
Abstract
Purpose
Cardiopulmonary bypass induces an ischaemia–reperfusion injury and systemic inflammatory response, which contributes to low cardiac output syndrome following cardiac surgery. Exogenous nitric oxide during cardiopulmonary bypass has shown potential to ameliorate such injury. We undertook a large randomised controlled trial to investigate the clinical effects of administering nitric oxide to the cardiopulmonary bypass circuit in children.
Methods
After written informed consent, children were randomised to receive 20 ppm nitric oxide to the gas inflow of the cardiopulmonary bypass oxygenator, or standard conduct of bypass.
Results
101 children received nitric oxide and developed low cardiac output syndrome less frequently (15 vs. 31 %, p = 0.007) than the 97 children who did not receive nitric oxide. This effect was most marked in children aged less than 6 weeks of age (20 vs. 52 %, p = 0.012) and in those aged 6 weeks to 2 years (6 vs. 24 %, p = 0.026), who also had significantly reduced ICU length of stay (43 vs. 84 h, p = 0.031). Low cardiac output syndrome was less frequent following more complex surgeries if nitric oxide was administered (17 vs. 48 %, p = 0.018). ECMO was used less often in the nitric oxide group (1 vs. 8 %, p = 0.014).
Conclusions
Delivery of nitric oxide to the oxygenator gas flow during paediatric cardiopulmonary bypass reduced the incidence of low cardiac output syndrome by varying degrees, according to age group and surgery complexity.
Clinical Trial Registration: ACTRN12615001376538.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
There is a predictable drop in cardiac output following cardiac surgery and cardiopulmonary bypass (CPB) in children [1]. The clinical picture associated with this fall in cardiac output, low cardiac output syndrome (LCOS), delays recovery and is associated with significant morbidity and mortality [2, 3]. Attenuation of this phenomenon could have significant implications for clinical outcome.
Surgery with CPB induces a generalized inflammatory response, triggered partly by ischaemia–reperfusion injury [4]. This inflammatory response contributes to myocardial dysfunction and reduced cardiac output. Nitric oxide (NO) has a complex role in the regulation of acute inflammation [5] and has been the focus of multiple clinical trials since its discovery in 1987 [6]. NO is a regulator of apoptosis [7], inhibits platelet adhesion and aggregation [8], monocyte adherence and migration [9] and generation of oxygen free radicals [10]. There is evidence of NO inhibition during cardiac surgery, and administration of the NO precursor l-arginine during surgery may improve NO bioavailability, with consequent improvement in cardiovascular function [11]. Administration of NO or an NO donor ameliorates injury in experimental models of ischaemia–reperfusion of the kidney, liver, lung [12] and brain [13]. NO is a common effector molecule in multiple approaches to cardioprotection [14], mediating such effects through multiform cellular and subcellular interactions. Exogenous NO administered during experimental ischaemia and reperfusion reduces markers of myocardial injury and decreases infarct size [15, 16].
Two small clinical studies have explicitly pursued the idea that NO delivery during CPB might limit myocardial injury. Gianetti and colleagues demonstrated that inhaled NO during and after adult CPB diminished serum markers of myocardial damage [17]. In 16 children undergoing tetralogy of Fallot repair, Checchia and colleagues reported a reduction in serum markers of inflammation and myocardial injury, and shorter mechanical ventilation and ICU stay in patients who had NO delivered to the CPB circuit [18].
To further investigate these potential clinical benefits we undertook a large, single-centre randomised controlled trial of NO delivery to the CPB oxygenator in children undergoing cardiac surgery. Results have been presented at the American Heart Association Scientific Sessions 2015, and published in abstract form [19].
Methods
All children undergoing cardiac surgery with CPB at our institution from 1 January to 31 December 2014 were eligible. Exclusion criteria were administration of inhaled NO immediately prior to surgery or emergency surgery. Sample size was determined with 80 % power to detect a 40 % reduction in LCOS with a significance level of 0.05. Assumptions for the control group and treatment effect were based on data reported by Checchia and colleagues [18].
