outcomes after ACL injury in young patients, some authors have advocated physeal-sparing techniques. These techniques may result in non-anatomic graft placement and the long-term function of these grafts is unknown [1, 8–11].
Recent studies have developed algorithms for treating ACL injury in skeletally immature patients, which include surgical reconstruction in carefully selected patients [1, 8–10, 12–21]. Some of these studies have advocated the placement of standard ACL reconstruction drill holes in the tibia and femur, even in patients with open physes.
The purpose of this study was to define the relationship between the ACL, and the proximal tibial epiphysis and apophysis in skeletally immature patients. The hypothesis was that the medial border of the tibial apophysis tapers close to the medial edge of the ACL. This relationship between the medial border of the ACL and tibial apophysis suggests that drill hole placement during ACL reconstruction can be performed without significant damage to the most peripheral and vulnerable region of the apophysis.
Material and methods
A database of pediatric patients who underwent diagnostic MRI for various clinical indications was reviewed. In all cases, the physeal plates were open and there were no injuries of the tibia tuberosity or apophysis. The study consisted of 59 patients, 41 males (ages 11–15), and 18 females (ages 6–15). The average age for all patients was 12.75 years ± 2.4. Scan dates ranged from 1996 to 2002. The dimensions of the physis, epiphysis, and the apophysis were assessed in three parasagittal planes. Measurements were recorded at the following parasagittal locations, using the image of the knee, which most closely defined these regions: (1) lateral border of the of the patellar tendon, (2) lateral edge of the ACL insertion, and (3) medial edge of the ACL insertion.
In each patient and parasagittal plane, the epiphyseal height and the combined epiphyseal and apophyseal height were recorded (Fig. 1).

Measurements of epiphysis, and epiphysis + apophysis in three sagittal planes. [left to right: (1) lateral border of the patellar tendon, (2) lateral border of the anterior cruciate ligament (ACL) insertion, and (3) medial border of the ACL insertion]
In order to further elucidate the implications of various drill-hole placements, a computed tomography (CT) scan from a 9-year-old female was used as a representative model to estimate physeal damage because of drill holes in three-dimensional (3D) space. This patient was chosen for detailed analysis because of the presence of open physes. Virtual drill holes were superimposed on the image. The relationships between the drill hole path and physis location were examined.
mri protocol
Patients were scanned on either GE Signa LX 1.5 T (Milwuakee, WI, USA), a Seimens Symphony 1.5 T (Erlangen, Germany) or a 0.3 T Hitachi Aries II (Hitachi Corporation, Osaka, Japan). All images were obtained with the patient in the supine position, knee in extension, and externally rotated approximately 15°. T1-weighted spin-echo (TR range/TE range, 400–800/7–20) sagittal images were obtained in all patients. Proton density and T2-weighted spin-echo or fast spin-echo images were also obtained in each patient. These images had the TR ranging from 3,000 to 6,000 ms and TE from 30 to 100 ms. Slice thickness was 3.0–4.0 mm and gap width was 0.5–1.0 mm. Matrix size was 256 × 256. The T1- and T2-weighted sagittal images were preferred for anatomical measurements. The images were downloaded to an independent workstation for analysis.
CT protocol
A CT scan (Toshiba Aquilion Multi-slice CT, TSX-101A, Toshiba Corporation, Tokyo, Japan) from a 9-year-old female patient was analyzed. The patient was positioned supine, with the knee supported and secured with sponges. The patient was shielded. The scan technique used 0.5 s rotation speed and a pitch with 1.0-mm reconstructions in both bone and standard soft tissue reconstruction algorithms. Multi-planar reformations were performed on a Toshiba Multi slice scan system image processor. The series were transferred to a Vitrea II workstation (Vital Images, Plymouth, MN, USA) for further data manipulations and reformations.
Two-dimensional radiographic measurement protocol
Standard workstation tools were used to make measurements of the epiphysis and apophysis. The height of the epiphysis and apophysis were determined by drawing a straight reference line perpendicular to the axis of the tibia (Fig. 1). The reference line was drawn through the most proximal point of the tibia. Measuring distally to the physis gave the height of the epiphysis and measuring the distance to the most distal aspect of the apophysis gave the combined height of the epiphysis and the apophysis.
A representative MRI series and 3D CT scan were analyzed with a superimposed drill hole similar to that used in ACL reconstruction. The images were reviewed for potential injury to the apophyseal and epiphyseal regions of the physis.
