
Abstract
Objective
In ICU patients, abnormal liver tests are common. Markers of cholestasis are associated with adverse outcome. Research has focused on the possibility that mild hyperbilirubinemia, instead of indicating inadvertent cholestasis, may be adaptive and beneficial. These new insights are reviewed and integrated in the state-of-the-art knowledge on hepatobiliary alterations during sepsis and other critical illnesses.
Data sources
Relevant publications were searched in Medline with search terms bile, bile acids, cholestasis, critical illness, intensive care, sepsis, alone or in combination.
Data synthesis
Studies have shown that bilirubin, but also bile acids, the main active constitutes of bile, are increased in plasma of patients with critical illnesses. In particular the conjugated fractions of bilirubin and bile acids are high, indicating that during critical illness the liver is capable of converting these molecules to less toxic forms. In human liver biopsies of prolonged critically ill patients, expression of bile acid excretion pumps towards the bile canaliculi was lower, while alternative transporters towards the systemic circulation were upregulated. Remarkably, in the presence of increased circulating bile acids, expression of enzymes controlling synthesis of bile acids was not suppressed. This suggested loss of feedback inhibition of bile acids synthesis, possibly explained by the observed cytoplasmic retention of the nuclear FXR/RXR heterodimer. As macronutrient restriction during acute critical illness, an intervention that improved outcome, was found to further increase plasma bilirubin while reducing other markers of cholestasis, a potentially protective role of hyperbilirubinemia was suggested.
Conclusion
The increase in circulating levels of conjugated bile acids and bilirubin in response to acute sepsis/critical illnesses may not necessarily point to cholestasis as a pathophysiological entity. Instead it may be the result of an adaptively altered bile acid production and transport back towards the systemic circulation. How these changes could be beneficial for survival should be further investigated.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
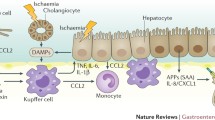
The liver plays a central role in the systemic response to sepsis and other critical illnesses by releasing acute-phase proteins, cytokines, and coagulants and by facilitating clearance of pathogenic organisms and toxins [1]. However, alterations in biochemical liver function tests are commonly observed in critically ill patients and are interpreted as signs of hepatobiliary dysfunction and cholestasis [2–4]. Two pathophysiological conditions are typically distinguished on the basis of laboratory parameters and clinical presentation: “hypoxic hepatitis” and “cholestatic liver dysfunction” [5]. Both conditions are associated with increased morbidity, mortality, and a longer hospital length of stay [2, 6–8].
Hypoxic or ischemic hepatitis is a well-recognized condition hallmarked by diffuse hepatocellular necrosis provoked by acute cellular hypoxia because of insufficient arterial blood supply of the liver. The laboratory findings reflect the underlying pathogenesis, as a steep increase of plasma alanine transaminase (ALAT) and aspartate transaminase (ASAT) and up to 20 times the upper limit of normality indicates hepatocytic damage and release of intracellular enzymes [3]. Approximately 5–10 % of the ICU patients fulfill the diagnostic criteria for hypoxic hepatitis at ICU admission [3, 9]. Mortality of patients diagnosed with hypoxic hepatitis reflects and therefore relates to the severity of the underlying condition [3]. Acute cardiac failure can cause a mixed derangement of all liver parameters (alkaline phosphatase (ALP), gamma glutamyl transpeptidase (GGT), ALAT, ASAT, and bilirubin). The most important determinants for abnormalities in liver parameters in heart failure are high central venous pressure and reduced hepatic perfusion. Comparable to hypoxic hepatitis, prognostic value was related to the extent of the underlying condition [10].
Cholestatic liver dysfunction (CLD) is traditionally defined as impaired bile formation and flow, which are caused by extrahepatic obstruction of the bile duct or by an inability of the hepatocyte to secrete bile into the bile duct (intrahepatic cholestasis). Obstructive cholestasis due to acute mechanical blockage of the canalicular system or by inflammation-driven narrowing of the bile ducts can be easily and reliably diagnosed by ultrasonography, but is seldom the cause of what is referred to as “CLD” during critical illness [11, 12]. In contrast, what is labeled CLD in critically ill patients is most often the result of non-obstructive intrahepatic alterations that may lead to accumulation of bilirubin and bile acids in the liver. In contrast with hypoxic hepatitis, clear diagnostic criteria for this type of CLD during critical illness are lacking. In fact, the criterion most often used in clinical practice is a serum total bilirubin greater than 2 or 3 mg/dl [13]. Besides the use of bilirubin as a marker, increased ALP and GGT are also used to indicate CLD, with used thresholds around 2–3 times the upper limit of normality. Up to 20 % of ICU patients develop CLD according to these diagnostic criteria, of which the majority already fulfills them upon admission to the ICU [2, 4, 9]. Risk factors are sepsis with gram-negative bacteria, but also major surgery, trauma with systemic inflammation response syndrome (SIRS), and other severe shock states [7, 14]. The occurrence of CLD during critical illness is also associated with the use of parenteral nutrition, antibiotics, and other medications [15, 16].
Although increased amounts of bile acids and bilirubin within the hepatocyte are presumed to be the culprit in inducing the clinical presentation of CLD, the underlying molecular and biochemical pathways are poorly characterized. Furthermore, whether hyperbilirubinemia during critical illness truly reflects cholestasis is not clear. Overt hyperbilirubinemia in the prolonged phase of critical illness may not be the same as a mild increase of circulating bilirubin, which is almost always observed during the acute phase of critical illnesses. In addition, many other factors can affect bilirubin such as hemolysis, blood transfusion, and (viral) infections of the liver. Furthermore, proof of causality in the link between hyperbilirubinemia and worse outcomes is still lacking. Hyperbilirubinemia might also be merely a biochemical epiphenomenon, indicative of severe hepatobiliary dysfunction, or it could reflect a transient and adaptive response during critical illness. Better insights into the pathophysiological and molecular aspects of hepatobiliary alterations during critical illness are clearly needed. In addition, the role of bile acids in the CLD that is present during critical illness has largely been overlooked, despite their known pivotal role in bile formation and in the metabolism of cholesterol and lipids [17].