The study was approved by, and prospectively registered with, the institutional human research ethics committee (HREC 33112B). Subsequent to completion, the study was registered with the Australia and New Zealand Clinical Trials Registry (ACTRN12615001376538). Consent was obtained from parents or guardians of participants. Patients were randomised into two groups: NO group (NO added to the oxygenator gas inflow at 20 ppm throughout CPB) and control group (standard conduct of CPB).
Randomisation and blinding
Randomisation was performed just before surgery by the treating perfusionist. Randomisation was stratified by age, corrected for gestation if younger than 6 months postnatal age (<6 weeks, 6 weeks–2 years, >2 years) in blocks of six to ensure balanced allocation in each group. Sequentially ordered randomisation cards were generated by the institutional clinical epidemiology and biostatistics unit, stored in opaque envelopes and opened immediately before surgery. The perfusionist alone was unblinded and was responsible for NO delivery. Equipment and devices were identical, with opaque draping of CPB and NO circuits to maintain allocation blinding to all other operating room staff.
NO delivery
CPB devices included a Maquet HL-30 heart–lung machine and HCU-30 heater-cooler. (Maquet, Hirrlingen, Germany). A Terumo Fx05 or Fx15 oxygenator (Terumo Corporation, Tokyo, Japan) was used, depending on weight. For a blood prime, the reservoir was primed with 500 ml Plasmalyte148 (Baxter Healthcare, Australia), 100 ml sterile water, 100 ml 20 % albumin, 2500 IU heparin, 25 mmol Na2CO3 and 2.5 mmol CaCl2. Donor packed red blood cells (approximately 250 ml) were added to the prime, warmed to 32 °C and haemofiltered to a total prime volume of 300 ml. In greater than 10 kg, the blood component was replaced with proportionally more Plasmalyte148 and other circuit additives.
A minimum sweep gas flow of 2.5 l/min was used in all patients, regardless of study group, with CO2 added or sweep flow increased to maintain PaCO2 35–40 mmHg. This minimum flow was necessary to ensure complete NO mixing and accurate delivery of 20 ppm in NO group patients. NO was blended into the CPB gas administration line upon initiation of CPB, via an Ikaria INOmax DSIR (Ikaria, NJ, USA), with continuous sampling of NO and NO2 concentration from a port just prior to the oxygenator. In all patients, sweep gas FiO2 was 0.9–0.6, depending on temperature, aiming for PaO2 450–550 mmHg. Blood gases were monitored continuously (CDI, Terumo Cardiovascular, MD, USA) and measured intermittently, along with co-oximetry, every 30 min. Administration of NO or additional CO2 was not recorded on the perfusion record.
Data collection
Arterial lactate, central venous saturation (ScvO2) and vasoactive inotropic score (VIS) [20] were recorded on ICU admission (time 0) and at 3, 6, 12, 24 and 48 h.
Blood loss was recorded for the first 24 post-operative hours and blood product administration for the first 48 h. Information pertaining to the entire ICU stay included duration of mechanical ventilation; use of inhaled NO (iNO), peritoneal dialysis and ECMO; cardiac arrest; duration of ICU stay and mortality.
Primary outcome
The primary outcome was LCOS, defined as any of the following at any time during the first 48 h:
-
Lactate >4 mmol/l and ScvO2 <60 % (or SaO2–ScvO2 difference >35 % in single ventricle) [21]
-
VIS ≥ 10
-
ECMO.
Secondary outcomes
Secondary outcome measures were use of iNO, use of peritoneal dialysis, delayed sternal closure, blood loss, blood product transfusion, duration of mechanical ventilation, length of ICU and hospital stay.
