
Abstract
We reviewed 164 consecutive cases (158 patients) of arthroscopic examinations for lateral meniscal variants during the last 10 years. We classified lateral meniscal variants into four types by arthroscopic appearance, into six tear patterns by modifying O’Connor’s classification, and compared magnetic resonance images (MRI) with arthroscopic findings. Regarding the four types, 131 cases were complete, 25 cases were incomplete, 4 cases were Wrisberg, and 4 cases were ring-shaped meniscus. The six tear patterns were as follows: 33 simple horizontal, 21 combined horizontal, 37 longitudinal, 27 central, 14 complex, and 12 radial tear. Among the 31 knees with a central tear or ring-shaped meniscus, we reviewed 25 MR images. Fifteen (60%) MRI findings were interpreted to represent a bucket-handle (displaced) tear of the normal C-shaped meniscus; 7(28%) MRI findings, a discoid meniscal tear; and the remaining 3(12%) MRI findings, a simple meniscal tear. Moreover, all ring-shaped menisci were interpreted as a displaced lateral meniscal tear on the MRI findings. Twelve patients (13 knees, 7.9%) had osteochondritis dissecans: Nine patients (10 knees) of them had a central tear, two patients (2 knees) of them had a simple horizontal tear of the discoid meniscus, and one patient (1 knee) had a ring-shaped meniscus. Twenty three patients (92.6%) with a central tear of the discoid meniscus did not have any traumatic events. For the differential diagnosis of a central tear or a ring-shaped meniscus from a bucket-handle tear of the normal C-shaped meniscus, we should take a careful history, in particular any traumatic events, we should also consider the possibility of misinterpreting the MR images though these images can provide additional information about associated abnormalities and probe carefully in the arthroscopic operations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Lateral meniscal variants include several pathologic entities, which vary with respect to size, shape, and attachment. Such variability is likely due to multifactorial origins with probable congenital and developmental influences. The most common lateral meniscal variant is the discoid meniscus. Other anomalies of the lateral meniscus such as a ring-shaped lateral meniscus are relatively rare. In a review of 20 published reports of lateral meniscal variants, it was found that most of these reports [1, 2, 5, 6, 24] except for a few [3, 8, 18] have focused on only a limited age group (mostly children). Also these studies had a small number of cases in their reports. We, however, meet patients of diverse age groups in our actual practice.
The purpose of this study was to classify lateral meniscal variants into the four types based on arthroscopic appearance, into six tear patterns by modifying O’Connor’s [19] classification in a large number of cases comprehensively, and to compare MR images with arthroscopic findings.
Materials and methods
We reviewed 164 consecutive cases (158 patients) of arthroscopic examinations performed by the senior author (K.H.S) at one institute for lateral meniscal variants between September 1993 and September 2003 for 10 years. During the same period, 1,221 arthroscopic operations were performed because of symptoms attributable to the meniscus or other structures of the knee. Among them, 164 (13.4%) knees had lateral meniscal variants whether torn or not. Also, 510 arthroscopic meniscal resections were performed in the same period, 144 (28.2%) meniscal resections of them were done due to lateral meniscal variants.
There were 83 males (85 knees) and 75 females (79 knees) and the average age was 27.9±13.1 years (range, 3–59 years). Ninety-one (55.5%, 87 patients) knees were affected in the second or the third decade. The age distributions are presented in Table I. Eighty-one patients were affected in the right knee, 71 patients were affected in the left knee, and six patients were affected in the bilateral knee. The operative findings were recorded and collected in a standard, predetermined format by a single surgeon (K.H.S.), even though this was a retrospective study.
Based on the detailed arthroscopic photographs and operation records, we classified the lateral meniscal variants into four types (Fig. 1) by modifying the Watanabe’s [23] classification such as complete, incomplete, Wrisberg, and ring-shaped meniscus (Fig. 2).