The aim of this article is to review recent novel insights into the hepatobiliary transport and regulation of bilirubin and bile acids during critical illness and integrate these in the state-of-the art knowledge on this topic.
Normal hepatobiliary transport
The formation and excretion of bile is one of the key functions of the liver (Fig. 1a). Bile consists mainly of bile acids that are known for their role in dietary lipid absorption in the small intestine [18]. Bile synthesis and secretion is also important for the removal of excess cholesterol, bilirubin, and excretion of endogenous toxic compounds and xenobiotics. In the hepatocyte, primary bile acids are synthesized from their precursor molecule cholesterol by an extensive enzymatic cascade [18]. The rate-limiting enzyme CYP7A1 is regulated by multiple mechanisms and serves as the primary target in the negative feedback inhibition controlling the synthesis of bile acids [18]. The two primary bile acids produced by the liver are cholic acid (CA) and chenodeoxycholic acid (CDCA). The majority of CA and CDCA are conjugated in the liver with glycine or taurine, which enhances their physiological function. After secretion in the intestinal lumen, primary bile acids are transformed by the bacterial flora of the gut into the secondary bile acids deoxycholic acid (DCA) and litocholic acid (LCA) and their respective conjugates (Fig. 2). Secondary bile acids are absorbed in the intestinal lumen and transported to the liver, where they are reconverted to their primary form.

Hepatobiliary transport system in a normal conditions and b during critical illness. During the course of critical illness the specific uptake transporter NTCP and less specific OATP transporters are downregulated. Also the specific export pump BSEP is downregulated. MRP3 and MRP4, pumps mediating alternative export to the systemic circulation, are upregulated. Simultaneously, nuclear receptors are no longer located in the nucleus of the hepatocyte and are unable to bind to their respective response elements. NTCP Na+-taurocholate co-transporting polypeptide, OATP organic anion transporting polypeptide, BSEP bile salt export pump, MRP multidrug resistance-associated protein, FXR farnesoid X receptor, RXR retinoid X receptor alpha, PXR pregnane X receptor, VDR vitamin D receptor

Bile acid differentiation. The primary bile acids cholic acid (CA) and chenodeoxycholic acid (CDCA) are formed by the hepatocyte from their precursor molecule cholesterol. In the liver, these primary bile acids are conjugated with glycine or taurine, which improves their physiological function and decreases their toxicity. In the intestinal lumen, these primary bile acids are converted by the gut microbiome to secondary bile acids, which are efficiently reabsorbed and recycled in the enterohepatic cycle
Bile acid uptake and export transporters
The hepatocyte is a strongly polarized cell type that features specific hepatobiliary transporters for the uptake and excretion of biliary constituents from the blood compartment into the bile compartment (Table 1). Cell polarity is maintained through the presence of tight junctions and the cytoskeleton to create distinctive basolateral and apical cell membranes. Hepatic excretion of bile acids to the bile canaliculi is the rate-limiting factor in bile salt dependent bile flow. The apical excretion is mainly mediated by the bile salt export pump (BSEP) [19]. Other apical but less specific bile acid transporters are the multidrug resistance protein (MDR) and multidrug resistance-associated protein (MRP) family. MRP2 transports amphipathic conjugates (including bilirubin and bile acids), whereas MDR1 and MDR3 excrete cytotoxic agents and xenobiotics (including bile acids) [20]. Excreted bile acids are delivered to the small intestine through the bile ducts. The majority of these bile acids are efficiently reabsorbed in the enterocytes of the small intestine and transported through the portal circulation back to the liver; this overall process is known as the enterohepatic cycle. Reuptake of bile acids from the blood into the hepatocyte is mainly mediated by the high affinity Na+ dependent bile acid transporter (NTCP) and the less specific organic anion transporting polypeptide (OATP). Aside from these influx systems, the basolateral membrane expresses the export transporters MRP3 and MRP4 [21, 22]. In normal conditions, only low levels of these export transporters are expressed at the basolateral membrane of hepatocytes through which a small fraction of bile acids in the portal circulation escapes the hepatic extraction and can re-enter the systemic circulation. From the systemic circulation, bile acids can also be directly excreted by the kidneys, although highly efficient reabsorption minimizes urinary excretion, even under cholestatic conditions [23].
Regulation of bile acid homeostasis
The homeostasis of bile acids is regulated through a group of nuclear hormone receptors, a family of intracellular, ligand-dependent transcription factors [24]. In the nuclear receptor family, the farnesoid X receptor (FXR) has the highest affinity for bile acids. FXR activation leads to reduced expression of basolateral uptake transporters and stimulation of apical export transporters of bile acids, and it therefore has a self-regulating role by interfering with the intracellular concentration of its ligand. Binding of bile acids to FXR in hepatocytes also induces the expression of a small heterodimer partner (SHP) that inhibits the key enzyme CYP7A1 in bile synthesis [25, 26]. Furthermore, SHP inhibits target genes of other nuclear receptors including the expression of bile acid transporters [27]. Other nuclear receptors with bile acid affinity are the vitamin D receptor (VDR), pregnane X receptor (PXR), and constitutive androstane receptor (CAR) [28, 29]. All bile acid-sensing nuclear receptors operate in a heterodimer form with the obligatory partner retinoid X receptor alpha (RXRα) (Fig. 1a).
Because of the highly efficient reuptake system in the enterohepatic organs only a small amount of bile acids is present in the systemic circulation, although circulatory bile acids can increase 4–6 times after a meal [30]. The ingestion of meals regulates daily variation in serum bile acids concentration, although regulation by the circadian clock might also play a role [31]. These factors result in a diurnal rhythm that allows bile acids to serve as systemic metabolic signaling molecules to peripheral tissues. Indeed, circulatory bile acids have an additional important metabolic regulatory role besides their function in dietary lipid absorption and bile acid homeostasis [32–36]. These peripheral effects are mainly mediated by the nuclear receptor FXR and via the G-coupled TGR-5 receptor [32, 34, 36].