Statistical analysis
Analyses were performed using Stata v13.1 (StataCorp, College Station, TX, USA). Patient characteristics were summarised for each group. A test of two proportions was used to assess evidence of a difference between the proportion of children with LCOS in each group. Primary outcome subgroup analyses were performed by age group and surgical risk. No adjustments were made for multiple comparisons. Secondary outcomes were compared between groups using Chi squared, Fisher’s exact or Mann–Whitney U tests as appropriate, for the full sample and by age subgroups. Additional clinical parameters were described separately for those who were diagnosed with LCOS and those who were not.
Results
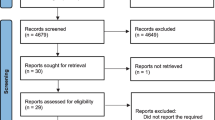
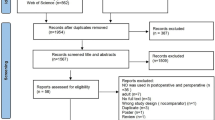
During the study period 490 congenital cardiac operations were performed using CPB. A total of 198 children were enrolled: 101 in the NO group and 97 in the control group (Fig. 1). Groups were well matched with respect to complexity of surgery and duration of CPB and cross-clamp times (Table 1). No patient had deep hypothermic circulatory arrest. Peak methaemoglobin was higher in the NO group (0.6 vs. 0.3 g/dl, p < 0.001). No patient received perioperative corticosteroid. Operations performed are categorised in Supplementary Table 1.

CONSORT flow diagram of enrolment, allocation, follow-up and analysis
Primary outcome
Fewer patients in the NO group developed LCOS in the first 48 post-operative hours than in the control group (15 vs. 31 %, p = 0.007) (Table 2). The effect was most marked in children aged less than 6 weeks (20 vs. 52 %, p = 0.012), those aged 6 weeks to 2 years (6 vs. 24 %, p = 0.026) and following more complex surgeries (17 vs. 48 %, p = 0.018) (Table 3).
The NO group had a reduced incidence of LCOS at almost every time point (Fig. 2). Most children who developed LCOS were diagnosed on admission to ICU and any child who developed LCOS did so within 12 h (Supplementary Fig. 1).

Incidence of LCOS
Most patients with LCOS (89 %) had high inotrope requirement. No patient was diagnosed with LCOS solely because of high lactate and low ScvO2 (Supplementary Table 2).
The proportion of patients requiring ECMO support was an important difference between the groups. Nine patients received ECMO during the 48 h following surgery (one NO, eight control). Eight of these were younger than 6 weeks. Five had ECMO initiated in the operating theatre because of inability to safely wean from CPB. Four patients with refractory LCOS were cannulated in ICU, within 12 h of admission, none of whom suffered a cardiac arrest.
Two ECMO patients died before discharge from ICU.
Secondary outcomes
There were no differences in duration of ventilation, ICU stay or hospital stay between groups (Table 2). NO group patients received iNO less often than the control group (3 vs. 12 %, p = 0.015). iNO was initiated in the operating theatre or within 4 h of admission to ICU to treat pulmonary hypertension or poor oxygenation in all but one case (control group), where NO was initiated 1 month after ICU admission. There was no difference between groups in the amount of bleeding in the first 24 h. Seventeen patients had delayed sternal closure (eight NO, nine control). Sixteen were admitted with an open sternum; the remaining patient had emergency chest opening after 24 h because of refractory LCOS.
Secondary outcomes by age group are shown in Supplementary Table 3. In patients aged 6 weeks to 2 years, ICU stay was shorter in the NO group (43 vs. 84 h, p = 0.031). There was a trend toward fewer transfusions in patients over 2 years old (8 vs. 24 %, p = 0.096).
Consequences of LCOS
Patients with LCOS more frequently received peritoneal dialysis (51 vs. 16 %, p < 0.001) and iNO (30 vs. 1 %, p < 0.001), and had a longer period of mechanical ventilation (72 vs. 18 h, p < 0.001), ICU stay (144 vs. 46 h, p < 0.001) and hospital stay (17 vs. 8 days, p < 0.001) compared to patients without LCOS (Fig. 3).