Schematic drawings of the modified Watanabe’s classification for lateral meniscal variants: a a complete meniscus, b an incomplete meniscus, c a Wrisberg meniscus, and d ring-shaped meniscus

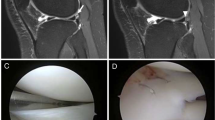
a–c A ring-shaped lateral meniscus without any sign of a tear on an arthroscopy (a), the MR images of coronal (b) and sagittal (c) views show an unusual shape of the lateral meniscus, mimicking a bucket-handle tear of the C-shaped lateral meniscus
For the tear pattern, we modified the O’Connor’s [19] classification of meniscal tears to classify the variable tear patterns into six simple and comprehensive categories (Fig. 3): (1) a simple horizontal tear; (2) a combined horizontal tear, in which the major tear component is horizontal and another tear component is accompanied according to Bin et al. [3]; (3) a longitudinal tear including peripheral tear; (4) a radial tear including a oblique and a flap tear; (5) a complex tear including a degenerative tear, which is a combination of two major components except a horizontal tear or a combination of three or more major tear components including a horizontal tear; and (6) a central tear (Fig. 4), which is a broad spectrum of the wear in the central portion of the discoid meniscus as a result of repeated maceration. We regarded as a central tear from wearing of superior or inferior surface to a central perforation without other major tear component. The extent of the meniscal resection was dependent on the tear pattern and symptoms, which consisted of a partial, a subtotal, a total menisectomy and a simple diagnostic arthroscopy without a menisectomy. We reviewed the MRI findings of the central tear of the discoid meniscus, and the ring-shaped meniscus which were diagnosed by an arthroscopy, and reviewed any traumatic histories.

Schematic drawings of the modified O’Connor’s classification for lateral discoid meniscal tears: a a simple horizontal, b a combined horizontal, c a longitudinal, d a radial, e a complex, and f a central tear

a–c A central tear has irregular or degenerative inner margin which is not tapered and sharp (a), the MR images of coronal (b) and sagittal (c) views show the presence of a redundant meniscus centrally placed within a joint which implies a displaced meniscal tear such as a bucket-handle tear of the C-shaped lateral meniscus
Results
From the classification of the four types based on arthroscopic appearance, 131 (79.9%) cases were complete, 25 (15.2%) cases were incomplete, 4 (2.4%) cases were Wrisberg type, and 4 (2.4%) cases were ring-shaped meniscus. Among 164 knees, 144 (87.8%) knees had a meniscal tear and 20(12.2%) knees had no tear. The six tear patterns were as follows: 33(20.1%) simple horizontal, 21(12.8%) combined horizontal, 37(22.6%) longitudinal, 27(16.5%) central, 14(8.5%) complex, and 12(7.3%) radial tear. Table 2 presented tear patterns according to the types of lateral meniscal variant.
For the extent of a meniscal resection with or without meniscal repairs, the types of surgery performed were 77(47%) subtotal menisectomies, 43(26.2%) partial menisectomies, 24 (14.6%) total menisectomies, and 20 (12.2%) diagnostic arthroscopy without a menisectomy.
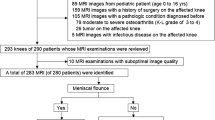
Among the 29 patients (31 cases) with a central tear (27 cases) or a ring-shaped meniscus (4 cases), we reviewed 25 MR images of 23 patients who took it. Only seven (accuracy = 28%) MRI findings were interpreted to represent a discoid meniscal tear. On the other hand, 18 (72%) MRI findings were misinterpreted to represent a bucket-handle (displaced) tear (15 findings) of the normal C-shaped lateral meniscus or a simple tear (3 findings) of normal C-shaped lateral meniscus. Moreover, all ring-shaped menisci were misinterpreted as a bucket-handle tear of a normal C-shaped lateral meniscus of the MRI findings.
For the traumatic histories, 23 patients (25 knees, 92.6%) with a central tear did not have any specific traumatic events and only two patients (2 knees, 7.4%) experienced trauma: One individual collided with a person during a soccer game 2 years ago and the other collided with a motorcycle 15 years ago. Seventy-eight (78 knees, 96.3%) of 81 patients (81 knees), however, who were diagnosed with a bucket-handle tear from an arthroscopic operation during the same index period experienced specific traumatic events from playing soccer, basketball, and being in a traffic accident with anterior cruciate ligament rupture. They recall the trauma that occurred with pinpoint accuracy. The other three (3.7%) patients who could not describe their traumatic events complained of intermittent pain, swelling, and locking from 5 years to 10 years ago.
One of the four patients with a ring-shaped meniscus was discovered during a posterior cruciate ligament reconstructive surgery incidentally and the other three patients with a ring-shaped meniscus were transferred to our department with recurring pain at the lateral aspect of the affected knee. All patients with a ring-shaped meniscus had no traumatic history.
For associated injuries, 12 patients (13 knees, 7.9%) had osteochondritis dissecans; nine (10 knees) of them had a central tear, two patients (2 knees) had a simple horizontal tear, and the remaining one patient (1 knee) had a ring-shaped meniscus. Nine patients (9 knees) had a anterior cruciate ligament tear and two patients (2 knees) had an posterior cruciate ligament tear.
