
Abstract
Purpose
Some patients presenting with acute respiratory failure and meeting the Berlin criteria for acute respiratory distress syndrome (ARDS) lack exposure to common risk factors (CRF). These so-called ARDS mimickers often lack histological diffuse alveolar damage. We aimed to describe such ARDS mimickers lacking CRF (ARDSCRF−) in comparison with others (ARDSCRF+).
Methods
Retrospective study including all patients receiving invasive mechanical ventilation for ARDS admitted to the intensive care units (ICUs) of two tertiary care centers from January 2003 to December 2012.
Results
The prevalence of ARDSCRF− was 7.5 % (95 % CI [5.5–9.5]; n = 50/665). On the basis of medical history, bronchoalveolar lavage fluid cytology, and chest CT scan patterns, four etiological categories were identified: immune (n = 18; 36 %), drug-induced (n = 13; 26 %), malignant (n = 7; 14 %), and idiopathic (n = 12; 24 %). Although the ARDSCRF− patients had a lower logistic organ dysfunction score (4 [3–8] vs. 10 [6–13]; p < 0.0001) and less often shock upon ICU admission (44 vs. 80 %; p < 0.0001) than their counterparts, their overall ICU mortality rate was very high (66 % [46–74]), and the absence of CRF remained associated with ICU mortality by multivariable logistic regression analysis (adjusted OR = 2.06; 95 % CI [1.02–4.18]; p = 0.044). Among ARDSCRF− patients, the presence of potentially reversible lung lesions with corticosteroids (aOR = 0.14; 95 % CI [0.03–0.62]) was associated with ICU survival.
Conclusions
The absence of CRF among patients with ARDS is common and associated with a higher risk of mortality. For such atypical ARDS, a complete diagnostic workup, including bronchoalveolar lavage fluid cytology and chest CT scan patterns, should be performed to identify those patients who might benefit from specific therapies, including corticosteroids.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The recent Berlin definition of acute respiratory distress syndrome (ARDS) [1] stipulates that respiratory symptoms are to occur (or worsen) within 7 days after exposure to at least one common ARDS risk factor (CRF), classified as direct (e.g., pneumonia, gastric aspiration, etc.) or indirect (e.g., extrapulmonary sepsis, polytrauma, pancreatitis, etc.). Still, the members of the ARDS Definition Task Force anticipated that a subset of patients would have the clinical and radiological features of ARDS, while not having been exposed to any of these CRFs, and stated that an “objective assessment” of left heart filling pressures would then be required to rule out a pulmonary edema of the hydrostatic type [1].
On the other hand, it is apparent that ARDS criteria encompass a widely heterogeneous group of pathologic processes. Indeed, none of the proposed definitions of ARDS [2, 3], including the recent Berlin definition [1], appear to be fully reliable for diagnosing diffuse alveolar damage (DAD), the commonly accepted pathological hallmark of ARDS [3]. Indeed, other lesions than DAD have been reported in more than one-third of autopsied cases, including infectious pneumonia without DAD, lung fibrosis either associated with an autoimmune disease or drug-induced, organizing pneumonia, diffuse alveolar hemorrhage, lung tumoral infiltration, acute pulmonary edema, pulmonary embolism, or even the lack of histological abnormality [4]. These unusual histological entities, commonly occurring in the absence of the CRFs for ARDS, have been previously termed imitators of ARDS [5, 6]. The prevalence and the prognosis of patients fulfilling the Berlin criteria for ARDS while having no CRF have, to the best of our knowledge, not been previously assessed. The primary objective of this study was to report the prevalence and etiologies of patients developing ARDS despite no exposure to any of the common risk factors and to contrast their clinical presentation and outcomes with those of their counterparts. The secondary objective was to assess the impact of the presence of lung lesions potentially responding to therapy with corticosteroids on outcomes in the subgroup of patients with ARDS and no CRF.
Methods
Methods are further described in the online supplement.