Implications of LCOS
Adverse events
No cardiac arrests occurred during the 48-h post-operative period. There were three later cardiac arrests, each with successful return of circulation. No deaths occurred during the 48-h post-operative period. Four patients (control group) died before ICU discharge, 2 weeks to 2 months after surgery (bidirectional cavopulmonary shunt, hypoplastic left heart syndrome; rhabdomyoma removal with Norwood procedure; hypoplastic aortic arch and ventricular septal defect (VSD) repair; tetralogy of Fallot repair with hypoplastic pulmonary arteries).
Discussion
This prospective randomised controlled trial showed that administration of NO to the CPB oxygenator in children undergoing cardiac surgery reduced the incidence of post-operative LCOS. This effect was most marked in children younger than 2 years or undergoing complex surgery. This finding, consistent with smaller studies suggesting a beneficial clinical effect of NO administration during CPB, may have important implications for future practice.
Paediatric cardiac surgical mortality is low, necessitating the use of surrogate outcome measures in interventional studies of this population. We used LCOS as the primary outcome, given its association with adverse outcomes, including mortality [3]. LCOS first occurring more than 48 h after surgery was unlikely to be directly related to the CPB and was therefore not part of the outcome of interest. The incidence of LCOS in the control group (31 % overall, 52 % neonates) is comparable to other reports [2, 22, 23]. However, these studies have defined LCOS variably. We chose to use a simple definition incorporating three important and objective features: biochemical evidence of inadequate tissue oxygen delivery, high inotrope or vasopressor requirement, or the need for ECMO. The VIS cut-off in our definition (>10) is relatively low and may have led to an over-reporting of LCOS. However, this was based on local data: 70 % of infants in our PICU following high-risk cardiac surgery have a VIS of less than 10 [24]. Study patients fulfilling this definition received more complex therapies and had a longer post-operative stay in ICU and hospital. Supplementary Table 4 shows how a higher VIS threshold for LCOS diagnosis would have affected the primary outcome; the incidence of LCOS inevitably falls, but the effect of the intervention remains significant in the youngest patients. It is important for future studies that a consensus objective definition of LCOS is agreed upon.
The reduction in LCOS was most evident in the youngest group. Our age cut-off of 6 weeks was chosen in an attempt to capture most of the high-risk neonatal operations in this group (see Supplementary Table 1). Younger children have an exaggerated inflammatory response to CPB [25] and limited cardiac reserve [26], rendering them particularly vulnerable in the post-operative period. Any intervention that might diminish inflammation and preserve myocardial function would likely preferentially benefit the youngest patients.
ECMO use, one component of our LCOS definition, was less frequent in the NO group. Post-operative ECMO is associated with an increased mortality risk: in more than 96,000 children having cardiac surgery, Mascio and colleagues reported a risk of death in patients requiring post-operative ECMO of 53.2 %, compared to 2.9 % if ECMO was not required [27]. The frequency with which ECMO was used in our study (4.5 %) is higher than the median rate (2.5 %), but within the range (0.6–9.3 %) reported by Mascio. This variation in institutional post-operative ECMO rates means that our finding of a reduction in ECMO use may not be widely replicable.
The trend toward a shorter ventilation and ICU stay in the NO group was not significant, apart from the 6 weeks to 2 years subgroup. This is at odds with the findings of Checchia, who reported reduced duration of ventilation and ICU stay in patients who received intraoperative NO [18]. The heterogeneity of surgical procedures in our study may explain these discrepant findings. In addition, both of these outcomes are readily confounded by factors other than the immediate response to CPB and surgery.
Fewer patients in the NO group received post-operative iNO, with this effect also being most evident in younger patients. Our study cannot discern whether less frequent iNO use was due to preserved pulmonary endothelial function, rather than less lung injury or better preserved right ventricular function, in the group that received NO during CPB.