Discussion
The normal lateral meniscus is more morphologically variable than the medial meniscus and the most common lateral meniscal variant is the discoid meniscus. Other anomalies of the lateral meniscus such as ring-shaped lateral meniscus are relatively rare. Since the publication of Watanabe’s Atlas [23], three types of lateral meniscal abnormalities have been generally accepted. He classified a discoid meniscus according to morphological basis into complete, incomplete, and Wrisberg type meniscus. Several recent descriptions [11, 14] of a ring-shaped lateral meniscus, however, could be evidence of another type. Monllau et al. [14] described the existence of a fourth meniscal malformation variant, characterized by a ring-shaped morphology with a normal posterior tibial attachment. The authors agree with the existence of this fourth meniscal variant and four (2.4%) knees had a ring-shaped meniscus in our study.
The reported prevalence of discoid lateral meniscus varies, depending on the method of investigation, the selection criteria, and the patient population. Discoid lateral meniscus, however, is not a rare disease entity in far eastern countries such as Korea and Japan. Reported prevalence in western countries is 0.7%–5.2% [4, 15, 16, 24], while the prevalence in Korea and Japan has been reported to be between 15.2% and 16.6% [3, 8, 18]. In our clinic, the prevalence was 13.4%, which was confirmed by arthroscopic examinations incidentally or symptomatically. The proportion of Wrisberg type meniscus has been reported to be between 0% and 33% [6, 8, 10, 12, 20–22] and we found four patients (4 knees, 2.4%) with it. For bilateral occurrence, Bellier et al. [2] reported 20% of patients with a discoid meniscus, Bin et al. [3] reported 4.9%, and our result was 3.8% (six patients).
Our classification of tear patterns is more comprehensive and simpler than that of original O’Connor’s. The longitudinal tear includes a peripheral tear, the radial tear includes a flap and an oblique tear. When the horizontal tear was accompanied by another tear component, extent of meniscal resection depended mainly upon the latter according to Bin et al. [3]; hence we subdivided horizontal tears into simple and combined horizontal tear groups. Also, we proposed a new tear pattern, which we called ‘central tear’ and there were 27(16.5%) central tears in our study. We believe that the central tear pattern has been neglected because it is difficult and confusing to distinguish it from a ring-shaped meniscus, in particular, a displaced meniscal tear like a bucket-handle tear of the C-shaped lateral meniscus which we meet quite often in our practice. In our experience, 54 knees (32.9%) had a horizontal tear component (33 simple, 21 combined), which was the most common. The distribution of the tear pattern has been reported in several studies [3, 6, 8, 21]. Smillie [21] stated that a horizontal cleavage was the most common type of tear of a discoid meniscus. Bin et al. [3] stated that 36% (39 of 108 cases) of patients had a horizontal tear component that was the most common type.
The ring-shaped meniscus is abnormally circular in shape, which has also been found in animals other than humans [10] and usually at the lateral meniscus [7, 10, 11, 14, 17]. The inner portion of the ring-shaped menisci was the same as that of the normal menisci with a sharp and tapering inner margin, and was not mobilized when we tried to move the medial portion within an intercondylar notch with a probe toward the lateral side. These are what make our cases different from the bucket handle tear or central tear. On the other hand, the central tear has an irregular or degenerative circular inner margin that is not tapered and sharp. We regarded a central tear as one from the wear of a superior or inferior surface by repeated maceration to the central perforation without any other major tear component. For a bucket-handle tear of the C-shaped lateral meniscus, the displaced meniscal portion within the intercondylar notch is usually movable and reducible into lateral portion of the meniscus and we are able to observe the detached portion from the lateral joint capsule.
In interpreting the MRI, it is important to keep in mind the possibility of a ring-shaped meniscus or central tear in a differential diagnosis of a displaced meniscal tear. The presence of a redundant meniscus centrally placed within a joint in the MRI usually implies a displaced meniscal tear such as a bucket-handle tear of the C-shaped lateral meniscus. Usually, patients with a bucket-handle tear have experienced traumatic events. We reviewed 81 consecutive cases and most of them (96.3%) experienced specific traumatic events. On the other hand, 23 patients (92.6%) with a central tear had no traumatic event.
The association of osteochondritis dissecans in the lateral femoral condyle with a torn discoid lateral meniscus in children was first described by Irani et al. [9]. Since then, Aichroth et al. [1] found seven knees with osteochondritis dissecans affecting the lateral femoral condyle in 62 knees with a lateral discoid meniscus injury in 52 children under 18 years of age. Mitsuoka et al. [13] studied the clinical features of osteochondritis dissecans affecting the lateral femoral condyles and noted that all patients in their series were in the growing period and had a damaged lateral discoid meniscus. In our study, twelve patients (13 knees, 7.9%) had osteochondritis dissecans, which was associated with ten central tears, one ring-shaped meniscus, and two simple horizontal tears. Unlike the above-mentioned cases, there were three children under 18 years of age in our cases, however, repetitive abnormal stress associated with a central tear might be a cause of osteochondritis dissecans of the lateral femoral condyle in adults as well as in the growing period.
