
Abstract
Purpose
In patients with acute respiratory distress syndrome (ARDS), extracorporeal life support (ECLS) has been utilized to support gas exchange and mitigate ventilator-induced lung injury (VILI). The optimal ventilation settings while on ECLS are unknown. The purpose of this systematic review is to describe the ventilation practices in patients with ARDS who require ECLS.
Methods
We electronically searched MEDLINE, EMBASE, CENTRAL, AMED, and HAPI (inception to January 2015). Studies included were randomized controlled trials, observational studies, or case series (≥4 patients) of ARDS patients undergoing ECLS. Our review focused on studies describing ventilation practices employed during ECLS for ARDS.
Results
Forty-nine studies (2,042 patients) met our inclusion criteria. Prior to initiation of ECLS, at least one parameter consistent with injurious ventilation [tidal volume >8 mL/kg predicted body weight (PBW), peak pressure >35 cmH2O (or plateau pressure >30 cmH2O), or FiO2 ≥0.8] was noted in 90 % of studies. After initiation of ECLS, studies reported median [interquartile range (IQR)] reductions in: tidal volume [2.4 mL/kg PBW (2.2–2.9)], plateau pressure [4.3 cmH2O (3.5–5.8)], positive end-expiratory pressure (PEEP) [0.20 cmH2O (0–3.0)], and FiO2 [0.40 (0.30–0.60)]. Median (IQR) overall mortality was 41 % (31–51 %).
Conclusions
Reduction in the intensity of mechanical ventilation in patients with ARDS supported by ECLS is common, suggesting that clinicians may be focused on reducing VILI after ECLS initiation. Future investigations should focus on establishing the optimal ventilatory strategy for patients with ARDS who require ECLS.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acute respiratory distress syndrome (ARDS) is a common cause of acute respiratory failure and is associated with substantial mortality [1–4]. While mechanical ventilation is life-saving, development of ventilator-induced lung injury (VILI) may have a detrimental effect on patient outcomes [5, 6]. While lung protective ventilation with pressure- and volume-limited strategies is associated with improved survival [7, 8], additional strategies to further mitigate VILI may be of value in facilitating lung healing.
Extracorporeal life support (ECLS) can provide gas exchange support in order to facilitate unloading of the pulmonary system [9]. ECLS can take on several configurations depending on therapeutic goals, but in patients with ARDS, these most commonly include venovenous (VV) extracorporeal membrane oxygenation (ECMO), venoarterial (VA) ECMO, or extracorporeal CO2 removal (ECCO2R) [9–11]. In addition to gas exchange support, ECLS may facilitate lung protective ventilation in patients in whom this may not have been achievable with conventional mechanical ventilation given the severity of lung injury [10, 12]. Due to extracorporeal support of gas exchange, ARDS patients may require less ventilatory support during ECLS. While some clinicians target “lung rest,” with minimal ventilator settings [13, 14], there are no evidence-based guidelines for mechanical ventilation in patients supported by ECLS. This systematic review aims to describe mechanical ventilation practices in patients with ARDS supported with ECLS and associated outcomes.
Methods
Study population
Eligible studies included any randomized controlled trials (RCTs), observational studies, or case series (≥4 patients) of adult patients (age ≥15 years) with ARDS who received any form of ECLS (VV, VA, or ECCO2R) for respiratory failure. In studies with mixed patient populations supported with ECLS [i.e., chronic obstructive pulmonary disease (COPD), cardiac failure, etc.], data were only abstracted for patients with ARDS. As a requirement for inclusion, studies needed to report on mechanical ventilation parameters used during ECLS as well as mortality. In studies reporting on ARDS patients supported on VA-ECMO, data were abstracted under the assumption that these patients required ECLS for hemodynamic support in addition to respiratory failure.
Search strategy and study selection
We electronically searched MEDLINE, EMBASE, CENTRAL, AMED, and HAPI (from inception to January 2015) to identify studies for inclusion. Our search combined Medical Subject Headings (or appropriate controlled vocabulary) and keywords for ECLS and ARDS. There were no language or date restrictions applied. Three reviewers (J.D.M., L.M., T.T.) independently reviewed all titles and abstracts for possible inclusion. Full texts were reviewed for both definite and potentially eligible studies (J.D.M., L.M., T.T.). Any disagreements were resolved by group consensus (J.D.M., L.M., T.T., M.D., E.F.).
