
Abstract
Questions addressed in this in-vitro study are (1) what are the actual three-dimensional kinematics of talus and calcaneus during an anterior drawer test as performed with the quasi-static anterior ankle tester (QAAT) (2) does laxity measurement with the QAAT represent the true anterior translation of talus relative to the tibia?. Simultaneous measurements were made with the QAAT and a three-dimensional kinematics analysis system in five specimens. The three-dimensional translations and rotations on three axes were analysed at 25, 50 and 100 N of applied anterior load, with increased ligament damage. For four out of five remaining specimens, anterior translation values of talus and calcaneus and values as measured with the QAAT show a significant increase with growing ligament damage and with higher loads. Skeletal motions of talus and calcaneus show great similarity in three different motion axes, with increased ligament damage and at any given load. Skeletal translations and rotations of talus and calcaneus show great similarity during an anterior drawer movement of the ankle joint. Anterior skeletal translation of the talus and calcaneus show fair correlation with the anterior displacements measurements of the QAAT. These QAAT measurements show an overestimation of the laxity value by more than 200% irrespective of the load applied.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Insufficiency of the lateral ankle ligaments affects normal ankle joint motion (Sammarco 1977). Several studies pointed out that lateral ankle joint ligament insufficiency can produce anterolateral laxity that allows the talus to rotate internally and dislocate anteriorly on the tibia (Brantigan et al. 1977; Ishii et al. 1996; Louwerens et al. 1995; Sammarco 1977). Reliable analysis of the functional status of the lateral ankle ligaments is important for treatment selection and prevention of long-term complications (Kannus and Renström 1991; Verhagen et al. 1995). Ligament injuries are found in 40% of the patients, who present with pain, fear of giving-way, actual instability and/or swelling that interfere with daily living and/or sports activities (Verhagen et al. 1995).
Although several diagnostic methods (radiographic stress tests, magnetic resonance imaging, arthrography) are helpful for assessing pathologic conditions of the ankle testing of the ankle joint laxity during clinical examination is still considered to be the most reliable analysis of lateral ankle ligament injuries. Anterior laxity is clinically tested using the manual anterior drawer test (ADT) (Klenerman 1998; van Dijk et al. 1996; Kerkhoffs 2005). However, also the ADT can be criticized because of its subjective nature and the inability to produce reproducible and quantitative results (Fujii et al. 2000). As part of an extensive study to develop an objective diagnostic test for anterior ankle joint ligament laxity, a quasi-static anterior ankle tester (QAAT) was developed that showed accurate inter and intra-observer reliability (Kerkhoffs et al. 2005a, b). However the actual validity of the tester has not been determined. On the basis of our previous findings in a patient study, the question has arisen whether the measured laxity values represent anterior translation of the talus relative to the tibia. The measured 20–30 mm are non-realistic laxity values if these represent the actual translation in the ankle joint. In many similar tests, anterior translation is measured between the posterior aspect of the calcaneus and the tibia (Kerkhoffs et al. 2001; Siegler et al. 1994; Tohyama et al 2003). Actual three-dimensional kinematics of the ankle joint during the test and how these relate to what is measured as anterior translation have not yet been described in detail.
The present in-vitro cadaver study describes the three-dimensional kinematics of the bony structures of the ankle joint during an anterior drawer movement as performed with the QAAT, with different levels of ligament damage. The aims of the study are (1) what are the actual three-dimensional kinematics of talus and calcaneus during an anterior drawer test as performed with the QAAT? (2) does laxity measurement with the QAAT represent the true anterior translation of talus relative to the tibia?