In summary, it is difficult and confusing to distinguish a ring-shaped meniscus or central tear of the discoid meniscus from a bucket handle tear of the C-shaped lateral meniscus. For the differential diagnosis of them, we should take a careful history, in particular, any traumatic event. We should also consider the possibility of misinterpreting the MRI, though these images can provide additional information about associated abnormalities. Finally, we should carefully probe in the arthroscopic operations.
References
Aichroth PM, Patel DV, Marx CL (1991) Congenital discoid lateral meniscus in children. A follow-up study and evolution of management. J Bone Joint Surg Br 73:932–936
Bellier G, Dupont JY, Larrain M, Caudron C, Carlioz H (1989) Lateral discoid menisci in children. Arthroscopy 5:52–56
Bin SI, Kim JC, Kim JM, Park SS, Han YK (2002) Correlation between type of discoid lateral menisci and tear pattern. Knee Surg Sports Traumatol Arthrosc 10:218–222
Dickhaut SC, DeLee JC (1982) The discoid lateral-meniscus syndrome. J Bone Joint Surg Am 64:1068–1073
Fujikawa K, Iseki F, Mikura Y (1981) Partial resection of the discoid meniscus in the child’s knee. J Bone Joint Surg Br 63:391–395
Hayashi LK, Yamaga H, Ida K, Miura T (1988) Arthroscopic meniscectomy for discoid lateral meniscus in children. J Bone Joint Surg Am 70:1495–1500
Hong CN (1999) A ring-shaped lateral meniscus. Am J Knee Surg 12:109–110
Ikeuchi H (1982) Arthroscopic treatment of the discoid lateral meniscus. Technique and long-term results. Clin Orthop Relat Res 167:19–28
Irani RN, Karasick D, Karasick S (1984) A possible explanation of the pathogenesis of osteochondritis dissecans. J Pediatr Orthop 4:358–360
Kaplan EB (1957) Discoid lateral meniscus of the knee joint: nature, mechanism and operative treatment. J Bone Joint Surg Am 39:77–87
Kim SJ, Jeon CH, Koh CH (1995) A ring-shaped lateral meniscus. Arthroscopy 11:738–739
Middleton DS (1936) Congenital disc-shaped lateral meniscus with snapping knee. Br J Surg 24:246–255
Mitsuoka T, Shino K, Hamada M, Horibe S (1999) Osteochondritis dissecans of the lateral femoral condyle of the knee joint. Arthroscopy 15:20–26
Monllau JC, Leon A, Cugat R, Ballester J (1998) Ring-shaped lateral meniscus. Arthroscopy 14:502–504
Nathan PA, Cole SC (1969) Discoid meniscus. A clinical and pathologic study. Clin Orthop 64:107–113
Neuschwander DC, Drez D Jr, Finney TP (1992) Lateral meniscal variant with absence of the posterior coronary ligament. J Bone Joint Surg Am 74:1186–1190
Noble J (1975) Congenital absence of the anterior cruciate ligament associated with a ring meniscus. J Bone Joint Surg Am 57:1165–1156
Seong SC, Park MJ (1992) Analysis of the discoid meniscus in Koreans. Orthopedics 15:61–65
Shahriaree H (1992) O’Conner’s textbook of arthroscopic surgery. Lippincott, Philadelphia, pp 318–321
Silverman JM, Mink JH, Deutsch AL (1989) Discoid menisci of the knee: MR imaging appearance. Radiology 173:351–354
Smillie IS (1948) The congenital discoid meniscus. J Bone Joint Surg Br 30:671–682
Vandermeer RD, Cunningham FK (1989) Arthroscopic treatment of the discoid lateral meniscus: results of long-term follow-up. Arthroscopy 5:101–109
Wadanabe M, Takeda S, Ikeuchi H (1974) Atlas of arthroscopy, 3rd edn. Igaku Shoin, Tokyo, pp 87–91
Washington ER III, Root L, Liener UC (1995) Discoid lateral meniscus in children. Long-term follow-up after excision. J Bone Joint Surg Am 77:1357–1361
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, YG., Ihn, JC., Park, SK. et al. An arthroscopic analysis of lateral meniscal variants and a comparison with MRI findings. Knee Surg Sports Traumatol Arthrosc 14, 20–26 (2006). https://doi.org/10.1007/s00167-005-0629-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-005-0629-6