Study design
We conducted a retrospective study including all consecutive patients presenting with ARDS [1] within 48 h of admission to the intensive care units (ICUs) of two tertiary care centers (Hôpital Tenon, Paris and Hôpital Henri Mondor, Créteil, France) from January 2003 to December 2012. This observational, non-interventional analysis of medical records was approved by the Institutional Review Board of the French Society for Respiratory Medicine. As per French law, no informed consent is required for this type of study.
Subjects, data collection, and definitions
Patients were included in the cohort when aged 18 years or older and having received invasive mechanical ventilation for management of ARDS. Exclusion criteria were previously known lung interstitial disease or tumoral infiltration; ARDS due to negative pressure pulmonary edema; left heart failure in the absence of identified CRF; mild ARDS treated with non-invasive ventilation only. ARDS was categorized as mild, moderate, or severe according to the Berlin definition [1]. Particular attention was paid to the timing criteria of the Berlin definition; as per definition, for patients not exposed to ARDS CRF, the onset of ARDS was to occur within 1 week of new or worsening respiratory symptoms [1]. ARDS patients were also classified into two groups, whether they had been exposed to any common risk factor (ARDSCRF+) or not (ARDSCRF−) (online supplement, Table 1). Patients with vasculitides were deemed to have ARDS with no CRF because vasculitides are not pathologically characterized by diffuse alveolar damage. Increase in left heart filling pressures was ruled out using transthoracic and/or transesophageal echocardiography in all ARDSCRF− patients. The ARDSCRF− patients were then separated into four etiological groups, as follows: (1) immune ARDS, including vasculitides, as defined by the American College of Rheumatology (ACR) criteria [7], and connective tissue diseases according to ACR and American Rheumatogical Association (ARA) criteria; (2) drug-induced ARDS, defined as previous exposure to a drug known as a pneumonia inducer in the absence of any other risk factor for ARDS (i.e., definite or probable drug-induced ARDS) [8]; (3) malignant ARDS, which required cytological or pathological evidence of hematologic or solid malignancy; and (4) idiopathic ARDS, defined as the absence of both CRFs and the above etiologies despite a comprehensive etiological workup.
Demographics and clinical and laboratory variables upon ICU admission, at 48 h, and during ICU stay were abstracted from the medical charts of all patients. Their initial severity was assessed using the SAPS II (Simplified Acute Physiology II) [9] and LOD (Logistic Organ Dysfunction) scores [10]. Outcome variables included the use of adjuvant therapies for ARDS (i.e., neuromuscular blocking agents, nitric oxide inhalation, prone positioning, extracorporeal membrane oxygenation), the need for hemodialysis or vasopressors, the administration of corticosteroids, the number of ventilator-free days at day 28, and ICU mortality.
The following variables were abstracted from the medical charts for ARDSCRF− patients: presence of extrapulmonary symptoms on ICU admission, bronchoalveolar lavage (BAL) fluid cytological analysis, chest CT scan patterns, and autoimmunity tests. Chest CT scan lesions were analyzed and described by a radiologist according to the Fleischner Society Glossary of Terms for Thoracic Imaging [11]. The presence of lung lesions potentially responding to therapy with corticosteroids was assessed on the basis of BAL fluid cytology and chest CT scan patterns by three experts blinded to the final diagnosis and outcome, and patients were considered as potential responders when an agreement of all three experts was met [12–14].
Data presentation and statistical analysis
Continuous variables are reported as median [25–75th percentiles] or mean (±standard deviation, SD) and compared as appropriate. Categorical variables are reported as number and percentages (95 % confidence interval) and compared as appropriate. Factors associated with ICU mortality were determined by univariable and multivariable backward logistic regression analyses, both within the whole cohort of patients (i.e., ARDSCRF+ and ARDSCRF− patients), and within the ARDSCRF− group. Independent variables with p < 0.10 in univariable analysis were included in the multivariable analysis, with backward elimination of variables displaying a p value greater than 0.05. Interactions between variables were assessed using the Mantel–Haenszel test and interaction terms introduced in the model as appropriate. Analyses were conducted using the SPSS Base 21.0 statistical software package (SPSS Inc., Chicago, IL).