Our study did not address protection from renal injury. Peritoneal dialysis is an unreliable marker of renal injury and is performed readily at our institution for fluid removal, electrolyte management, cooling and cytokine removal, particularly in neonates: more than 50 % of the youngest patients had peritoneal dialysis. A trial has been published in abstract form, reporting that NO during and after adult CPB may abrogate acute kidney injury [28]. This suggests another beneficial remote effect of NO administration during CPB and demands further investigation.
Exogenous NO can exert effects in organs and tissues remote to the site of administration. Although NO is largely inactivated rapidly in blood by binding to oxy- and deoxyhaemoglobin, there is a circulating pool of potentially bioavailable NO in relatively stable molecules [29]. Some of these can act as NO donors, including simple nitrite and S-nitrosothiols [29, 30]. During the acute inflammatory reaction to surgery and CPB, constitutive NO production is impaired [4], and levels of the NO inhibitor asymmetric dimethylarginine are increased [11]. NO supplementation by administration of l-arginine in cardioplegia solution results in less myocardial oxidative stress and better oxygen uptake [11]. Damage to red blood cells during CPB liberates haemoglobin into plasma. Stored blood contains deformed red cells, microparticles and free haemoglobin, which act as NO scavengers [31]. Exogenous NO may act to supplement reduced production and increased removal of endogenous NO. Stored red blood cells have impaired NO-synthesizing capacity [32], an important function of native red cells, which is activated by CPB [33]. This may further reduce bioavailability of NO during paediatric CPB and could help explain why NO did not affect LCOS in older children, where blood exposure was less.
Ample experimental evidence exists for NO-mediated protection from ischaemia–reperfusion injury in the heart [34] and other organs [12], and diverse cardioprotective interventions rely on NO as an essential mediator [14]. Clinical investigations report inhaled NO amelioration of injury during liver transplantation [35], cardiac surgery [17] and knee surgery [36]. Ours is the second study of NO administration directly to the CPB oxygenator in children, building on the work of Checchia and colleagues [18]. This delivery method also reduces membrane platelet consumption [37, 38] and leukocyte activation and adhesion [39], suggesting specific benefits during cardiac surgery.
Doses of NO from 20 to 80 ppm have been administered by different routes in clinical studies to ameliorate injury [17, 18, 28, 35, 36]. We chose 20 ppm on the basis of the most relevant of these studies [17, 18] and experience of this as a safe clinical dose in critically ill children. Methaemoglobin levels in the NO group confirmed safe, effective delivery of NO. Further work is required to ascertain the ideal dose under these circumstances.
There is little apparent cost-benefit from this intervention. More important cost-effective outcomes (e.g. reduction in duration of mechanical ventilation or length of stay) would need to be evident in larger studies to recommend routine use of NO. The reduction in ECMO use would also be an important consideration, if this were reproducible in other centres; paediatric cardiac ECMO costs have been reported as US$ 18–20,000 per day [40].
There are important limitations to the current study. Forty per cent of eligible patients were not included because of limited availability of a small research team. We cannot say if this influenced results, but those that were not included did not differ in age, weight or risk of surgery from the study cohort (data not shown).
For safety reasons the perfusionist was not blinded to group allocation. Although all other staff were blinded, conduct of CPB was identical in both groups and NO administration was not identified in the patient record, this is a potential source of bias. Control placebo gas has been used in trials investigating the effect of NO in the past [41]. We made a pragmatic decision not to further complicate conduct of CPB by using a control placebo gas; study patients already had an additional NO cylinder and delivery device, along with opaque draping of the entire apparatus.
Although the number of patients in the study is relatively large, this single-centre investigation is limited in its general applicability. Local practices regarding conduct of anaesthesia, CPB, surgery, ECMO deployment and post-operative care may all have influenced outcomes.