Data extraction and study quality
A custom-designed Excel spreadsheet (Microsoft Corporation, Redmond, WA) was used to store abstracted data on study design, patient characteristics, ECLS and mechanical ventilation parameters, complications, and outcomes (T.T., J.D.M., L.M.). Actual and targeted tidal volume, plateau pressures, positive end-expiratory pressure (PEEP), and/or fraction of inspired oxygen (FiO2) following ECLS initiation were collected. Tidal volume data were abstracted only if reported in mL/kg predicted body weight (PBW). In studies where data were reported at multiple time points, we collected the data closest to 24 h following initiation of ECLS. All studies were assessed for evidence of bias using the Cochrane Collaboration risk of bias instrument [15], and we assessed study quality using the Newcastle Ottawa Scale for observational studies and Jadad Score for RCTs (Appendix 1).
Statistical analysis
Study-level data reporting on mean and median ventilator settings were summarized using median and interquartile range (IQR) and proportions as appropriate. We grouped studies describing mechanical ventilation practices in patients on VV-ECMO with studies where multiple ECLS modalities were used (labeled as mixed ECLS). Conversely, studies focusing on ECCO2R exclusively were analyzed separately in order to compare and contrast ventilator strategies between groups. A predefined sensitivity analysis was conducted in order to restrict analysis to studies conducted in the lung protective era, defined as the period following the publication of the ARDSNet ARMA study (i.e., after the year 2000). Injurious ventilation was defined as ventilation using tidal volume >8 mL/kg PBW, peak pressures >35 cmH2O, plateau pressures >30 cmH2O or FiO2 >0.80. Finally, crude mortality was analyzed according to quartiles of plateau pressure, median tidal volume, and both median tidal volume and plateau pressure in studies reporting on both parameters from studies from the lung protective ventilation era.
Results
Literature search
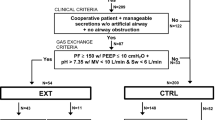
The electronic search retrieved 2,677 citations, of which 99 full texts were retrieved for further adjudication (Fig. 1). Forty-nine studies (2,042 patients) fulfilled the inclusion criteria, including 3 RCTs and 46 observational studies [13, 16–56]. Twenty-one studies (777 patients) included patients on VV-ECMO alone, 10 studies (353 patients) included patients on ECCO2R alone, and the remaining 18 studies (924 patients) included mixed configurations, in which the majority of patients (16 studies, 883 patients) were predominantly supported by VV-ECMO. Two remaining studies used both VV- and VA-ECMO (1 study, 31 patients) or both VV and ECCO2R (1 study, 10 patients) (Appendix 1). Since the use of VV-ECMO predominated in these studies, it was felt that the aim of mechanical ventilation would be similar, with the selection of a particular configuration based on patient or clinical factors (i.e., use of VA-ECMO for concomitant ARDS and circulatory shock in the setting of severe sepsis).

Flow diagram of search strategy
Baseline characteristics along with initial ECLS settings are provided in Table 1. The most common cause of ARDS was bacterial (847 patients) and viral (388 patients) pneumonia, of which the majority of viral causes were influenza A (H1N1).
Peripheral cannulation was used in the majority of cases and most commonly involved the femoral and internal jugular veins, or in the case of VA-ECMO, the femoral artery. The majority of programs (76 %) used activated clotting time (ACT) as their anticoagulation target.
Mechanical ventilation prior to initiation of ECLS
Across all studies, at least one ventilator setting was provided prior to initiation of ECLS (Table 2). Before initiation of ECLS, patients were ventilated using median (IQR) tidal volume 6.2 mL/kg PBW (5.9–6.7 mL/kg PBW), plateau pressure 32 cmH2O (30.0–33.7 cmH2O), PEEP 13 cmH2O (12.0–15.0 cmH2O), and FiO2 0.99 (0.80–1.00). Ninety percent of studies reported injurious ventilation prior to ECLS initiation. These results were similar across mixed ECLS and ECCO2R studies.
Adjunctive therapies and indications for ECLS
The use of adjunctive therapies was described in 20 studies (836 patients). Three hundred and two patients underwent prone positioning, 369 patients received inhaled pulmonary vasodilators, and 32 patients were placed on high-frequency oscillation before use of ECLS. Twenty-five studies (647 patients) specified hypoxemia to be the primary indication for initiating ECLS, 1 study (8 patients) cited hypercapnia to be the primary indication, and 10 studies (540 patients) reported both hypoxemia and hypercapnia to be the indication for ECLS.