3D analysis protocol
Using a Vitrea II workstation (Vital Images, Plymouth, MN, USA), 2D axial images were used to create a 3D computerized model. Contour lines were drawn to define the region of the epiphysis. An ellipse was sized to the best approximation of the drill bit, and it was placed on the appropriate axial image to represent the location of the ACL insertion on the tibial plateau. A second ellipse was placed on a more distal axial slice to represent where a drill would be inserted and placement was verified in the sagittal and coronal planes. The ellipses were connected electronically, and the resulting image demonstrated a simulated drill hole path.
Results
In the sagittal plane, the average height of the epiphysis was 19.6 ± 3.0, 20.7 ± 2.4, and 21.5 ± 2.6 mm at the lateral border of the patellar tendon, the lateral edge of the ACL insertion, and the medial edge of the ACL insertion, respectively. The apophysis extended below the physis 20.2 ± 4.3, 16.8 ± 5.1, and 7.0 ± 4.5 mm at the lateral border of the patellar tendon, the lateral edge of the ACL insertion, and the medial edge of the ACL insertion, respectively. As a percentage of epiphysis height, the average at each of the three parasagittal planes were 104, 82, and 33%, respectively.
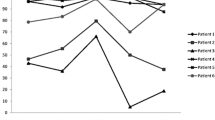
In all three sagittal planes, the apophysis extended below the physis. The apophysis tapers medially, with a rapid taper occurring at or just medial to the medial border of the ACL. In most patients, the MRI slice medial to the slice corresponding to the medial border of the ACL insertion showed no difference in height of the apophyseal portion of the epiphysis. Thus, the medial border of the ACL closely defines the medial extent of the apophysis in the sagittal plane. In some patients, there was not a measurable extension of the apophysis distal to the epiphysis in the parasagittal plane that corresponded to the medial border of the ACL. Complete measurements of the tibial apophysis appear in Table 1, and the distal extension of the apophysis as a percentage of the height of the epiphysis is plotted in Fig. 2.

Scatter plot showing extension of apophysis in three sagittal planes correlated with age. Extension of the apophysis is expressed as a percentage or epiphysis height. Sagittal images from top to bottom are: lateral border of the patellar tendon, the lateral border of the anterior cruciate ligament (ACL) insertion, and the medial border of the ACL insertion
A representative MRI image with open physes was analyzed in sagittal and coronal planes with superimposed drill holes. Figures 3 and 4 show the placement of a drill hole in the sagittal and coronal planes, respectively. The tibial tuberosity extends more distally in the region lateral to a tibial drill hole typically used for ACL reconstruction. Thus, a drill hole placed in a more lateral position had the potential to damage a larger portion of the apophyseal region of the physis. By moving the drill hole medially, as shown in Fig. 4, the apophysis is spared.

Sagittal images of the tibial tuberosity with superimposed drill hole (left to right: medial to lateral). The dotted red line represents the central directions of the drill hole, and the yellow circle represents the position of the periphery of the drill hole

Coronal images of the tibial tuberosity with superimposed drill hole (left to right: anterior to posterior). The dotted red line represents the central directions of the drill hole, and the yellow circle represents the position of the periphery of the drill hole
A representative sagittal CT image was analyzed with respect to the placement of drill holes in the proximal tibia (Figs. 5, 6). Two separate drill hole paths, with exit points at the anatomic insertion of the ACL on the tibial plateau, were superimposed on this CT image. The first hole has a starting position that is more proximal and with a shallower angle of inclination than the second hole. The modified starting point is more distal, with a steeper angle of inclination. The first drill hole violates a larger volume of the apophyseal portion of the physis, and the violation is in a more peripheral (anterior) region of the physis. The second drill hole avoids the apophyseal portion of the physis, and crosses the physis in a more central region.

Sagittal image of inferiorly placed drill hole (teal) in relation to more proximal placement (red). The more proximal first drill hole crosses a larger portion of the apophyseal portion of the physis, and the violation of the physis/apophysis is in a more peripheral (anterior) portion of the physis. The second drill hole avoids the apophyseal portion of the physis, and crosses the physis in a more central region

Three-dimensional representation of a drill hole, placed in a more medial and inferior position, which avoids violating the tibial apophysis
Discussion
The treatment of ACL injuries in young patients has been controversial because of concerns about physeal injuries, which have the potential for angular deformity and lower extremity length inequality [13, 22, 23]. Despite the concerns related to physeal arrest, there are very few reports of complications after transphyseal ACL reconstruction in skeletally immature patients [13, 24, 25]. Koman and Sanders reported a single case of distal femoral valgus after hamstring ACL reconstruction. The femoral fixation used in this case consisted of a transfixation pin across the lateral aspect of the femoral physis [26] (edited per reviewer’s comments).