Results
Prevalence of ARDS with no common risk factors
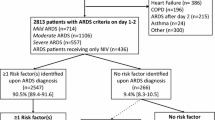
Over the 10-year study period, 812 patients were hospitalized for suspected ARDS in the two ICUs, of whom 110 met exclusion criteria, 37 received non-invasive ventilation only, and 665 remained in the study cohort (Fig. 1). In this large cohort, the prevalence of ARDS with no CRF (n = 50) was 7.5 % [5.5–9.5].

Selection of the patients included in the study. Common risk factors (CRF) for acute respiratory distress syndrome (ARDS) were adapted from the Berlin definition (1): pneumonia, gastric aspiration, pulmonary contusion, drowning, inhalation of gases, extrapulmonary sepsis, polytrauma, pancreatitis, burn, non-cardiogenic shock, drug intoxication, polytransfusion. VAP ventilator-acquired pneumonia, ILD interstitial lung disease, NPPE negative pressure pulmonary edema, CHF congestive heart failure, NIV non-invasive ventilation, ARDS CRF+ patients having ARDS with CRF, ARDS CRF− patients having ARDS with no CRF
ARDSCRF+ patients (n = 615) had been exposed to the following risk factors: pneumonia (n = 310; 50.4 % [46.0–54.0]), aspiration of gastric content (n = 214; 34.8 % [31.2–38.8]), non-pulmonary sepsis (n = 150; 24.4 % [20.6–27.4]), non-cardiogenic shock (n = 114; 18.5 % [15.0–21.0]), multiple transfusions (n = 27; 4.4 % [2.5–5.5]), drug overdose (n = 18; 2.9 % [1.7–4.3]), pulmonary contusion (n = 8; 1.3 % [0.2–1.8]), pancreatitis (n = 7; 1.1 % [0.2–1.8]), smoke inhalation (n = 2; 0.3 % [0.0–0.7]), and near-drowning (n = 1; 0.2 % [0.0–0.6]).
Outcome of patients with and without common risk factors for ARDS
As compared with ARDSCRF+ patients, ARDSCRF− patients showed a longer time from the onset of respiratory symptoms to ICU admission, were more frequently referred to the ICU for acute respiratory failure, and had lower severity scores upon ICU admission and less shock (Table 1). Overall, 360 patients (54.1 % [50.1–57.9]) died in the ICU. There was a trend toward a higher ICU mortality rate in ARDSCRF− patients, as compared with their counterparts (66.0 % [52.9–79.1] vs. 53.2 % [49.1–56.9]; p = 0.09). Among variables available within 48 h of ICU admission, the absence of common risk factors for ARDS was associated with ICU mortality (adjusted OR, aOR = 2.06; 95 % CI [1.02–4.18]) after adjusting for covariates significantly associated with mortality (online supplement, Table 2).
Etiologies and outcomes of ARDS patients with no common risk factors
The ARDSCRF− patients (n = 50) were classified into four etiological subgroups: immune ARDS (n = 18; 36 % [23–49]), drug-induced ARDS (n = 13; 26 % [14–38]), malignant ARDS (n = 7; 14 % [4–24]), and idiopathic ARDS (n = 12; 24 % [12–36]) (Table 2). When available, histopathological examination of lung tissue samples (n = 12) revealed the presence of DAD (n = 4), organizing pneumonia (n = 3), hemophagocytosis (n = 1), or cancer (n = 4) (online supplement, Table 3).
