
Abstract
The posterior cruciate ligament (PCL) avulsion fracture from its tibial insertion is a very rare condition in children. An isolated avulsion fracture of PCL in a child and its repair by open reduction and internal fixation with a screw is reported.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The posterior cruciate ligament (PCL) avulsion fracture from its tibial insertion is a rare condition in children. Very few cases in children were reported in the literature [4–6]. We report on one patient with an isolated avulsion fracture of PCL from its tibial insertion, which was repaired by open reduction and internal fixation with a screw, and his 7 year follow-up until his proximal tibial physis was closed.
Case report
A 13-year-old boy was admitted with left knee pain and swelling after a fall from a bicycle. He described twisting his leg when falling, and hitting the anterior aspect of the proximal tibia. On physical examination, hemarthrosis, and tenderness on the joint line in the middle of the popliteal fossa were present. Because of pain and swelling, the knee could not be examined appropriately. Radiographic examination showed an isolated avulsion and elevation of the tibial attachment of the PCL (Fig. 1). The MRI examination confirmed the lesion, and other pathologies such as meniscal or chondral lesions were excluded (Fig. 2).

Lateral radiograph of PCL avulsion

MRI view of avulsed PCL
Under general anesthesia, the posterior drawer sign was (++) positively confirmed. Then, the patient was rolled over to prone position. Through a posterior S shaped incision the capsule was exposed. After incision of the capsule, which was partially torn, the avulsed fragment of PCL was displayed. The fragment was reduced easily and fixed with one 3.5 mm cancellous screw directed parallel to the physeal line (Fig. 3). The wound was closed per premium over a suction drain, and the lower extremity put in a long leg brace in 30° of flexion.

Early postoperative AP/Lat radiographs
Postoperatively, in the postoperative first 6 weeks, no weight bearing was allowed, and range of motion (ROM) exercises between 30 and 45° were initiated. For the next 2 weeks partial weight bearing was allowed with the brace on, and ROM exercises advanced to 30–90°. After 8 weeks, the brace was removed, and full ROM and weight bearing were allowed. At the 7 year follow-up the patient has full pain free ROM (S: 0-0-135), and there was no leg length discrepancy (Fig. 4). There was no instability or laxity. At the follow-up, the IKDC score of the patient was 87.3. The patient did not have any restriction or complaints on daily and sport activities.

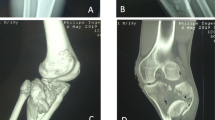
About 7 year follow-up radiographs showing the closed physis
Discussion
Posterior cruciate injuries are very rare in children. Few avulsion fractures of PCL have been reported in the literature [4–6]. In our case, the diagnosis was made radiologically because of swelling and pain in the knee. As noted in the literature, diagnosis with physical examination may be difficult and radiographic or MR imaging are often needed.
In PCL avulsion fractures, if the fragment is undisplaced, the result of non-surgical treatment is satisfactory. If the fragment is displaced, however, surgical treatment is advised [7]. In a recent report, arthroscopic repair is reported with successful outcomes. In children, there are not enough clear guidelines to decide between surgical or non-surgical treatment. We preferred surgical treatment because of the displacement of the avulsed fragment. Exposure and open surgical technique were easy as noted in the literature [3]. Arthroscopy may be used to confirm and diagnose other intra-articular pathologies if suspected.
There are very few cases of open reduction and screw fixation of PCL avulsion fracture in the literature [1–7]. None has follow-up until the physis is closed. Our case has a long-term follow-up for 7 years with an excellent clinical outcome. So, we suggest open reduction and screw fixation as a safe and successful technique of treating PCL avulsion fractures in children with open physes.
References
Choi NH, Kim SJ (1997) Arthroscopic reduction and fixation of bony avulsion of the posterior cruciate ligament of the tibia. Arthroscopy 13(6):759–762
Deehan DJ, Pinczewski LA (2001) Arthroscopic reattachment of an avulsion fracture of the tibial insertion of the posterior cruciate ligament. Arthroscopy 17(4):422–425
Dhillon MS, Singh HP, Nagi ON (2003) Posterior cruciate ligament avulsion from the tibia: fixation by a posteromedial approach. Acta Orthop Belg 69(2):162–167
Goodrich A, Ballard A (1988) Posterior cruciate ligament avulsion associated with ipsilateral femur fracture in a 10-year-old child. J Trauma 28(9):1393–1396
Quintart C, Elbaum R (1999) A case of isolated avulsion fracture of the posterior cruciate ligament in a child. Rev Chir Orthop Reparatrice Appar Mot 85(6):617–620
Ross AC, Chesterman PJ (1986) Isolated avulsion of the tibial attachment of the posterior cruciate ligament in childhood. J Bone Joint Surg 68-B:747–748
Yang CK, Wu CD, Chih CJ, et al (2003) Surgical treatment of avulsion fracture of the posterior cruciate ligament and postoperative management. J Trauma 54(3):516–519
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ugutmen, E., Sener, N., Eren, A. et al. Avulsion fracture of the posterior cruciate ligament at the tibial insertion in a child: a case report. Knee Surg Sports Traumatol Arthrosc 14, 340–342 (2006). https://doi.org/10.1007/s00167-005-0706-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-005-0706-x