A recent study by Kocher et al. found 15 previously undocumented deformities secondary to ACL reconstruction. This study suggests that ACL reconstruction does have the potential for clinically significant physeal and apophyseal injuries in skeletally immature patients [27]. Of these cases, all but one was because of the placement of interference screws, staples, transfixation pins, or bony plugs across the physis, large (12 mm) drill holes or suturing to the periosteum. There was one reported leg length discrepancy secondary to ACL reconstruction wherein no transphyseal hardware or bone plugs were implicated. The patient was an 11-year-old girl whose ACL reconstruction involved 6-mm drill holes and a hamstring allograft.
To prevent injury to the physis of the distal tibia and proximal femur, techniques for ACL reconstruction have been described that avoid the physis. Methods that avoid drilling across the physis include the over-the-top tibial [8–10, 28], and over-the-top femoral approaches [1, 9, 10, 14]. These extra-articular reconstructions employ non-anatomic placement of grafts. The clinical results of patients treated with these techniques demonstrate good outcomes for most patients; however, the follow-up measures in many of these studies were limited. Questions about the long-term function of grafts in non-anatomic positions have been raised [1, 11, 24, 29], although a recent study by Kocher et al. demonstrated good results of these grafts at longer follow-up [30].
Anderson has described a technique that uses epiphyseal placement of both tibial and femoral drill holes, which avoids the use of transphyseal graft placement. This report includes adequate follow-up (2–8.2 years), and this technique did not suffer from physeal complications in this group of 12 patients [31] (edited per reviewer’s comments).
Other studies on ACL reconstruction in adolescent athletes have not demonstrated significant complications related to transphyseal reconstructive techniques [1, 14, 15, 20, 29]. Lipscomb and Anderson performed transphyseal ACL reconstruction in 11 patients with open physes, and reported no leg-length discrepancies secondary to transphyseal drill holes [13]. Matava and Siegel [21] and Lo et al. [14] also reported highly successful transphyseal ACL reconstructions in skeletally immature athletes.
Some authors argue that the rare complications from a physeal arrest after ACL surgery are less detrimental contrasted with likely subsequent meniscal or chondral injuries in the non-surgically treated, ACL-deficient knee [24]. This argument is based upon several factors: (1) deformities secondary to physeal arrest can be corrected by osteotomy with minimal risk of complications [24, 26], (2) long-term studies of untreated ACL tears in active [12] and athletic [3, 6, 7, 15, 32, 33] pediatric patients demonstrate poor outcomes, (3) ACL reconstruction may reduce future meniscal and/or chondral injuries [34], and (4) ACL reconstruction may prevent, delay, or reduce the onset of degenerative osteoarthritis [34, 35], although this is controversial.
In a recent survey of orthopedic surgeons who treat pediatric ACL injuries, it was found that 77% of respondents operatively treat ACL injuries in children [27]. More studies of surgical anatomy in skeletally immature patients [36–38], and the development of techniques to minimize the risk of clinically significant physeal and apophyseal injuryies are needed. The risk of proximal tibial deformity is a significant concern, and the development of recurvatum after proximal tibial surgery or trauma is well defined in the literature [27, 39].
This study demonstrated several anatomic findings: (1) the tibial apophysis is a lateral structure, when analyzed with respect to the angle of orientation for a traditional tibial drill hole used for ACL reconstruction, (2) the medial border of the insertion of the ACL is very close to the medial edge of the tibial apophysis, and (3) the apophysis tapers rapidly from the lateral to medial direction. The 3D reconstruction used in this study demonstrated that: (1) a drill hole can be placed in a medial position, away from the medial edge of the patellar tendon and tibial apophysis and reduce the volume of injury to the most peripheral region of the apophysis, and (2) this drill hole can still be in proper position for ACL reconstruction. Furthermore, based on the anatomy of the apophysis (3) a tibial drill hole with a shallow angle of inclination has the potential to damage more of the apophysis.
This study has several limitations. Although non-invasive, MRI scanning loses a small amount of precision because of signal averaging between slices. Although the best slice was chosen for the anatomic regions analyzed in this study, some anatomic precision is sacrificed. This may account for some of the variability seen in the data. CT scans offer more precise resolution for osseous structures and 3D reconstruction from CT imaging is becoming readily available to the clinician. However, CT scanning requires exposing the pediatric patient to radiation which is preferably avoided unless critical to patient care.