Mechanical ventilation after initiation of ECLS
Mechanical ventilatory settings were reduced across all studies after initiation of ECLS (Table 2). Injurious ventilation decreased from 90 % (29/32 studies, 1,291 patients) to 18 % (8/44 studies, 457 patients) after ECLS initiation.
Mixed ECLS studies
Of the 39 mixed ECLS studies, 15 reported tidal volume, 16 reported plateau pressure, 32 reported PEEP, and 26 reported FiO2 following initiation of ECLS. After initiation of ECLS, 14 studies (713 patients) reported mean tidal volume ≤6 mL/kg PBW, while 7 studies (550 patients) reported mean tidal volume ≤4 mL/kg PBW. PEEP ranged between 5 and 10 cmH2O in 15 studies (705 patients), 11 and 15 cmH2O in 12 studies (586 patients), and >15 cmH2O in 5 studies (59 patients). Plateau pressure ≤30 cmH2O was observed in 13 studies (685 patients) and ≤25 cmH2O in 7 studies (332 patients).
Conversely, tidal volumes >6 mL/kg PBW were observed in only 1 study (49 patients), and plateau pressures remained >30 cmH2O in only 3 studies (89 patients). FiO2 ≥0.80 was reported in no studies after patients were placed on ECLS.
ECCO2R
Of the 10 ECCO2R studies, 4 reported tidal volume, 2 reported plateau pressure, 8 reported PEEP, and 5 reported FiO2 following initiation of ECLS. While on ECCO2R, all studies (119 patients) achieved tidal volume ≤6 mL/kg PBW and 2 studies (47 patients) targeted tidal volume ≤4 mL/kg PBW. PEEP between 10 and 15 cmH2O was reported in 3 studies (120 patients), while 5 studies (172 patients) used PEEP >15 cmH2O. Two studies (58 patients) reported plateau pressure ≤30 cmH2O while ventilating patients on ECCO2R.
Interestingly, no studies reported tidal volume >6 mL/kg PBW after ECCO2R was initiated. Only 1 study (90 patients) reported using a FiO2 ≥0.80.
Mechanical ventilation post-lung protective era
Across 33 studies (1,505 patients) published after the year 2000 [8], mechanical ventilation parameters before and after initiation of ECLS were comparable (Table 3).
Mortality
The median (IQR) mortality reported across all studies was 41 % (31–51 %). The median (IQR) mortality was similar for studies using mixed ECLS [40 % (32–50 %)] but was slightly higher when restricted to studies examining ECCO2R exclusively [51 % (27–57 %)].
When mortality was stratified according to quartiles of plateau pressure following ECLS, the lowest quartile of plateau pressure (19–22 cmH2O) was associated with a lower crude mortality [28 % (15–45 %)] as compared with the highest quartile of plateau pressure [31–36 cmH2O; mortality 46 % (45–50 %)]. Similarly, a tidal volume below the median tidal volume following ECLS initiation (≤4 mL/kg) was associated with a lower mortality [29 % (18–50 %) versus 39 % (31–47 %)] compared with those with tidal volumes >4 mL/kg. Mortality was lowest in studies which achieved a combined tidal volume ≤4 mL/kg and plateau pressure ≤26 cmH2O as compared with studies with tidal volume between 4 and 6 mL/kg and plateau pressure between 26 and 30 cmH2O [23 %(15–34 %) versus 45 % (14–49 %)] (Table 4).
Discussion
Although recommendations for ventilation strategies during ECLS [10] have been promulgated (Table 5), this is the first systematic review (49 studies, 2,042 patients) to summarize ventilation practices in patients with ARDS supported on ECLS. This review demonstrates several ways that ECLS may help to mitigate VILI in ARDS. Across these studies, potentially injurious ventilation was present in almost all studies prior to ECLS. In addition, median tidal volumes across most studies reflected an “ultra” lung protective approach of ≤4 mL/kg PBW and achievement of plateau pressures ≤30 cmH2O. We speculate that these results suggest that clinicians were unable to achieve adequate gas exchange prior to initiation of ECLS without using tidal volumes and airway pressures outside of the lung protective range. Mortality was lower in the groups of patients who had a lower intensity of applied ventilation following ECLS initiation.