Hepatobiliary transport during critical illness
Pathophysiological manifestations of critical illness-associated CLD
Histologically, cholestatic abnormalities in the liver during critical illness are characterized by hepatocellular bilirubinostasis, sinusoidal dilatation, an increased number of infiltrating cells in the sinusoid, and Kupffer cell hyperplasia [37]. The increase in cell size from Kupffer cells in combination with infiltrating polymorphonuclear cells, eosinocytes, and platelets induces aggregate formation which can lead to obstruction of the sinusoidal lumen [37]. The resulting hypoperfusion of the sinusoid can be suspected by the presence of a dilated space of Disse. The centrilobular region is typically most affected, as it is a metabolically active region that hosts the p450 enzymes, while it has only little oxygen available [38]. In severe illness, apoptosis and necrosis of liver parenchyma can be observed [37, 39]. Besides hepatocellular bilirubinostasis, signs of bilirubinostasis can also be found in the canalicular and ductular bile ducts [40]. This phenomenon is driven by loss of contractile activity in actin and myosin microfilaments, which play a key role in the transport of bile acids trough the canalicular route [38, 41]. The impairment of polymerization and depolymerization of microfilaments results in the loss of canalicular membrane contraction and leads to bile ducts paralysis, distension, and bile secretory failure [37]. Development of such canalicular changes have been observed in septic shock patients and after long-term treatment in the ICU and are associated with severe morbidity [42, 43]. These histological findings can be accompanied by radiological abnormalities and biliary sludge, although ultrasonographic changes are also observed in patients without suspected biliary abnormalities [11, 12]. However, as explained above, presence of CLD during critical illness is mostly suspected clinically by elevated plasma bilirubin, as liver biopsies that would be required to confirm true cholestasis are hardly ever available for this indication given the invasiveness of this procedure.
Bile acid transport during critical illness
The majority of the current insights into the alterations that occur in the hepatocellular bile acid transport during critical illness are based on acute animal models challenged with pro-inflammatory agents such as LPS or cytokines. However, also limited but quite valuable data are available from studies of human patients (Fig. 1b).
In endotoxemic and septic animal studies and in critically ill humans, gene expression and protein levels of the basolateral uptake pump NTCP are markedly downregulated, likely due to suppression of essential transcription factors by pro-inflammatory cytokines [44–46]. The OATP uptake transporters are also downregulated by inflammation-induced mechanisms [45–47]. In rat endotoxemia and in LPS-treated human liver slices, a suppressed expression of the export pumps BSEP and MRP2 protein levels has been observed [48, 49]. Also in biopsies harvested immediately postmortem from critically ill patients, BSEP protein expression was dramatically reduced, whereas upregulated MRP2 gene expression was reported [45]. MDR1 and MDR3, which are involved in the export of toxic compounds to the bile canaliculi, are upregulated during critical illness in humans [45]. The most prominent changes observed in both animal and human studies are the increase in the basolateral export pumps MRP3 and MRP4 at both the transcriptional and translational level [45, 48, 50] (Fig. 3). Normally MRP3 and MRP4 are expressed at very low levels in hepatocytes, but upregulation is observed during inflammation and longstanding cholestasis, presumably shifting transport of bile acids back to the blood compartment. In human liver biopsies, MRP3 correlated strongly with histological bilirubinostasis and serum bilirubin and conjugated bile acids, suggesting that MRP3 upregulation may be a compensatory reaction to cholestasis [51].

Representative liver sections for MRP3 and MDR3. Left panel control patients, right panel ICU patients. a Normal basolateral MRP3 staining showing clear centrilobular and midzonal activity (left panel). Markedly upregulated panlobular honeycomb MRP3 staining pattern (right panel). b Normal pattern of a fine canalicular linear MDR3 staining (left panel). Strong double-stranded pattern of MDR3 staining around multiple dilated canaliculi (right panel). MRP multidrug resistance-associated protein, MDR multidrug resistance protein, CV centrilobular vein, PT portal tract. Reproduced with permission from [45]
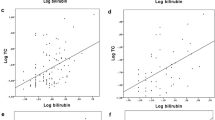
Retrospective analysis of preagonal serum from ICU non-survivors demonstrated elevated bile acid levels (11-fold) and elevated bilirubin (eightfold) levels [45]. Predominantly the conjugated forms of both bilirubin and bile acids were increased, which implies that the liver was still capable of converting these toxic compounds to their less toxic conjugated forms [45]. Despite the increased circulating levels of bile acids, hepatic protein levels of CYP7A1, which is the rate-limiting enzyme for bile acid synthesis, was not suppressed in liver biopsies from these patients [45]. The absence of a suppressed CYP71A1 protein expression in the face of quite elevated plasma bile acids suggests that the normal feedback inhibition is suppressed during critical illness, with ongoing synthesis despite increased bile acid availability.
The observed alterations in plasma bile acid levels and in the expression of hepatobiliary transporters in liver biopsies harvested immediately postmortem from human patients coincided with a remarkable decrease in the hepatocytic nuclear amount of the nuclear bile acid receptors FXR, PXR, CAR, and their obligatory partner RXR [45] (Fig. 1b). Again this is compatible with at least a partial loss of bile acid sensing and feedback regulation of de novo bile acids production that occurs during the course of critical illness. In vitro and in vivo models suggest that nuclear export of these receptors is regulated through c-Jun N-terminal kinases which can be activated by inflammatory mediators [52].
Together, these findings suggest that the so-called cholestasis, with high plasma bilirubin and bile acids, in acute critical illness is brought about by alterations in the hepatobiliary transport system. Critical illness induces an immediate increase in conjugated bile acids and bilirubin in the circulation, apparently through a reversal of the normal bile acid transport back into the blood. Furthermore, the hepatocyte of a critically ill patient appears to switch off the nuclear bile acid sensors. Whether this is a maladaptive or an adaptive response cannot be concluded from these data and should be further investigated.