Methods
Test device
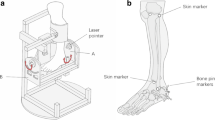
In the quasi-static anterior ankle tester (QAAT) (Kerkhoffs et al. 2005a, b), the tibia is firmly attached to a shank holder using straps; in the present tests the tibia was additionally fixated to a halo-frame with use of screws. The foot is held to the footplate using an additional strap. A linkage mechanism through a sub-frame allows manual force application on the anterior aspect of the tibia and posterior aspect of the heel resulting in an anterior drawer movement in the ankle joint. The footplate is attached to the moving sub-frame by means of a force transducer. The linkage mechanism allows manual force application up to a maximum of 200 N. The test is performed with the lower leg hanging downwards freely. As a result of the load at the heel of the patient, the horizontal footplate moves. The tester uses two displacement transducers to measure anterior translation of the heel relative to the tibia. One transducer measures the displacement of the footplate and sub-frame relative to the shank holder and the other transducer measures the displacement of the anterior aspect of the tibia relative to the shank holder (Fig. 1a). The applied force and the displacements of the footplate and the tibia are registered on-line during the test by a data-acquisition system. Data are shown on a computer screen, providing direct feedback to the observer. The intrinsic accuracy of the test device with respect to the measured values is 0.1 mm for the displacement and 1.0 N for the force.

a The quantitative, Quasi-static Anterior Ankle Tester. The tibia is firmly attached to a vertical construction (V) using straps (S1 and S2) and the foot is securely held to the footplate (F) using a strap (S3). A double handle system (H1 and H2) allows manual force application on the tibia and a resulting anterior drawer movement in the ankle joint. The applied load is registered by a force transducer (F2) that connects the vertical construction to the footplate. Two displacement transducers measure anterior translation of the heel relative to the tibia (M1) respectively the motion of the tibia in the vertical construction (M2). While testing, data can be read online on a computer screen (C) by the observer. b Test setting. Each specimen (S) was firmly attached through a haloframe (H) to a vertical construction (C) used for stable positioning of the specimen hanging freely downwards. Light emitting diodes (L) were used as markers. Two Optotrak position sensors (O) were used to continuously identify all markers during the test procedure. c Close-up fixation marker sets, anteromedial view of the ankle joint. Light emitting diodes (L) were fixed to fibula, tibia, talus and calcaneus with use of screws (S), thermoplastic holders (T) and instant glue
Specimens
Eight human lower leg specimens were obtained from five male and three female cadavers and stored at −20 degrees (mean age 67, range 61–73 years). Each specimen was thawed at room temperature for at least 12 h before testing. Three specimens were excluded from analysis due to problems with marker fixation (soft bone, loose grip) during the course of the test procedures. The remaining five specimens, four right and one left, went through the entire test protocol without noticeable failures in fixation; one specimen is presented separately because of apparent abnormal joint laxity due to ligament insufficiency that caused (partial) dislocation of the joint during the test.
Kinematic measurements
The Optotrak system (Northern Digital Inc., Canada) was used to determine motion and position of the bony structures of the ankle joint complex during an anterior drawer movement performed with the QAAT. The Optotrak system semi-automatically tracks 3D marker positions (infrared light-emitting diodes) in real time with an accuracy better than 0.1 mm (Northern Digital Inc., Canada). Three to four marks were rigidly fixated to the tibia, fibula, talus and calcaneus (Fig. 1c). Two Optotrak Position Sensors were used to continuously identify all markers during the entire anterior drawer movement.
Test procedure
Through a lateral surgical approach of the ankle joint, the lateral ankle ligaments (anterior and posterior talofibular and calcaneofibular ligament) were tagged with use of sutures. Skin, subcutaneous tissues, tendons and muscles of the lower leg were left intact as much as possible to optimally preserve the original anatomy for testing. Markers were fixed to fibula, tibia, talus and calcaneus with use of screws, thermoplastic holders and instant glue (Fig. 1c). Each lower leg was then firmly attached to a vertical construction used for stable positioning of the specimen hanging freely downwards (Fig. 1b).
After these preparations, calibration was performed with use of a calibration cage. The Z-axis of the calibration cage was set parallel to the long axis of the tibia. The Y-axis was aligned perpendicular to the Z-axis, in a plane defined by the Z-axis and the line joining the insertion of the Achilles tendon on the calcaneus and the second metatarsal head. The X-axis was perpendicular to the Z and Y-axes. This axis representation is similar to the one introduced by Allinger and Engsberg (1993). The positive Z-axis pointed proximally, the positive Y-axis anteriorly and the positive X-axis laterally. This definition was used for the right ankles. For the left ankle the positive X-axis pointed laterally. Consequently, after processing, the kinematic data were mirrored. The neutral position with the lower leg in the tester was the reference position from which the kinematics were quantified. By using this approach, the rotation axes were oriented in the anatomical planes. The cardan-convention was used for reconstructing the rotations, using the sequence X, dorsal-plantar flexion; Y, in-eversion; Z, in-external rotation (Crawford et al. 1996).