In this study we chose to focus on clinical outcomes, rather than to investigate mechanisms of protection or markers of organ injury. There is a compelling case for a larger, multicentre trial to confirm or refute our findings, and to further define which groups of patients or operative procedures might most benefit from this intervention. Although reduction in LCOS was only demonstrated in the younger cohort, there may be other effects of NO administration in older children and adults that deserve specific study. In addition, further investigations are necessary to address the means by which NO may exert remote effects, and to elucidate organ-specific effects and protective mechanisms.
Conclusions
Administration of nitric oxide to the CPB oxygenator during paediatric cardiac surgery reduced the incidence of post-operative low cardiac output syndrome. This effect was age-dependent, with the greatest effect observed in younger children. We believe that this safe and relatively simple intervention has the potential to improve short-term outcomes for children undergoing cardiac surgery. Larger studies are needed to validate these findings.
References
Wernovsky G, Wypij D, Jonas RA, Mayer JE, Hanley FL, Hickey PR, Walsh AZ, Chang AC, Castaneda AR, Newburger JW, Wesser DL (1995) Postoperative course and haemodynamic profile after the arterial switch operation in neonates and infants: a comparison of low-flow cardiopulmonary bypass and circulatory arrest. Circulation 92:2226–2235
Hoffman TM, Wernovsky G, Atz AM, Kulik TJ, Nelson DP, Chang AC, Bailey JM, Akbary A, Kocsis JF, Kaczmarek R, Spray TL, Wessel DL (2003) Efficacy and safety of milrinone in preventing low cardiac output syndrome in infants and children after corrective surgery for congenital heart disease. Circulation 107:996–1002
Ma M, Guavreau K, Allan CK, Mayer JE, Jenkins JK (2007) Causes of death after congenital heart surgery. Ann Thorac Surg 83(4):1438–1445
Paparella D, Yau TM, Young E (2002) Cardiopulmonary bypass induced inflammation: pathophysiology and treatment. An update. Eur J Cardiothorac Surg 21:232–244
Guzik TJ, Korbut R, Adamek-Guzik T (2003) Nitric oxide and superoxide in inflammation and immune regulation. J Physiol Pharmacol 54(4):469–487
Rossaint R, Lewandowski K, Zapol WM (2014) Our paper 20 years later: inhaled nitric oxide for the acute respiratory distress syndrome—discovery, current understanding, and focussed targets of future applications. Intensive Care Med 40(11):1649–1658
Uchiyama T, Otani H, Okada T, Ninomiya H, Kido M, Imamura H (2002) Nitric oxide induces caspase-dependent apoptosis and necrosis in neonatal rat cardiomyocytes. J Mol Cell Cadiol 34:1049–1061
Sawicki G, Salas E, Murat J, Miszta-Lane H, Radomski MW (1997) Release of gelatinase A during platelet activation mediates aggregation. Nature 386:616–619
Comini L, Bachetti T, Agnoletti L, Gaia G, Curello S, Milanesi B (1999) Induction of functional inducible nitric oxide synthetase in monocytes of patients with congestive heart failure: link with tumour necrosis factor-alpha. Eur Heart J 20:1503–1513
Van Dervort AL, Yan L, Madara PJ, Cobb JP, Wesley RA, Corriveau CC (1994) Nitric oxide regulates endotoxin-induced TNF-alpha production by human neutrophils. J Immunol 152:4102–4109
Zakkar M, Guida G, Suleiman MS, Angelini GD (2015) Cardiopulmonary bypass and oxidative stress. Oxid Med Cell Longev 2015:189863