Pathologies/interventions that affect CLD during critical illness
Sepsis
Sepsis and extrahepatic bacterial infection with inflammation are often accompanied by a rise in cholestatic markers [53]. A prospective analysis showed that sepsis is the second leading cause of cholestasis in clinically jaundiced patients [54]. Cholestasis in sepsis is linked predominantly to infections by gram-negative bacteria, especially with an intra-abdominal focus. In addition, pneumonia, pyelonephritis, and endocarditis have been linked to ICU jaundice [14]. Animal models of sepsis confirmed that endotoxin and inflammatory cytokines can alter the expression of the transporters for bile acids and bilirubin. Translocation of bacteria and endotoxin due to failure of the gut barrier might further enhance the altered hepatobiliary transport. Furthermore, reduced bile flow in the intestine has been suggested to augment this translocation, which might play a role in sustaining endotoxemia during the course of systemic inflammation [55]. However, similar alterations in bile acid transporter expression have been observed in an animal model of severe burn injury [51]. Furthermore, non-septic critically ill patients also display elevated plasma bilirubin levels, often already upon admission to the ICU [45, 56]. These observations suggest a more general underlying trigger as the main cause of the altered bilirubin and bile acid transport (Fig. 4).

Course and features of critical illness-associated cholestasis. The orange line represents plasma levels of bilirubin and bile acids during the course of critical illness. A steep rise in the acute phase of critical illness coincides with the burst of inflammatory cytokines as a consequence of sepsis, trauma, or severe burn injury. Additional factors that can affect markers of cholestasis are persistent or new sepsis episodes, drugs, parenteral nutrition, and hyperglycemia. In the recovery phase, bilirubin levels and bile acid are assumed to decrease to baseline levels again. BA bile acids, TPN total parenteral nutrition, ICU intensive care unit
Parenteral nutrition
Parenteral nutrition is often administered during the course of critical illness when patients cannot be fed enough macronutrients via the enteral route. However, lack of enteral feeding and the administration of lipids through parenteral nutrition are thought to contribute to the development of CLD during critical illness [57]. The impact of parenteral nutrition on the development of CLD during critical illness has been assessed in a third-degree burn rabbit model [51]. In this model, markers of liver damage were significantly lower in the group of animals that were fasted as compared with those that received parental nutrition [51]. Also, in this animal model, fasting during the course of illness induced a shift from unconjugated to conjugated circulating bile acids, in a higher hepatic expression of the efflux transporter MRP3 and a lower expression of FXR [51]. Markers of hepatobiliary function were also studied in a large clinical randomized controlled study of 4640 patients on the effect of early versus late initiation of parenteral nutrition on the outcome of critical illness (EPaNIC) [58]. This study showed that delaying the initiation of parental nutrition to beyond the first week of critical illness was associated with fewer infections, less organ failure, and significantly shorter duration of intensive care dependency and hospital stay [58, 59]. Biochemical markers of hepatocytic damage (maximum levels ALT) and of cholestasis (GGT, ALP) were lower in the group that did not get parenteral nutrition during the first week. In contrast, plasma bilirubin was significantly higher in this group throughout the 7-day intervention window, but it became equal to the group receiving parenteral nutrition as soon as parenteral nutrition was started in the fasting group beyond that first week [60]. These findings clearly suggest that hyperbilirubinemia during critical illness does not necessarily reflect true cholestasis. Given that those higher levels of bilirubin occurred in the group that experienced fewer complications and had better outcomes may also suggest an adaptive nature of the stress-induced rise in plasma bilirubin.
Hyperglycemia
In two randomized controlled trials assessing the impact of blood glucose control on outcome of critical illness in adults, in a context of early parenteral nutrition, an effect of preventing hyperglycemia on hepatobiliary function has been shown. Lowering blood glucose levels with insulin reduced biliary sludge and cholestasis in prolonged critical illness [9, 60–62].
Drug-induced cholestasis
Results from animal models also demonstrated that critical illness induces hepatic biotransformation and suppresses excretory function, which may account for the accumulation of not only bile acids and bilirubin but also exogenous xenobiotics [63, 64]. Drugs administered as part of the intensive care of ICU patients could therefore reflect a toxic threat to the hepatocytes. Accumulation of drugs can directly cause hepatocyte damage, but also exerts toxic accumulation of bile acids, bilirubin, and toxins by inhibition of canalicular transporters and interference with nuclear receptors [65]. Canalicular transporters form the rate-limiting step in clearance of lipophilic drugs and their metabolites by excretion along with bile. Drugs with biliary excretion contribute to the development of jaundice [66]. However, the majority of drugs are standard care in daily ICU practice. Cholestatic dysfunction is described for basically all antibiotics. Anesthetics and sedatives form another major group of commonly used drugs in the ICU associated with cholestasis. Currently, except for some specific toxins, there are no commonly used strategies available to eliminate this burden, besides discontinuation of potentially harmful drugs. Although extracorporeal liver support systems are known to reduce circulating bile acids, bilirubin, and toxins, this is not routine practice in ICU medicine.
Critical illness-induced CLD: beneficial or maladaptive?
One could speculate that the reversal of the hepatobiliary transport back to the blood could reflect an escape to cope with the inability of the hepatocyte to excrete bile acids against the concentration gradient into the bile ducts, which would thus be a protective mechanism of the hepatocyte to prevent toxicity of intracellular bile acids and bilirubin. Alternatively, ongoing bile acid production with a reversal of normal flow into the circulation can reflect an adaptive process in order to increase systemic effects of circulating bile acids and bilirubin. Indeed, bilirubin may attenuate organ damage by improving endothelial function and protecting against oxidative stress and high glucose levels [67–71]. Knockout mice lacking heme oxygenase, which is the rate-limiting factor in bilirubin production, were shown to have a higher mortality and more organ damage after induction of LPS than wild-type mice [71]. In an animal model of LPS-induced sepsis, bilirubin-treated rats had significantly lower expression of markers of hepatocyte damage and showed improved survival [70]. The protective role of bilirubin was shown to be, at least in part, mediated by inhibiting hepatic iNOS expression [70]. Another investigated mechanism in which bilirubin reduced cellular damage is redox cycling. Bilirubin can react with reactive oxygen species (ROS), which neutralizes the toxicity and oxidizes bilirubin to biliverdin. Biliverdin can be converted back to bilirubin through biliverdin reductase. By repeating this cycle, the antioxidative and cytoprotective effect of small amounts of bilirubin is greatly amplified [69]. In addition, bile acids were shown to reduce cortisol-metabolizing enzymes in rats [72]. An association between bile acids and cortisol was later also described in critically ill patients, suggesting that an increased availability of bile acids during critical illness may explain the reduced breakdown of cortisol, thereby contributing to elevated plasma cortisol concentrations and higher cortisol availability in vital organs and tissues and thus playing a key role in the stress response [73]. Potentially, a metabolic effect of bile acids on energy metabolism could play a protective role to reduce the hypermetabolic response of acute critical illness. Indeed, bile acids can regulate glucose, cholesterol, triglyceride, and energy homeostasis and are promising novel drug targets in the treatment for metabolic diseases [33–36]. Activation of bile acid signaling pathways increases energy expenditure and prevents development of insulin resistance [74]. In addition, bile acids were shown to increase insulin secretion by inducing the production of glucagon-like peptide-1 [75]. Mildly elevated bilirubin and/or bile acids could theoretically also have a protective role in advanced liver disease. However, in these patients hyperbilirubinemia is present over a much longer time frame than observed during critical illness and the severity appears to reflect the extent of the underlying pathogenesis [76].