To enable reconstruction of the translations, the 3D location of anatomic reference points was measured with use of a digitising probe, a pen-like pointing instrument containing six Optotrak-markers. The point on the talar surface in the centre of the ankle joint and the point on the most posterior aspect of the calcaneus were selected as two alternative origins to evaluate the anterior translation of the talus and calcaneus relative to the tibia. The locations of these points relative to the markers attached to the bones, were determined after the kinematics measurements were finished. Prior to the kinematics measurements, the ankle joint complex was preconditioned by three times repeating the anterior drawer movement. Each measurement consisted of a set of three loading cycles. The first measurement took place with intact ligaments, the second after cutting of the anterior talofibular ligament (ATFL), the third after additional cutting of the calcaneofibular ligament (CFL) and the final measurement after cutting of the posterior talofibular ligament (PTFL).
Data capturing and analysis
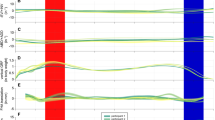
For data collection a custom software program written in LABVIEW (National Instruments Corp., Austin TX, USA) was used. Analysis of translation and rotation data was performed with use of MATLAB® (The Mathworks, Inc., Natick, MA, USA). From the continuous force-displacement data, the specific translation and rotation values were determined at 25, 50 and 100 N of applied load relative to the reading at 0 N (Fig. 2). Data were further processed with use of Microsoft Excel XPTM.

Raw measurements of intact specimens 1 and 3. The QAAT measurements and corresponding Y-translations of the talcocrural point on the talus are plotted in one graph. The loading and unloading directions are given in the graph of specimen 1. In the graph of specimen 3, the method is illustrated to calculate the laxity values at 25 N (L25), 50 N (L50) and 100 N (L100). The reference for the laxity calculation is the displacement reading at 0 N. The displacements at 0, 25, 50, and 100 N are calculated by linear regression on data points around the targeted value
For the calculations of the translations, different approaches were used. Firstly, to compare the actual anterior ankle joint laxity with the QAAT measurement, the anterior translation of the joint origin of the talus was calculated. Secondly, to evaluate the contribution of the calcaneus motions to the laxity measurements with the QAAT, the anterior translation of the calcaneus was calculated for the point at the posterior aspect of the calcaneus, as the alternative origin that moved with the calcaneus. Thirdly, to determine to what extend the talus and calcaneus move as one body, the calcaneus translations were calculated by using an alternative origin that coincided with the talus origin at the reference position of the joint and that virtually moved with the calcaneus. The concommittant rotations were calculated relative to the reference position where the axis systems of the talus, calcaneus and tibia were parallel.
A Pearson Correlation Coefficient was determined between anterior laxity values of the QAAT and Optotrak measurements. For determining the effect of sequential cutting of the ligaments and of the increasing force on the laxity measures as obtained by the QAAT and Optotrak ANOVA tests were used. For some tests T-tests were performed. All statistical tests were performed using SPSS 12.0.1 for Windows (SPSS Inc. Chicago, IL, USA)
Results
In a qualitative sense the QAAT-measurements appear to follow the actual anterior translation of the talus relative to the tibia. In specimen 1, a (partial) dislocation was observed that remained consistent throughout the test procedures. At the start of the test the force-displacement curve appears normal, but around 30–40 N a drop of the measured force was found combined with a sudden increase of the displacement (Fig. 2). This finding was reproducible with repeated loading in the subsequent tests. The anterior displacement as measured with the QAAT and Optotrak, was consistently much higher than in the other specimens. It was concluded that this specimen can be considered as an outlier. The data of this specimen were excluded from the subsequent analyses. For the four remaining specimens, the translation and rotation data at 25, 50 and 100 N relative to the measured values at 0 N were analysed (Fig. 2). The anterior displacement thus determined was considered as the anterior laxity.