Phillips L, Toledo AH, Lopez-Neblina F, Anaya-Prado R, Toledo-Pereyra LH (2009) Nitric oxide mechanism of protection in ischaemia and reperfusion injury. J Invest Surg 22(1):46–55
Godiez-Rubi M, Rojas-Mayorquin AE, Ortuno-Satiaguin D (2013) Nitric oxide donors as neuroprotective agents after ischaemic stroke related inflammatory reaction. Oxid Med Cell Longev 2013:297357. doi:10.1155/2013/297357
Jones SP, Bolli R (2006) The ubiquitous role of nitric oxide in cardioprotection. J Mol Cell Cardiol 40(1):16–23
Lin X, Huang Y, Pokreisz P, Vermeersch P, Marsboom G, Swinnen M, Verbeken E, Santos J, Pelles M, Gillijns H, Van de Wert F, Bloch K, Janssens S (2007) Nitric oxide inhalation improves microvascular flow and decreases infarction size after myocardial ischaemia and reperfusion. J Am Coll Cardiol 50(8):808–817
Nagasaka Y, Fernandez BO, Garcia-Saura MF, Petersen B, Ichinose F, Bloch KD, Feelisch M, Zapol WM (2008) Brief periods of nitric oxide inhalation protect against myocardial ischaemia-reperfusion injury. Anesthesiology 109(4):675–682
Gianetti J, Del Sarto P, Bevilacqua S, Vassalle C, De Filippis R, Kacila M, Farreti PA, Clerico A, Glauber M, Biagini A (2004) Supplemental nitric oxide and its effect on myocardial injury and function in patients undergoing cardiac surgery with extracorporeal circulation. J Thorac Cardiovasc Surg 127(1):44–50
Checchia P, Bronicki R, Muenzer J, Dixon D, Raithel S, Gandhi S, Huddleston C (2013) Nitric oxide delivery during cardiopulmonary bypass reduces postoperative morbidity in children—a randomised controlled trial. J Thorac Cardiovasc Surg 146(3):530–536
James C, Horton S, Brizard C, Molesworth C, Millar J, Butt W (2015) Nitric oxide during cardiopulmonary bypass improves clinical outcome: a blinded, randomized controlled trial. Circulation 132:A14827
Gaies M, Gurney J, Yen A, Napoli M, Gajarski R, Ohye R, Charpie J, Hirsch J (2010) Vasoactive-inotrope score as a predictor of morbidity and mortality in infants after cardiopulmonary bypass. Pediatr Crit Care Med 11:234–238
Duke T, Stocker C, Butt W (2004) Monitoring children after cardiac surgery: a minimalist approach might be maximally effective. Crit Care Res 6:306–310
Robert S, Borasino S, Dabal R, Cleveland D, Hock K, Alten J (2015) Postoperative hydrocortisone infusion reduces the prevalence of low cardiac output syndrome after neonatal cardiopulmonary bypass. Pediatr Crit Care Med 16(7):629–636
Oualha M, Urien S, Spreux-Varoquaux O, Bordessoule A, D’Agostino I, Pouard P, Treluyer JM (2014) Pharmacokinetics, haemodynamic and metabolic effects of epinephrine to prevent post-operative low cardiac output syndrome in children. Crit Care 18(1):R23
Kleiber N, de Wildt S, Cortina G, Clifford M, van Rosmalen J, van Dijk M, Tibboel D, Millar J (2016) A comparative analysis of pre-emptive versus targeted sedation on cardiovascular stability after high-risk cardiac surgery in infants. Pediatr Crit Care Med 17(4):321–331
Kozik DJ, Tweddell JS (2006) Characterizing the inflammatory response to cardiopulmonary bypass in children. Ann Thorac Surg 81(6):S2347–S2354
Bronicki RA, Chang AC (2011) Management of the postoperative pediatric cardiac surgical patient. Crit Care Med 39(8):1974–1984
Mascio CE, Austin EH, Jacobs JP, Jacobs ML, Wallace AS, He X, Pasquali SK (2014) Perioperative mechanical circulatory support in children: an analysis of the Society of Thoracic Surgeons Congenital Heart Surgery Database. J Thorac Cardiovasc Surg 147(2):658–665