However, the alterations observed in the hepatocytes during critical illness not only increase levels of bilirubin and bile acids. Drugs and other xenobiotics that are administered in daily ICU practice can easily accumulate as a result of decreased bile excretion. Reduced bile flow in the intestine has also been shown to exert translocation of the gut microbiome and could play a role in sustained release of endotoxin in the systemic circulation [55]. A prolonged lack of bile acids in the intestine can cause malabsorption of lipids and vitamins. In addition, sustained molecular changes in bile acid signaling pathways can be harmful. Evidence suggests that bile acids and FXR signaling regulate cell growth and inhibit tumor genesis. Animals lacking FXR or its downstream target SHP develop hepatocellular carcinoma [77, 78]. Furthermore, high levels of conjugated bilirubin in mice induce erythrocyte cell death which could contribute to anemia [79].
Besides supportive care and interventions to prevent liver damage, no treatment options are currently available for CLD. Reducing the load of inflammatory signaling molecules to the liver microenvironment in order to decrease the need for an adaptive response may be desirable. The latter can be achieved by reducing risk factors that provoke CLD, such as prevention of hyperglycemia and avoiding the administration of parenteral nutrition during acute critical illness [9, 60]. Opioids have been suggested to attenuate the inflammatory response and sequential liver injury, but this is still being investigated in vitro and in vivo, and thus clinical evidence is currently lacking [80, 81]. Ursodeoxycholic acid (UDCA) is used in various cholestatic liver diseases and improves clinical and/or laboratory parameters [82]. There is, however, currently no evidence to support the use of UDCA in critically ill patients.
The possible protective role of mild hyperbilirubinemia during critical illness questions the relevance of assessing liver dysfunction in ICU patients exclusively via laboratory parameters and of prognosticating via organ dysfunction scores that include bilirubin (Table 2) [13, 83, 84].
Conclusion
Alterations of biochemical cholestasis markers during the course of critical illness reflect a multifactorial process involving hepatic biotransformation and altered transporter expression. The current evidence is insufficient to conclude on whether these alterations reflect true cholestasis or only indicate a biochemical epiphenomenon. Whether the hepatobiliary alterations must be interpreted as maladaptive or adaptive changes also needs to be further elucidated. Bilirubin might therefore not be the ideal marker to assess liver dysfunction as it is currently used in organ assessment scores. Only an interventional study, in which circulating bilirubin levels can be actively and directly manipulated, can answer the questions whether the mild hyperbilirubinemia that is uniformly present during acute critical illness is a beneficial response that protects against adverse outcomes. Also, in order to explore possible specific therapeutic targets, the molecular pathways involved in the pathophysiology of the different aspects of critical illness-induced CLD need to be further elucidated. The novel insight that alterations in nuclear receptors may play a key role during critical illness opens perspectives for future research and to ultimately develop better targeted strategies to improve outcome.
References
Nesseler N, Launey Y, Aninat C, Morel F, Mallédant Y, Seguin P (2012) Clinical review: the liver in sepsis. Crit Care 16:235
Kramer L, Jordan B, Druml W, Bauer P, Metnitz PGH, Austrian Epidemiologic Study on Intensive Care ASDI Study Group (2007) Incidence and prognosis of early hepatic dysfunction in critically ill patients—a prospective multicenter study. Crit Care Med 35:1099–1104
Fuhrmann V, Kneidinger N, Herkner H, Heinz G, Nikfardjam M, Bojic A, Schellongowski P, Angermayr B, Schöniger-Hekele M, Madl C, Schenk P (2011) Impact of hypoxic hepatitis on mortality in the intensive care unit. Intensive Care Med 37:1302–1310
Thomson SJ, Cowan ML, Johnston I, Musa S, Grounds M, Rahman TM (2009) ‘Liver function tests’ on the intensive care unit: a prospective, observational study. Intensive Care Med 35:1406–1411
Horvatits T, Trauner M, Fuhrmann V (2013) Hypoxic liver injury and cholestasis in critically ill patients. Curr Opin Crit Care 19:128–132
Henrion J (2012) Hypoxic hepatitis. Liver Int 32:1039–1052
Brienza N, Dalfino L, Cinnella G, Diele C, Bruno F, Fiore T (2006) Jaundice in critical illness: promoting factors of a concealed reality. Intensive Care Med 32:267–274
Harbrecht BG, Zenati MS, Doyle HR, McMichael J, Townsend RN, Clancy KD, Peitzman AB (2002) Hepatic dysfunction increases length of stay and risk of death after injury. J Trauma 53:517–523
Mesotten D, Wauters J, Van den Berghe G, Wouters PJ, Milants I, Wilmer A (2009) The effect of strict blood glucose control on biliary sludge and cholestasis in critically ill patients. J Clin Endocrinol Metab 94:2345–2352
van Deursen VM, Damman K, Hillege HL, van Beek AP, van Veldhuisen DJ, Voors AA (2010) Abnormal liver function in relation to hemodynamic profile in heart failure patients. J Card Fail 16:84–90