The mean anterior laxity of the four remaining specimens, as measured by the QAAT, did not significantly increase after sequential sectioning of the anterior lateral ankle ligaments (ATFL, CFL and PTFL) (Fig. 3) (P = 0.12). The low power of the four cadaver specimens is the most probable cause for this finding. However, for the anterior laxity as determined from the talus and calcaneus motions, there was a statistically significant effect of ligament sectioning, as could be expected beforehand. The Bonferroni post-hoc analysis specified that there was only a significant difference between intact and all cutting conditions for the anterior laxity as determined from the talus translation (P < 0.05). For the anterior laxity based on calcaneus motions this significance was only after cutting the CFL (P < 0.05). These anterior laxities were calculated from the origin on the talar surface in the centre of the ankle joint that moved with the talus and for the point on the posterior aspect of the calcaneus that moved with the calcaneus. The effect of load on the anterior laxity as determined by the QAAT and skeletal motions of talus and calcaneus was statistically significant (P < 0.001) for all cutting conditions.

Anterior laxity at 25, 50 and 100 N of the intact specimens and after sequential cutting of the ATFL, CFL and PTFL. The laxity values are based on the Y-translations of the talocrural point on the talus, the Y-translations of the posterior point on the calcaneus and on the displacement reading of the QAAT. The data are averages and standard deviations of four specimens
By pooling the data from the 4 specimens, with increasing ligament damage and at the different force levels, a good relationship was found between the QAAT measurements and the anterior translations of the talus and calcaneus relative to the tibia. Correlation coefficients were 0.72 (P < 0.01) for the talus translations and 0.76 (P < 0.01) for the calcaneus translations if compared to the QAAT measurements, whereby the data at the different force levels and for the different ligament conditions were pooled.
The QAAT overestimated the actual anterior laxities of the talus by 6.5 times for the intact joint to 2.5 times after cutting all anterolateral ligaments. The anterior translations as calculated from the point on the posterior aspect of the calcaneus were higher than the talus translations, but this difference was by far not sufficient to explain the overestimation of anterior laxity by the QAAT (Fig. 3). The QAAT underestimated the laxity increase if compared to the talus laxity values.
The differences in translations and rotations between the talus and calcaneus were variable, small and not statistically significant when using the same reference coordinate system, i.e. with the coordinate axes parallel and the same origin on the talar surface in the centre of the ankle joint that moved with either the talus or calcaneus. With intact ligaments, the main motion was anterior translation (Fig. 4). The dorsal-plantar flexion that was found in the four specimens was not consistent. The other motions were small and variable. The only noticeable effects of cutting the anterolateral ligaments were the increase of anterior translation (P < 0.05) and small lateral translation (P < 0.05).

The translations and rotations at 100 N of the intact specimens and after sequential cutting of the ATFL, CFL and PTFL. The translations are based on the data of the talocrural point on the talus and of the talocrural point that is virtually attached to the calcaneus. The date are taken relative to the translation- or rotation readings at 0 N. The data are averages and standard deviations of four specimens. *Indicates that the mean value is significantly different from zero (P < 0.05, one-sample T-test). Explanation of the abbreviations: lat. lateral, med. medial, ant. = anterior, post. posterior, prox. proximal, dist. distal, dors. dorsal, plant. plantar, inv. inversion; ev. eversion, int. internal, ext. external
Mean translations and rotations of the fibula were small in all three motion axes, 0.6 mm (± 0.6 mm), −0.2 mm (± 0.6 mm), 0.1 mm (±0.3 mm) for the x-, y- and z- translation, respectively and 0.2° (± 0.1°), −0.1° (± 0.3°), −0.5° (± 0.4°) for the x-, y- and z-rotation respectively at 100 N anterior load with intact ligaments. Only the x-rotation (dorsal flexion) was not significantly different from zero (P = 0.03). There were no statistically significant effects of ligament cutting.