Further anatomic studies of the pediatric knee should aim to develop a better understanding of the complex physeal/apophyseal anatomy. 3D imaging techniques may provide additional anatomic detail to reduce the volume of physeal/apophyseal injury.
Conclusion
This study found that the anatomy of the proximal tibia is a complex structure, and that medial aspect of the apophysis tapers rapidly near the medial border of the ACL. Based on the anatomy of the tibial physis and apophysis shown in this study, it was also found that minor variation in the starting position of tibial drill holes in the proximal tibia can reduce the volume of injury to the proximal tibial apophysis and epiphysis. A surgical technique that avoids the peripheral (anterior) portion of the tibia apophysis by using a drill hole that is placed medial and inferior to the edge of the apophysis will minimize the volumetric damage to the physis in the skeletally immature knee. This has the potential to reduce the risk for clinically significant physeal/apophyseal damage during ACL reconstruction.
References
Andrews M, Noyes FR, Barber-Westin SD (1994) Anterior cruciate ligament allograft reconstruction in the skeletally immature athlete. Am J Sports Med 22:48–54
Lo IK, Bell DM, Fowler PJ (1998) Anterior cruciate ligament injuries in the skeletally immature patient. Instr Course Lect 47:351–359
Pressman AE, Letts RM, Jarvis JG (1997) Anterior cruciate ligament tears in children: an analysis of operative versus nonoperative treatment. J Pediatr Orthop 17:505–511
Shea KG, Pfeiffer R, Wang JH, Curtin M, Apel PJ (2004) Anterior cruciate ligament injury in pediatric and adolescent soccer players: an analysis of insurance data. J Pediatr Orthop 24:623–628
Angel KR, Hall DJ (1989) The role of arthroscopy in children and adolescents. Arthroscopy 5:192–196
Graf BK, Lange RH, Fujisaki CK, Landry GL, Saluja RK (1992) Anterior cruciate ligament tears in skeletally immature patients: meniscal pathology at presentation and after attempted conservative treatment. Arthroscopy 8:229–233
Mizuta H, Kubota K, Shiraishi M, Otsuka Y, Nagamoto N, Takagi K (1995) The conservative treatment of complete tears of the anterior cruciate ligament in skeletally immature patients [see comments]. J Bone Joint Surg Br 77:890–894
Brief LP (1991) Anterior cruciate ligament reconstruction without drill holes. Arthroscopy 7:350–357
Micheli LJ, Rask B, Gerberg L (1999) Anterior cruciate ligament reconstruction in patients who are prepubescent. Clin Orthop 40–47
Robert H, Bonnard C (1999) The possibilities of using the patellar tendon in the treatment of anterior cruciate ligament tears in children. Arthroscopy 15:73–76
Stanitski CL (1995) Anterior cruciate ligament injury in the skeletally immature patient: diagnosis and treatment. J Am Acad Orthop Surg 3:146–158
Janarv PM, Nystrom A, Werner S, Hirsch G (1996) Anterior cruciate ligament injuries in skeletally immature patients. J Pediatr Orthop 16:673–677
Lipscomb AB, Anderson AF (1986) Tears of the anterior cruciate ligament in adolescents. J Bone Joint Surg Am 68:19–28
Lo IK, Kirkley A, Fowler PJ, Miniaci A (1997) The outcome of operatively treated anterior cruciate ligament disruptions in the skeletally immature child. Arthroscopy 13:627–634
McCarroll JR, Rettig AC, Shelbourne KD (1988) Anterior cruciate ligament injuries in the young athlete with open physes. Am J Sports Med 16:44–47
McCarroll JR, Shelbourne KD, Patel DV (1995) Anterior cruciate ligament injuries in young athletes. Recommendations for treatment and rehabilitation. Sports Med 20:117–127
Micheli LJ, Metzl JD, Di Canzio J, Zurakowski D (1999) Anterior cruciate ligament reconstructive surgery in adolescent soccer and basketball players. Clin J Sports Med 9:138–141
Mylle J, Reynders P, Broos P (1993) Transepiphysial fixation of anterior cruciate avulsion in a child. Report of a complication and review of the literature. Arch Orthop Trauma Surg 112:101–103
Simonian PT, Metcalf MH, Larson RV (1999) Anterior cruciate ligament injuries in the skeletally immature patient. Am J Orthop 28:624–628
Aronowitz ER, Ganley TJ, Goode JR, Gregg JR, Meyer JS (2000) Anterior cruciate ligament reconstruction in adolescents with open physes. Am J Sports Med 28:168–175