Boland GW, Slater G, Lu DS, Eisenberg P, Lee MJ, Mueller PR (2000) Prevalence and significance of gallbladder abnormalities seen on sonography in intensive care unit patients. AJR Am J Roentgenol 174:973–977
Murray FE, Stinchcombe SJ, Hawkey CJ (1992) Development of biliary sludge in patients on intensive care unit: results of a prospective ultrasonographic study. Gut 33:1123–1125
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG (1996) The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 22:707–710
Trauner M, Fickert P, Stauber RE (1999) Inflammation-induced cholestasis. J Gastroenterol Hepatol 14:946–959
Grau T, Bonet A, Rubio M, Mateo D, Farré M, Acosta JA, Blesa A, Montejo JC, de Lorenzo AG, Mesejo A, Working Group on Nutrition and Metabolism of the Spanish Society of Critical Care (2007) Liver dysfunction associated with artificial nutrition in critically ill patients. Crit Care 11:R10
Lat I, Foster DR, Erstad B (2010) Drug-induced acute liver failure and gastrointestinal complications. Crit Care Med 38:S175–S187
Porez G, Prawitt J, Gross B, Staels B (2012) Bile acid receptors as targets for the treatment of dyslipidemia and cardiovascular disease. J Lipid Res 53:1723–1737
Chiang JYL (2009) Bile acids: regulation of synthesis. J Lipid Res 50:1955–1966
Kubitz R, Droge C, Stindt J, Weissenberger K, Haussinger D (2012) The bile salt export pump (BSEP) in health and disease. Clin Res Hepatol Gastroenterol 36:536–553
Alrefai WA, Gill RK (2007) Bile acid transporters: structure, function, regulation and pathophysiological implications. Pharm Res 24:1803–1823
Soroka CJ, Lee JM, Azzaroli F, Boyer JL (2001) Cellular localization and up-regulation of multidrug resistance-associated protein 3 in hepatocytes and cholangiocytes during obstructive cholestasis in rat liver. Hepatology 33:783–791
Denk GU, Soroka CJ, Takeyama Y, Chen W-S, Schuetz JD, Boyer JL (2004) Multidrug resistance-associated protein 4 is up-regulated in liver but down-regulated in kidney in obstructive cholestasis in the rat. J Hepatol 40:585–591
Lee J, Azzaroli F, Wang L, Soroka CJ, Gigliozzi A, Setchell KD, Kramer W, Boyer JL (2001) Adaptive regulation of bile salt transporters in kidney and liver in obstructive cholestasis in the rat. Gastroenterology 121:1473–1484
Glass CK, Ogawa S (2006) Combinatorial roles of nuclear receptors in inflammation and immunity. Nat Rev Immunol 6:44–55
Goodwin B, Jones SA, Price RR, Watson MA, McKee DD, Moore LB, Galardi C, Wilson JG, Lewis MC, Roth ME, Maloney PR, Willson TM, Kliewer SA (2000) A regulatory cascade of the nuclear receptors FXR, SHP-1, and LRH-1 represses bile acid biosynthesis. Mol Cell 6:517–526
Lu TT, Makishima M, Repa JJ, Schoonjans K, Kerr TA, Auwerx J, Mangelsdorf DJ (2000) Molecular basis for feedback regulation of bile acid synthesis by nuclear receptors. Mol Cell 6:507–515
Tirona RG, Kim RB (2005) Nuclear receptors and drug disposition gene regulation. J Pharm Sci 94:1169–1186
Chiang JYL (2003) Bile acid regulation of hepatic physiology: III. Bile acids and nuclear receptors. Am J Physiol Gastrointest Liver Physiol 284:G349–G356
Halilbasic E, Baghdasaryan A, Trauner M (2013) Nuclear receptors as drug targets in cholestatic liver diseases. Clin Liver Dis 17:161–189
Glicksman C, Pournaras DJ, Wright M, Roberts R, Mahon D, Welbourn R, Sherwood R, Alaghband-Zadeh J, le Roux CW (2010) Postprandial plasma bile acid responses in normal weight and obese subjects. Ann Clin Biochem 47:482–484
Ma K, Xiao R, Tseng H-T, Shan L, Fu L, Moore DD (2009) Circadian dysregulation disrupts bile acid homeostasis. PLoS One 4:e6843
Thomas C, Pellicciari R, Pruzanski M, Auwerx J, Schoonjans K (2008) Targeting bile-acid signalling for metabolic diseases. Nat Rev Drug Discov 7:678–693
Houten SM, Watanabe M, Auwerx J (2006) Endocrine functions of bile acids. EMBO J 25:1419–1425
Schaap FG, Trauner M, Jansen PLM (2014) Bile acid receptors as targets for drug development. Nat Rev Gastroenterol Hepatol 11:55–67
de Aguiar Vallim TQ, Tarling EJ, Edwards PA (2013) Pleiotropic roles of bile acids in metabolism. Cell Metab 17:657–669
Keitel V, Kubitz R, Haussinger D (2008) Endocrine and paracrine role of bile acids. World J Gastroenterol 14:5620–5629
Hirata K, Ikeda S, Honma T, Mitaka T, Furuhata T, Katsuramaki T, Hata F, Mukaiya M (2001) Sepsis and cholestasis: basic findings in the sinusoid and bile canaliculus. J Hepatobiliary Pancreatic Surg 8:20–26
Koskinas J, Gomatos IP, Tiniakos DG, Memos N, Boutsikou M, Garatzioti A, Archimandritis A, Betrosian A (2008) Liver histology in ICU patients dying from sepsis: a clinico-pathological study. World J Gastroenterol 14:1389–1393
Lysova NL, Gurevich LE, Trusov OA, Shchegolev AI, Mishnev OD (2001) Immunohistochemical characteristics of the liver in patients with peritonitis (early autopsy). Bull Exp Biol Med 132:1125–1129
Lefkowitch JH (1982) Bile ductular cholestasis: an ominous histopathologic sign related to sepsis and “cholangitis lenta”. Hum Pathol 13:19–24
Trauner M, Meier PJ, Boyer JL (1998) Molecular pathogenesis of cholestasis. New Engl J Med 339:1217–1227
Jaeger C, Mayer G, Henrich R, Gossner L, Rabenstein T, May A, Guenter E, Ell C (2006) Secondary sclerosing cholangitis after long-term treatment in an intensive care unit: clinical presentation, endoscopic findings, treatment, and follow-up. Endoscopy 38:730–734