Discussion
An easy, non-invasive anterior ankle tester for ligament laxity measurements is desirable to substitute the manual anterior drawer test during delayed physical examination and clinical diagnosis of acute and chronic lateral ankle instability complaints. For the evaluations of therapeutic interventions, a quantitative measure is preferred over a subjective manual examination. Logically, an externally applied measuring device cannot be as exact as recordings with devices secured directly to the bones (Almquist et al. 2002; Jorn et al. 1998). In a previous study, the QAAT proved to be a reliable test device with questionable validity (Kerkhoffs 2005). In the present in-vitro study, the 3D kinematics of the talus and calcaneus during an anterior drawer movement of the ankle joint were analysed. Secondly, the validity of a simple anterior ankle tester was evaluated. Disadvantages of this in-vitro study design were that pain due to fixation of the test device as well as lack of control over self-generated muscle tonus and post-mortem stiffness with differences in soft tissue compliance were not taken into account. For the evaluation of the validity of the tester, that uses points on the heel (calcaneus) and shank (tibia) as external references to measure the relative motion between talus and tibia, it was important to find that anterior displacement values measured with the QAAT correlate well with anterior skeletal translations of talus and calcaneus over sequential cutting of ligaments, and that those correlations held over a range of loads. Therefore, it is concluded that the QAAT represents a valid test principle for anterior displacement measurements. However additional adjustments are mandatory, since the QAAT overestimates the anterior translation values of talus and calcaneus by 6.5–2.5 times and seems to underestimate the increase in anterior translation values seen after sequential cutting of the ligaments.
In a previous patient study the maximum anterior load at which laxity was determined was 150 N. This magnitude of load was determined on the basis of previous findings in literature (Kerkhoffs et al. 2001). The ideal load for testing anterior ankle joint laxity was again brought up for discussion by Tohyama et al. (2003). These authors presented a different measurement system and suggested that a large force magnitude is not indicated to detect the integrity of the ligament during an anterior drawer test. Following this line of reasoning, this could imply that the higher absolute values for anterior translation found in our patient study could be a result of a too great magnitude of the applied force. Therefore, loading cycles for the measurements in this in-vitro study were restricted from 0 to 100 N and displacement values were calculated at 25, 50 and 100 N. However, large translations persisted. The translations measured with the QAAT are also high when compared to values described in literature (Kerkhoffs et al. 2001). The laxity values as determined from the actual skeletal translation of the talus are within the range of the values reported in other studies at any given load (Fig. 5). A number of possible error sources may explain the overestimation of the anterior translation by the QAAT. Movements of soft tissues at shank and heel and movements in adjacent joints may have contributed to the high QAAT values. Also fixation of the lower leg in the tester is a possible source for the introduction of errors: the displacement transducer at the shank was placed 15 cm proximally from the point at the heel, so the extra translation measured by the QAAT may have been due to the placement of the transducers. An error source that hampers the comparisons between experiments is the uncertainty of determining the reference position in the unloaded joint. Because of the low stiffness around this neutral position, a small variation of 5 N can cause a difference of several millimetres in the QAAT measurement. This effect may mask the actual differences in translation values between joints (Edixhoven et al. 1989). In the current experiments the specimen remained in the tester during the all measurements and the zero force at which the reference point was calculate was the same for the QAAT and Optotrak measurements. This means that with in-vivo measurements the validity of the QAAT to detect differences between joints will be lower than in the current experiment.

Scatter diagrams showing actual anterior laxity values of the talus for a given applied load. The values found in the current study are presented in the range of values reported in other studies (Kerkhoffs et al. 2005b). The values are reported for intact and ligament deficient ankles
Due to the high absolute laxity values, the subtle increase in anterior displacement caused by ligament damage, as seen with the skeletal motion of the talus, cannot be measured with great accuracy by the QAAT.
The principal finding of the present study was that the QAAT presents a valid test principle, however needs serious adjustments for clinical practice in order to minimize the errors.
Conclusions
The differences in skeletal translations and rotations between the talus and calcaneus are small during an anterior drawer movement of the ankle joint.
Anterior skeletal translation of the talus and calcaneus show fair correlation with the anterior displacements measurements of the QAAT. These QAAT measurements show a 2.5–6.5 times overestimation of the laxity value irrespective of the load applied.
For future use in clinical practice, the current prototype of the QAAT requires technical adaptations to ensure a measurement that more closely follows the actual skeletal motions.