The ICU mortality of ARDSCRF− patients was 66 % (46–74) and did not differ significantly according to the four etiological subgroups (immune ARDS, 50 % [36–64]; drug-induced ARDS, 69 % [56–82]; malignant ARDS, 96 % [91–100]; idiopathic ARDS, 75 % [63–87]; p = 0.29). Corticosteroids were initiated in 100 % of the ICU survivors, as compared with 76 % of the non-survivors (Table 3). The median duration of mechanical ventilation before corticosteroid treatment initiation was 2 [1–3] days. A predominantly hemorrhagic or lymphocytic BAL fluid cytology, as opposed to a macrophagic or neutrophilic one, was associated with survival of ARDSCRF– patients (Table 3). The presence of positive ANCA tests and presence of a plasma creatinine level over 140 µmol/L were also associated with survival, consistent with the fact that patients with vasculitides exhibited a better survival than those with connective tissue diseases (1/6 vs. 8/11 died; p = 0.049). Conversely, chest CT scan abnormalities suggestive of pulmonary fibrosis tended to be associated with ICU mortality (Table 3). The three experts’ consensus considered potentially reversible lung lesions to be present in 19 patients (38 %); in multivariable analysis (Table 4), this composite variable was a protective factor for ICU mortality (aOR = 0.14; 95 % CI [0.03–0.62]). The presence of potentially reversible lung lesions was mainly associated with the presence of a lymphocytic BAL fluid, with a threshold value of lymphocyte counts over 20 %, together with the lack of signs consistent with pulmonary fibrosis (honeycombing and traction bronchiectasis) on chest CT scan (online supplement, Figs. 1 and 2).
Discussion
This study is, to the best of our knowledge, the first to report the prevalence, characteristics, management, and outcomes of patients meeting the radiological and clinical criteria of the Berlin definition of ARDS while having none of the common risk factors listed. The main results are as follows: (1) the prevalence of ARDS with no CRF was 7.5 % among a large cohort of ARDS patients requiring invasive mechanical ventilation; (2) the absence of CRF for ARDS was an independent risk factor of ICU mortality; and (3) among ARDSCRF− patients, the presence of a lung cellular inflammatory infiltration, assessed by both BAL fluid cytology and chest CT scan patterns, suggesting the potential reversibility of lung lesions with anti-inflammatory agents, was an independent predictor of survival.
Prevalence and etiologies of ARDS with no common risk factors of the Berlin definition
Our series shows that ARDS with no CRF is a frequent and peculiar condition among unselected patients with ARDS, with a prevalence of 7.5 %. This prevalence may, however, have been overestimated because our study was conducted in only two centers, one of which houses a specialized thoracic center, where the prevalence was higher than in the other. Nevertheless, our results are consistent with previous series including selected ARDS cases and reporting a high prevalence of lung histology other than DAD [15–17]. Furthermore, that both clinical and radiological definitions of ARDS correlate imperfectly with histological DAD lesions has been previously emphasized from autopsy [15], as well as lung biopsy series of ARDS [18]. Indeed, Thille et al. recently showed that 9 % of 356 patients who had died of ARDS while meeting the Berlin criteria had various pathologic features, including fibrosis, alveolar hemorrhage, or lung tumor infiltration [15]. Histological analyses from selected patients who underwent surgical lung biopsies showed even more striking results, with 60 % exhibiting other lesions than DAD [16].
Immune ARDS accounted for over one-third (36 %) of ARDSCRF− and revealed the underlying immune disease in most cases, consistent with the fact that patients having acute exacerbations of previously known interstitial lung diseases were excluded a priori. Drug-induced ARDS was the second most frequent etiology, with a predominance of chemotherapy agents incriminated. Although we may have underestimated the relative importance of this etiology by considering only cases of probable drug-induced ARDS (i.e., no established factors for ARDS except for the specific drug exposure within 1 year) [8], the overall frequency recorded in our series (2.8 %) is consistent with that recently estimated by Dhokarh et al. [8] among patients with acute lung injury (3 %). Malignant ARDS represented 14 % of ARDSCRF− and included several histological types, predominantly in situ adenocarcinoma. Finally, and although lung pathology had been obtained only for a limited number of patients, idiopathic ARDS (24 %) likely encompassed patients with acute interstitial pneumonia (DAD lesions were confirmed in 2/4 patients with idiopathic ARDS), a rare entity that was initially described as a clinical and radiological ARDS [19] with histological DAD lesions developing in spite of no exposure to any ARDS risk factor, and exhibiting a high mortality rate [20].