Kulaksiz H, Heuberger D, Engler S, Stiehl A (2008) Poor outcome in progressive sclerosing cholangitis after septic shock. Endoscopy 40:214–218
Green RM, Beier D, Gollan JL (1996) Regulation of hepatocyte bile salt transporters by endotoxin and inflammatory cytokines in rodents. Gastroenterology 111:193–198
Vanwijngaerden YM, Wauters J, Langouche L, Vander Perre S, Liddle C, Coulter S, Vanderborght S, Roskams T, Wilmer A, Van den Berghe G, Mesotten D (2011) Critical illness evokes elevated circulating bile acids related to altered hepatic transporter and nuclear receptor expression. Hepatology 54:1741–1752
Andrejko KM, Raj NR, Kim PK, Cereda M, Deutschman CS (2008) IL-6 modulates sepsis-induced decreases in transcription of hepatic organic anion and bile acid transporters. Shock 29:490–496
Geier A, Dietrich CG, Voigt S, Ananthanarayanan M, Lammert F, Schmitz A, Trauner M, Wasmuth HE, Boraschi D, Balasubramaniyan N, Suchy FJ, Matern S, Gartung C (2005) Cytokine-dependent regulation of hepatic organic anion transporter gene transactivators in mouse liver. Am J Physiol Gastrointest Liver Physiol 289:G831–G841
Cherrington NJ, Slitt AL, Li N, Klaassen CD (2004) Lipopolysaccharide-mediated regulation of hepatic transporter mRNA levels in rats. Drug Metab Dispos 32:734–741
Elferink MGL, Olinga P, Draaisma AL, Merema MT, Faber KN, Slooff MJH, Meijer DKF, Groothuis GMM (2004) LPS-induced downregulation of MRP2 and BSEP in human liver is due to a posttranscriptional process. Am J Physiol Gastrointest Liver Physiol 287:G1008–G1016
Donner MG, Warskulat U, Saha N, Häussinger D (2004) Enhanced expression of basolateral multidrug resistance protein isoforms Mrp3 and Mrp5 in rat liver by LPS. Biol Chem 385:331–339
Vanwijngaerden Y-M, Langouche L, Derde S, Liddle C, Coulter S, Van den Berghe G, Mesotten D (2014) Impact of parenteral nutrition versus fasting on hepatic bile acid production and transport in a rabbit model of prolonged critical illness. Shock 41:48–54
Zimmerman TL, Thevananther S, Ghose R, Burns AR, Karpen SJ (2006) Nuclear export of retinoid X receptor alpha in response to interleukin-1beta-mediated cell signaling: roles for JNK and SER260. J Biol Chem 281:15434–15440
Geier A, Fickert P, Trauner M (2006) Mechanisms of disease: mechanisms and clinical implications of cholestasis in sepsis. Nat Clin Pract Gastroenterol Hepatol 3:574–585
Whitehead MW, Hainsworth I, Kingham JG (2001) The causes of obvious jaundice in South West Wales: perceptions versus reality. Gut 48:409–413
Clements WD, Parks R, Erwin P, Halliday MI, Barr J, Rowlands BJ (1996) Role of the gut in the pathophysiology of extrahepatic biliary obstruction. Gut 39:587–593
te Boekhorst T, Urlus M, Doesburg W, Yap SH, Goris RJ (1988) Etiologic factors of jaundice in severely ill patients. A retrospective study in patients admitted to an intensive care unit with severe trauma or with septic intra-abdominal complications following surgery and without evidence of bile duct obstruction. J Hepatol 7:111–117
Carter BA, Shulman RJ (2007) Mechanisms of disease: update on the molecular etiology and fundamentals of parenteral nutrition associated cholestasis. Nat Clin Pract Gastroenterol Hepatol 4:277–287
Casaer MP, Mesotten D, Hermans G, Wouters PJ, Schetz M, Meyfroidt G, Van Cromphaut S, Ingels C, Meersseman P, Muller J, Vlasselaers D, Debaveye Y, Desmet L, Dubois J, Van Assche A, Vanderheyden S, Wilmer A, Van den Berghe G (2011) Early versus late parenteral nutrition in critically ill adults. New Engl J Med 365:506–517
Hermans G, Casaer MP, Clerckx B, Güiza F, Vanhullebusch T, Derde S, Meersseman P, Derese I, Mesotten D, Wouters PJ, Van Cromphaut S, Debaveye Y, Gosselink R, Gunst J, Wilmer A, Van den Berghe G, Vanhorebeek I (2013) Effect of tolerating macronutrient deficit on the development of intensive-care unit acquired weakness: a subanalysis of the EPaNIC trial. Lancet Respir Med 1:621–629
Vanwijngaerden Y-M, Langouche L, Brunner R, Debaveye Y, Gielen M, Casaer M, Liddle C, Coulter S, Wouters PJ, Wilmer A, Van den Berghe G, Mesotten D (2013) Withholding parenteral nutrition during critical illness increases plasma bilirubin but lowers the incidence of biliary sludge. Hepatology ;60:202–610
Van den Berghe G, Wilmer A, Hermans G, Meersseman W, Wouters PJ, Milants I, Van Wijngaerden E, Bobbaers H, Bouillon R (2006) Intensive insulin therapy in the medical ICU. New Engl J Med 354:449–461
Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R (2001) Intensive insulin therapy in critically ill patients. New Engl J Med 345:1359–1367
Gonnert FA, Recknagel P, Hilger I, Claus RA, Bauer M, Kortgen A (2013) Hepatic excretory function in sepsis: implications from biophotonic analysis of transcellular xenobiotic transport in a rodent model. Crit Care 17:R67
Recknagel P, Gonnert FA, Westermann M, Lambeck S, Lupp A, Rudiger A, Dyson A, Carré JE, Kortgen A, Krafft C, Popp J, Sponholz C, Fuhrmann V, Hilger I, Claus RA, Riedemann NC, Wetzker R, Singer M, Trauner M, Bauer M (2012) Liver dysfunction and phosphatidylinositol-3-kinase signalling in early sepsis: experimental studies in rodent models of peritonitis. PLoS Med 9:e1001338
Yang K, Köck K, Sedykh A, Tropsha A, Brouwer KLR (2013) An updated review on drug-induced cholestasis: mechanisms and investigation of physicochemical properties and pharmacokinetic parameters. J Pharm Sci 102:3037–3057