References
Allinger TL, Engsberg JR (1993) A method to determine the range of motion of the ankle joint complex, in vivo. J Biomech 26(1):69–76
Almquist PO, Arnbjörnsson A, Zätterström R, Ryd L, Ekdahl C, Fridén T (2002) Evaluation of an external device measuring knee joint rotation: an in vivo study with simultaneous Roentgen stereometric analysis. J Orthop Res 20:427–432
Brantigan JW, Pedegana LR, Lippert FG (1977) Instability of the subtalar joint: diagnosis by stress tomography in three cases. J Bone Joint Surg (A) 59:321–324
Crawford NR, Yamaguchi GT, Dickman CA (1996) Methods for determining spinal flexion/extension, lateral bending and axial rotation from marker coordinate data: analysis and refinement. Hum Mov Sci 15:55–78
van Dijk CN, Mol BW, Lim LS, Marti RK, Bossuyt PM (1996) Diagnosis of ligament rupture of the ankle joint. Physical examination, arthrography, stress radiography and sonography compared in 160 patients after inversion trauma. Acta Orthop Scand 6:566–570
Edixhoven P, Huiskes R, de Graaf R (1989) Anteroposterior drawer measurements in the knee using an instrumented test device. Clin Orthop 247:232–242
Fujii T, Luo Z-P, Kitoaka HB, An K-N (2000) The manual stress test may not be sufficient to differentiate ankle ligament injuries. Clin Biomech 15:619–623
Ishii T, Miyagawa S, Fukubayashi T, Hayashi K (1996) Subtalar stress radiography using dorsiflexion and supination. J Bone Joint Surg (B) 78:56–60
Jorn LP, Fridén T, Ryd L, Lindstrand A (1998) Simultaneous measurement of sagital knee laxity with an external device and radiostereometric analysis. J Bone Joint Surg (B) 80:169–172
Kannus P, Renström P (1991) Current concept review. Treatment for acute tears of the lateral ligaments of the ankle. J Bone Joint Surg (A) 73:305–312
Kerkhoffs GM (2005) Acute lateral ankle ligament injury; new insights in diagnosis and treatment. Thesis. University of Amsterdam, The Netherlands
Kerkhoffs GM, Blankevoort L, van Poll D, Marti RK, van Dijk CN (2001) Review. Anterior lateral ankle ligament damage and anterior talocrural-joint laxity: an overview of in-vitro reports in literature. Clin Biomech 16:635–643
Kerkhoffs GM, Blankevoort L, Sierevelt IN, Corvelein R, Janssen GH, van Dijk CN (2005a) Two ankle joint laxity testers: reliability and validity. Knee Surg Sports Traumatol Arthrosc 13:699–705
Kerkhoffs GM, Blankevoort L, van Dijk CN (2005b) A measurement device for anterior laxity of the ankle joint complex. Clin Biomech 20:218–222
Klenerman L (1998) Editorial. The management of sprained ankle. J Bone Joint Surg (B) 80:11–12
Louwerens JW, Ginai AZ, van Linge B, Snijders CJ (1995) Stress radiography of the talocrural and subtalar joints. Foot Ankle Int 16:148–155
Sammarco J (1977) Biomechancs of the ankle, I: surface velocity and instant rotation in the sagital plane. Am J Sports Med 5:231–234
Siegler S, Wang D, Plasha E, Berman AT (1994) Technique for in-vivo measurement of the three-dimensional kinematics and laxity characteristics of the ankle joint complex. J Orthop Res 12:421–431
Tohyama H, Yasuda K, Ohkoshi Y, Beynnon BD, Renström PA (2003) Anterior drawer test for acute anterior talofibular ligament injuries of the ankle. How much load should be applied during the test? Am J Sports Med 31:226–232
Verhagen RA, de Keizer G, van Dijk CN (1995) Long-term follow-up of inversion trauma of the ankle. Arch Orthop Trauma Surg 114:92–96
Acknowledgment
Authors thank D. van Poll for his assistance with the experiments and thank I. Sierevelt for her assistance with statistical analyses.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kerkhoffs, G., Blankevoort, L., Kingma, I. et al. Three-dimensional bone kinematics in an anterior laxity test of the ankle joint. Knee Surg Sports Traumatol Arthrosc 15, 817–824 (2007). https://doi.org/10.1007/s00167-006-0169-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-006-0169-8