Outcomes of patients having ARDS with no common risk factors
Albeit consistent with the median SAPS II value on admission, the in-ICU mortality of the whole cohort (54 %) was notably higher than that reported in ARDS trials, ranging from 27 % in mild to 45 % in severe ARDS [1], likely related to differences in the case mix, with unselected and sicker patients being included in our observational study. In fact, the ICU mortality in our study was in the range of what has recently been reported in a series of ARDS patients with cancer in the 2006–2011 period (52 %) [21]. Nevertheless, our results suggest that ARDSCRF− patients may have a poorer prognosis than their counterparts. Indeed, the absence of CRF remained associated with ICU mortality after adjustment for the severity scores, age, the severity of ARDS and shock, and the absence of bacterial infection. Of note, the prolonged use of non-invasive ventilation was also independently associated with mortality, in line with previous series suggesting its potentially harmful effects in patients with de novo acute respiratory failure [22].
Early identification of ARDSCRF− patients may improve their management and outcome. Importantly, the clinical presentation of ARDSCRF− patients differed from that of other ARDS patients in several respects. First, ARDSCRF− patients exhibited a longer time between the onset of respiratory symptoms and ICU admission, with a worsening of symptoms occurring within 2 days prior to ICU admission, consistent with the timing criterion of the Berlin definition [1]. Second, the presence of shock on ICU admission was less frequent, consistent with findings from other series [23]. Together with the lack of a recognized risk factor for ARDS, these features should raise the suspicion of an unusual etiology and drive the clinician to perform a comprehensive diagnostic workup in search of etiologies potentially amenable to specific therapies [6].
In the ARDSCRF− group, ICU survival was associated with the presence of potentially reversible lung lesions, as assessed by three independent experts blinded to outcome, based on BAL cytology and chest CT scan patterns available within the first 48 h of ICU admission. Altogether, these findings suggest that ARDSCRF− patients, who exhibit a high mortality, may have better outcomes when cytological or radiological signs suggestive of lung lesions potentially responding to therapy with anti-inflammatory agents are present. Such findings are in line with observations in patients with idiopathic pulmonary fibrosis, where lung cellular infiltration scores, obtained from open lung biopsies, together with an alveolar pattern on chest CT scan (i.e., predominance of ground glass opacities) allow for predicting the response to a corticosteroid challenge [12, 24]. In contrast, in typical ARDS cases (i.e., ARDSCRF+), BAL fluid cytological analyses usually show a predominance of neutrophils [25], and chest CT scans most frequently reveal alveolar consolidations of lower lobes [26]. Last, as was recently shown, the early acquisition of a chest CT scan allows for predicting a poor outcome when lung fibrosis is present [27]. Thus, both chest CT scans and BAL fluid analysis could be important decision-making tools in this subgroup of ARDSCRF− patients, as they might help to identify which patients are more likely to benefit from specific therapies, including corticosteroids.
Surprisingly, acute renal failure, as defined by a plasma creatinine level over 140 µmol/L, was a protective factor for mortality, likely reflecting the fact that it was mainly associated with vasculitis, a condition associated with a low mortality (17 %) in the current study. However, the proportion of patients requiring hemodialysis during their ICU stay was not different between survivors and non-survivors of the ARDSCRF− group.
Study limitations
Our study has several limitations. First, we used a two-center retrospective design, which may have caused a selection bias, thereby limiting the generalizability of our findings. Indeed, we cannot exclude that some of these patients categorized as having ARDS with no CRF and exhibiting a subacute presentation (i.e., longer than 7 days) were misdiagnosed because previous respiratory symptoms could have been underestimated or neglected. Moreover, the etiologies of ARDS with no CRF could vary depending on hospital recruitment and size of the cohort. Second, important predictors of mortality related to mechanical ventilation (i.e., tidal volume, positive end-expiratory pressure level, plateau and driving pressure [28]) were not entered in the mortality analyses, because these parameters were not readily available as a result of the retrospective design and the 10-year span of the study. However, because patients included were admitted after the demonstration of a reduction in mortality with ‘protective ventilation’ [29], all patients of the current study received a standardized tidal volume of 6 mL/kg. Third, although meeting the Berlin criteria for mild ARDS if having a PaO2/FiO2 ratio less than 300 mmHg, patients who received non-invasive ventilation only were not included in the study cohort because we assumed that, because of the retrospective design of the study, ARDS might have been less well identified and reported over the study period. As a matter of fact, only 37 patients (5 % of the whole cohort) were identified as having ARDS while receiving non-invasive ventilation only. This might be explained at least in part because patients from the current study were included between 2003 and 2012, i.e., before the Berlin definition was proposed, and thus ARDS was potentially underdiagnosed in this less severe subgroup of patients. Fourth, lung histopathological specimens were obtained in only 24 % of our patients. The low number of lung biopsies (n = 5) probably reflects the concerns of intensivists regarding the risk associated with this procedure, although previous series have suggested that open lung biopsies may be well tolerated even in severe ARDS patients [17, 30]. Fifth, the small numbers of patients within each etiological ARDSCRF− subgroup may have limited our ability to show differences among clinical or laboratory features, as well as in management and outcomes. Sixth, although vasculitides were mentioned among risk factors for ARDS in the Berlin definition, we have deliberately classified patients with vasculitides within the ARDSCRF− group. Indeed, lung involvement in vasculitides is not pathologically characterized by diffuse alveolar damage but rather by diffuse alveolar hemorrhage and capillaritis, so vasculitides are usually classified as ARDS mimickers rather than common risk factor for ARDS [5, 6, 16].