Lei C, Berra L, Rezoagali E, Yu B, Strelow S, Nordio F, Bonventre J, Xiong L, Zapol W (2015) Prevention of acute kidney injury by nitric oxide during and after prolonged cardiopulmonary bypass. A double blind randomized controlled trial. Abstract presentation, American Heart Association Scientific Sessions, Orlando, Florida, Nov 2015
Rassaf T, Kleinbongard P, Kelm M (2005) Circulating NO pool in humans. Kidney Blood Press Res 28:341–348
Bhatraju P, Crawford J, Hall M, Lang JD (2015) Inhaled nitric oxide: current clinical concepts. Nitric Oxide 31(50):114–128
Liu C, Liu X, Janes J, Stapley R, Patel RP, Gladwin MT, Kim-Shapiro DB (2014) Mechanism of faster NO scavenging by older stored red blood cells. Redox Biol 10(2):211–219
Zimring JC (2015) Established and theoretical factors to consider in assessing the red cell storage lesion. Blood 125(14):2185–2190
Fischer UM, Schindler R, Brixius K, Mehlhorn U, Bloch W (2007) Extracorporeal circulation activates endothelial nitric oxide synthase in erythrocytes. Ann Thorac Surg 84(6):2000–2003
Bolli R (2001) Cardioprotective function of inducible nitric oxide synthase and role of nitric oxide in myocardial ischaemia and preconditioning: an overview of a decade of research. J Mol Cell Cardiol 33(11):1897–1918
Lang JD, Smith AB, Brandon A, Bradley KM, Liu Y, Li W, Crowe DR, Jhala NC, Cross RC, Frennette L, Martay K, Vater YL, Vitin AA, Dembo GA, DuBay DA, Bynon JS, Szychowski JM, Reyes JD, Halldorson JB, Rayhill SC, Dick AA, Bakthavatsalam R, Brandenberger J, Broeckel-Elrod JA, Sissons-Ross L, Jordan T, Chen LY, Siriussawakul A, Eckhoff DE, Patel RP (2014) A randomized clinical trial testing the anti-inflammatory effects of preemptive inhaled nitric oxide in human liver transplantation. PLoS One 9(2):e86053
Mathru M, Huda R, Solanki DR, Hays S, Lang JD (2007) Inhaled nitric oxide attenuates reperfusion inflammatory responses in humans. Anesthesiology 106(2):275–282
Keh D, Gerlach M, Kurer KJ, Gerlach H (1996) Reduction of platelet trapping in membrane oxygenators by transmembraneous application of gaseous nitric oxide. Int J Artif Organs 19(5):291–293
Mellgren K, Friberg LG, Mellgren G, Hedner T, Wennmalm A, Wadenvik H (1996) Nitric oxide in the oxygenator sweep gas reduces platelet activation during experimental perfusion. Ann Thorac Surg 61(4):1194–1198
Chello M, Mastroroberto P, Marchese AR, Maltese G, Santangelo E, Amantea B (1998) Nitric oxide inhibits neutrophil adhesion during experimental extracorporeal circulation. Anesthesiology 89(2):443–448
Harvey MJ, Gaies MG, Prosser LA (2015) US and international in-hospital costs of extracorporeal membrane oxygenation: a systematic review. Appl Health Econ Health Policy 13(4):341–357
Maitre B, Djibre M, Katsahian S, Habibi A, Stankovic Stojanovic K, Khellaf M, Bourgeon I, Lionnet F, Charles-Nelson A, Brochard L, Lemaire F, Galacteros F, Brun-Buisson C, Fartoukh M, Mekontso Dessap A (2015) Inhaled nitric oxide for acute chest syndrome in adult sickle cell patients: a randomized controlled study. Intensive Care Med 41(12):2121–2129
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding sources
None.
Conflicts of interest
WB has received payment for educational activities by Ikaria Australia.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
James, C., Millar, J., Horton, S. et al. Nitric oxide administration during paediatric cardiopulmonary bypass: a randomised controlled trial. Intensive Care Med 42, 1744–1752 (2016). https://doi.org/10.1007/s00134-016-4420-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-016-4420-6