Lammert C, Bjornsson E, Niklasson A, Chalasani N (2010) Oral medications with significant hepatic metabolism at higher risk for hepatic adverse events. Hepatology 51:615–620
Maruhashi T, Soga J, Fujimura N, Idei N, Mikami S, Iwamoto Y, Kajikawa M, Matsumoto T, Kihara Y, Chayama K, Noma K, Nakashima A, Tomiyama H, Takase B, Yamashina A, Higashi Y (2012) Hyperbilirubinemia, augmentation of endothelial function, and decrease in oxidative stress in Gilbert syndrome. Circulation 126:598–603
Castilho Á, Aveleira CA, Leal EC, Simões NF, Fernandes CR, Meirinhos RI, Baptista FI, Ambrósio AF (2012) Heme oxygenase-1 protects retinal endothelial cells against high glucose- and oxidative/nitrosative stress-induced toxicity. PLoS One 7:e42428
Baranano DE, Rao M, Ferris CD, Snyder SH (2002) Biliverdin reductase: a major physiologic cytoprotectant. Proc Natl Acad Sci USA 99:16093–16098
Wang WW, Smith DLH, Zucker SD (2004) Bilirubin inhibits iNOS expression and NO production in response to endotoxin in rats. Hepatology 40:424–433
Wiesel P, Patel AP, DiFonzo N, Marria PB, Sim CU, Pellacani A, Maemura K, LeBlanc BW, Marino K, Doerschuk CM, Yet SF, Lee ME, Perrella MA (2000) Endotoxin-induced mortality is related to increased oxidative stress and end-organ dysfunction, not refractory hypotension, in heme oxygenase-1-deficient mice. Circulation 102:3015–3022
McNeilly AD, Macfarlane DP, O’Flaherty E, Livingstone DE, Mitić T, McConnell KM, McKenzie SM, Davies E, Reynolds RM, Thiesson HC, Skøtt O, Walker BR, Andrew R (2010) Bile acids modulate glucocorticoid metabolism and the hypothalamic-pituitary-adrenal axis in obstructive jaundice. J Hepatol 52:705–711
Boonen E, Vervenne H, Meersseman P, Andrew R, Mortier L, Declercq PE, Vanwijngaerden YM, Spriet I, Wouters PJ, Vander Perre S, Langouche L, Vanhorebeek I, Walker BR, Van den Berghe G (2013) Reduced cortisol metabolism during critical illness. New Engl J Med 368:1477–1488
Watanabe M, Houten SM, Mataki C, Christoffolete MA, Kim BW, Sato H, Messaddeq N, Harney JW, Ezaki O, Kodama T, Schoonjans K, Bianco AC, Auwerx J (2006) Bile acids induce energy expenditure by promoting intracellular thyroid hormone activation. Nature 439:484–489
Katsuma S, Hirasawa A, Tsujimoto G (2005) Bile acids promote glucagon-like peptide-1 secretion through TGR5 in a murine enteroendocrine cell line STC-1. Biochem Biophys Res Commun 329:386–390
Alsatie M, Kwo PY, Gingerich JR, Qi R, Eckert G, Cummings OW, Imperiale TF (2007) A multivariable model of clinical variables predicts advanced fibrosis in chronic hepatitis C. J Clin Gastroenterol 41:416–421
Kim I, Morimura K, Shah Y, Yang Q, Ward JM, Gonzalez FJ (2007) Spontaneous hepatocarcinogenesis in farnesoid X receptor-null mice. Carcinogenesis 28:940–946
Zhang Y, Xu P, Park K, Choi Y, Moore DD, Wang L (2008) Orphan receptor small heterodimer partner suppresses tumorigenesis by modulating cyclin D1 expression and cellular proliferation. Hepatology 48:289–298
Lang E, Gatidis S, Freise NF, Bock H, Kubitz R, Lauermann C, Orth HM, Klindt C, Schuier M, Keitel V, Reich M, Liu G, Schmidt S, Xu HC, Qadri SM, Herebian D, Pandyra AA, Mayatepek E, Gulbins E, Lang F, Haussinger D, Lang KS, Foller M, Lang PA (2015) Conjugated bilirubin triggers anemia by inducing erythrocyte death. Hepatology 61:275–284
Yang LQ, Tao KM, Liu YT, Cheung CW, Irwin MG, Wong GT, Lv H, Song JG, Wu FX, Yu WF (2011) Remifentanil preconditioning reduces hepatic ischemia-reperfusion injury in rats via inducible nitric oxide synthase expression. Anesthesiology 114:1036–1047
Zhao G, Shen X, Nan H, Yan L, Zhao H, Yu J, Lv Y (2013) Remifentanil protects liver against ischemia/reperfusion injury through activation of anti-apoptotic pathways. J Surg Res 183:827–834
Beuers U (2006) Drug insight: mechanisms and sites of action of ursodeoxycholic acid in cholestasis. Nat Clin Pract Gastroenterol Hepatol 3:318–328
Zimmerman JE, Kramer AA, McNair DS, Malila FM (2006) Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today’s critically ill patients. Crit Care Med 34:1297–1310
Le Gall JR, Lemeshow S, Saulnier F (1993) A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 270:2957–2963
Acknowledgments
Funding was provided by the Methusalem Program of the Flemish Government to GVdB via the KU Leuven University (METH/08/07); by an ERC Advanced grant (AdvG-2012-321670) to GVdB from the Ideas Program of the European Union 7th Framework Program. Senior Clinical Investigator Fellowship from the Research Foundation Flanders to DM.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no conflicts of interest to disclose.
Additional information
Take-home message: During sepsis and other critical illnesses, mild hyperbilirubinemia, instead of indicating inadvertent cholestasis, may be an adaptive and beneficial response. The observed increase in circulating levels of conjugated bile acids and bilirubin may be the result of an adaptively altered bile acid production and transport back towards the systemic circulation.
Rights and permissions
About this article

Cite this article
Jenniskens, M., Langouche, L., Vanwijngaerden, YM. et al. Cholestatic liver (dys)function during sepsis and other critical illnesses. Intensive Care Med 42, 16–27 (2016). https://doi.org/10.1007/s00134-015-4054-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-015-4054-0