We believe our work has several important clinical implications. First, we report a meaningful prevalence of so-called ARDS mimickers, having no CRF from the Berlin definition, a feature identified as an independent factor of mortality in a large cohort of unselected ARDS patients receiving invasive mechanical ventilation. Second, among the subset of ARDSCRF− patients, BAL fluid cytology and chest CT scan might help to identify a subset of patients who might benefit from specific therapies and have a better outcome. Whether early therapy with anti-inflammatory agents could decrease the mortality of ARDSCRF− patients and which patients would benefit most from this treatment need to be prospectively assessed.
References
Ranieri VM, Rubenfeld GD, Thompson BT et al (2012) Acute respiratory distress syndrome: the Berlin definition. JAMA 307:2526–2533. doi:10.1001/jama.2012.5669
Bernard GR, Artigas A, Brigham KL et al (1994) The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 149:818–824. doi:10.1164/ajrccm.149.3.7509706
Ferguson ND, Frutos-Vivar F, Esteban A et al (2005) Acute respiratory distress syndrome: underrecognition by clinicians and diagnostic accuracy of three clinical definitions. Crit Care Med 33:2228–2234
Esteban A, Fernández-Segoviano P, Frutos-Vivar F et al (2004) Comparison of clinical criteria for the acute respiratory distress syndrome with autopsy findings. Ann Intern Med 141:440–445
Schwarz MI, Albert RK (2004) “Imitators” of the ARDS: implications for diagnosis and treatment. Chest 125:1530–1535
Guérin C, Thompson T, Brower R (2014) The ten diseases that look like ARDS. Intensive Care Med. doi:10.1007/s00134-014-3608-x
Jennette JC, Falk RJ, Andrassy K et al (1994) Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum 37:187–192
Dhokarh R, Li G, Schmickl CN et al (2012) Drug-associated acute lung injury: a population-based cohort study. Chest 142:845–850. doi:10.1378/chest.11-2103
Le Gall JR, Lemeshow S, Saulnier F (1993) A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 270:2957–2963
Le Gall JR, Klar J, Lemeshow S et al (1996) The Logistic Organ Dysfunction system. A new way to assess organ dysfunction in the intensive care unit. ICU Scoring Group. JAMA J Am Med Assoc 276:802–810
Hansell DM, Bankier AA, MacMahon H et al (2008) Fleischner Society: glossary of terms for thoracic imaging. Radiology 246:697–722. doi:10.1148/radiol.2462070712
Gay SE, Kazerooni EA, Toews GB et al (1998) Idiopathic pulmonary fibrosis: predicting response to therapy and survival. Am J Respir Crit Care Med 157:1063–1072. doi:10.1164/ajrccm.157.4.9703022
Wells AU, Hansell DM, Rubens MB et al (1993) The predictive value of appearances on thin-section computed tomography in fibrosing alveolitis. Am Rev Respir Dis 148:1076–1082. doi:10.1164/ajrccm/148.4_Pt_1.1076
Terriff BA, Kwan SY, Chan-Yeung MM, Müller NL (1992) Fibrosing alveolitis: chest radiography and CT as predictors of clinical and functional impairment at follow-up in 26 patients. Radiology 184:445–449. doi:10.1148/radiology.184.2.1620845
Thille AW, Esteban A, Fernández-Segoviano P et al (2013) Comparison of the Berlin definition for acute respiratory distress syndrome with autopsy. Am J Respir Crit Care Med 187:761–767. doi:10.1164/rccm.201211-1981OC