Matava MJ, Siegel MG (1997) Arthroscopic reconstruction of the ACL with semitendinosus-gracilis autograft in skeletally immature adolescent patients. Am J Knee Surg 10:60–69
Sanders JO (2000) Anterior cruciate ligament reconstruction in the skeletally immature high-performance athlete: what to do and when to do it? [comment]. Arthroscopy 16:392–393
Vahasarja V, Kinnuen P, Serlo W (1993) Arthroscopy of the acute traumatic knee in children. Prospective study of 138 cases. Acta Orthop Scand 64:580–582
Barber FA (2000) Anterior cruciate ligament reconstruction in the skeletally immature high-performance athlete: what to do and when to do it? Arthroscopy 16:391–392
Clark R (2000) Anterior cruciate ligament reconstruction in the skeletally immature high-performance athlete: what to do and when to do it? Arthroscopy 16:393–394
Koman JD, Sanders JO (1999) Valgus deformity after reconstruction of the anterior cruciate ligament in a skeletally immature patient. A case report. J Bone Joint Surg Am 81:711–715
Kocher MS, Saxon HS, Hovis WD, Hawkins RJ (2002) Management and complications of anterior cruciate ligament injuries in skeletally immature patients: survey of the herodicus society and the acl study group. J Pediatr Orthop 22:452–457
Parker AW, Drez D Jr, Cooper JL (1994) Anterior cruciate ligament injuries in patients with open physes [see comments]. Am J Sports Med 22:44–47
Shelbourne KD, Patel DV, McCarroll JR (1996) Management of anterior cruciate ligament injuries in skeletally immature adolescents. Knee Surg Sports Traumatol Arthrosc 4:68–74
Kocher MS, Garg S, Micheli LJ (2005) Physeal sparing reconstruction of the anterior cruciate ligament in skeletally immature prepubescent children and adolescents. J Bone Joint Surg Am 87:2371–2379
Anderson AF (2004) Transepiphyseal replacement of the anterior cruciate ligament using quadruple hamstring grafts in skeletally immature patients. J Bone Joint Surg Am 86A(Suppl 1):201–209
Angel KR, Hall DJ (1989) Anterior cruciate ligament injury in children and adolescents. Arthroscopy 5:197–200
Engebretsen L, Svenningsen S, Benum P (1988) Poor results of anterior cruciate ligament repair in adolescence. Acta Orthop Scand 59:684–686
Murrell GA, Maddali S, Horovitz L, Oakley SP, Warren RF (2001) The effects of time course after anterior cruciate ligament injury in correlation with meniscal and cartilage loss. Am J Sports Med 29:9–14
Jomha NM, Borton DC, Clingeleffer AJ, Pinczewski LA (1999) Long-term osteoarthritic changes in anterior cruciate ligament reconstructed knees. Clin Orthop 188–193
Shea KG, Apel PJ, Pfeiffer RP, Showalter LD, Traughber PD (2002) The tibial attachment of the anterior cruciate ligament in children and adolescents: analysis of magnetic resonance imaging. Knee Surg Sports Traumatol Arthrosc 10:102–108
Guarino J, Tennyson S, Barrios Y, Shea K, Pfeiffer R, Sabick M (2004) Modeling the growth plates in the pediatric knee: implications for anterior cruciate ligament reconstruction. Comput Med Imaging Graph 28:419–424
Kocher MS, Hovis WD, Curtin MJ, Hawkins RJ (2005) Anterior cruciate ligament reconstruction in skeletally immature knees: an anatomical study. Am J Orthop 34:285–290
Knight JL (1998) Genu recurvatum deformity secondary to partial proximal tibial epiphyseal arrest: case report. Am J Knee Surg 11:111–115
Acknowledgments
To Chris Hayden (Intermountain Medical Imaging, Boise, ID, USA) for his help with the CT software and image generation, and also to Drew Taylor (MRI Center of Idaho, Boise, ID, USA) for his help with compiling the MRI database.
Author information
Authors and Affiliations
Corresponding author
Additional information
The preliminary work on this topic was presented at the 2000 Meeting of the Pediatric Orthopaedic Society of North America, Vancouver, Canada, and the 2001 American Academy of Orthopaedic Surgeons Annual Meeting in San Francisco.
Rights and permissions
About this article
Cite this article
Shea, K.G., Apel, P.J., Pfeiffer, R.P. et al. The anatomy of the proximal tibia in pediatric and adolescent patients: implications for ACL reconstruction and prevention of physeal arrest. Knee Surg Sports Traumatol Arthrosc 15, 320–327 (2007). https://doi.org/10.1007/s00167-006-0171-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-006-0171-1