Patel SR, Karmpaliotis D, Ayas NT et al (2004) The role of open-lung biopsy in ARDS. Chest 125:197–202
Papazian L, Doddoli C, Chetaille B et al (2007) A contributive result of open-lung biopsy improves survival in acute respiratory distress syndrome patients. Crit Care Med 35:755–762. doi:10.1097/01.CCM.0000257325.88144.30
Guerin C, Bayle F, Leray V et al (2015) Open lung biopsy in nonresolving ARDS frequently identifies diffuse alveolar damage regardless of the severity stage and may have implications for patient management. Intensive Care Med 41:222–230. doi:10.1007/s00134-014-3583-2
Katzenstein AL, Myers JL, Mazur MT (1986) Acute interstitial pneumonia. A clinicopathologic, ultrastructural, and cell kinetic study. Am J Surg Pathol 10:256–267
Olson J, Colby TV, Elliott CG (1990) Hamman-Rich syndrome revisited. Mayo Clin Proc 65:1538–1548
Azoulay E, Lemiale V, Mokart D et al (2014) Acute respiratory distress syndrome in patients with malignancies. Intensive Care Med 40:1106–1114. doi:10.1007/s00134-014-3354-0
Carrillo A, Gonzalez-Diaz G, Ferrer M et al (2012) Non-invasive ventilation in community-acquired pneumonia and severe acute respiratory failure. Intensive Care Med 38:458–466. doi:10.1007/s00134-012-2475-6
Guérin C, Reignier J, Richard J-C et al, PROSEVA Study Group (2013) Prone positioning in severe acute respiratory distress syndrome. N Engl J Med 368:2159–2168. doi:10.1056/NEJMoa1214103
Wells AU, Desai SR, Rubens MB et al (2003) Idiopathic pulmonary fibrosis: a composite physiologic index derived from disease extent observed by computed tomography. Am J Respir Crit Care Med 167:962–969. doi:10.1164/rccm.2111053
Idell S, Cohen AB (1985) Bronchoalveolar lavage in patients with the adult respiratory distress syndrome. Clin Chest Med 6:459–471
Caironi P, Carlesso E, Gattinoni L (2006) Radiological imaging in acute lung injury and acute respiratory distress syndrome. Semin Respir Crit Care Med 27:404–415. doi:10.1055/s-2006-948294
Zafrani L, Lemiale V, Lapidus N et al (2014) Acute respiratory failure in critically ill patients with interstitial lung disease. PLoS One 9:e104897. doi:10.1371/journal.pone.0104897
Amato MBP, Meade MO, Slutsky AS et al (2015) Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med 372:747–755. doi:10.1056/NEJMsa1410639
(2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med 342:1301–1308. doi: 10.1056/NEJM200005043421801
Papazian L, Thomas P, Bregeon F et al (1998) Open-lung biopsy in patients with acute respiratory distress syndrome. Anesthesiology 88:935–944
Acknowledgments
The authors thank Prof. A. Tazi for his valuable insights and help in designing the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None of the authors have conflicts of interest.
Additional information
M. Fartoukh and N. de Prost contributed equally to this work.
Take-home message: Some 7.5 % of patients meeting ARDS criteria from the Berlin definition have not been exposed to ARDS risk factors. These patients exhibit a higher risk of mortality than others.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Gibelin, A., Parrot, A., Maitre, B. et al. Acute respiratory distress syndrome mimickers lacking common risk factors of the Berlin definition. Intensive Care Med 42, 164–172 (2016). https://doi.org/10.1007/s00134-015-4064-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-015-4064-y