While ECLS can help facilitate a reduction in ventilation intensity, optimal targets for tidal volume, plateau pressure, PEEP, and FiO2 have not been established beyond those from the ARDS Network ARMA trial [8]. Recent evidence by Hager and colleagues demonstrated a dose–response relationship between day-1 plateau pressures and mortality in patients with ARDS [58]. They showed that no “safe” threshold for plateau pressure exists, with lower plateau pressure associated with lower mortality [57]. Terragni and colleagues demonstrated ongoing tidal hyperinflation, an increase in lung inflammatory biomarkers, and a longer duration of ventilation in 33 % of patients with severe ARDS despite being ventilated with tidal volumes of 6 mL/kg PBW [58]. Increasing evidence suggests that these patients may benefit from even lower tidal volumes [56, 59], but the optimal target remains unclear. While ventilation with “ultra”-protective volumes has not demonstrated a definitive mortality benefit, it has been reported to reduce pulmonary inflammation and potentially increase ventilator-free days in patients with PaO2/FiO2 ≤150 [56, 58, 60].
Mechanical ventilation during ECLS appears to have an important impact on mortality. A study by Pham and colleagues illustrates the importance of mechanical ventilation practices in patients requiring VV ECMO for H1N1-induced ARDS [43]. It demonstrated that a lower day-1 plateau pressure following ECMO initiation was independently associated with survival and concluded that targeting “ultra”-protective tidal volumes aimed at minimizing plateau pressure may be required to improve outcome [43]. This conclusion is further corroborated by a recent review by Schmidt and colleagues, which recommends limiting tidal volume to <4 mL/kg PBW, targeting a plateau pressure <25 cmH2O, and alveolar recruitment with the use of PEEP while supporting ARDS patients on ECLS [10].
A recent international survey of centers registered with the Extracorporeal Life Support Organization (ELSO) reported on variation in ventilation practices among patients supported on ECLS for acute respiratory failure [14]. It showed that the majority of centers used a controlled mode of mechanical ventilation in order to target lung protective tidal volumes and moderate levels of PEEP. Centers responding to the survey used VV-ECMO to provide “lung rest” and preferentially weaned VV-ECMO before mechanical ventilation. Of note, 31 % of centers reported using tidal volumes <4 mL/kg PBW while ventilating patients on VV-ECMO [14]. In our review, the initiation of ECLS corresponded with an observed reduction in tidal volume and plateau pressure, although clinicians seem to have placed greater emphasis on tidal volume reductions while ventilating patients on ECLS. These findings seem to suggest that ECLS permitted a reduction in tidal volume in order to limit plateau pressures to lung protective, or even “ultra”-protective ranges. Alternatively, this may reflect a belief that tidal volume has a greater impact on mortality reduction in the setting of ARDS, though this remains controversial [61].
While PEEP and FiO2 decreased across the mixed ECLS studies, an increase in PEEP and no change in FiO2 were noted in the ECCO2R studies, reflecting the possible atelectasis that follows isolated CO2 clearance [62, 63]. In the setting of ECCO2R, application of PEEP to maintain alveolar recruitment and oxygenation is required, as ECCO2R is unable to generate sufficient blood flow to facilitate oxygenation [63]. Conversely, use of PEEP to improve oxygenation and reduce alveolar strain is not required in VV/VA-ECMO. Instead, PEEP may be used to promote lung healing by preventing pulmonary vascular leakage and macrophage activation [64–67]. In patients with severe ARDS, use of higher PEEP may be limited by high plateau pressure if sufficiently large tidal volumes are needed for adequate gas exchange. In facilitating lower tidal volumes, ECLS enables more room to apply an open lung ventilatory strategy [68]. The optimal PEEP target for patients supported on ECLS remains unclear at this point in time as no data are available to guide clinicians. More information may become available, as the impact of tidal ventilation and the optimal level of PEEP on VILI, physiological parameters, and cardiac function will be evaluated in the Strategies for Optimal Lung Ventilation during VV-ECMO for ARDS (SOLVE-ARDS) study (ClinicalTrials.gov NCT01990456).
There are several limitations to this review. First, we were able to identify only three RCTs describing ventilation strategies during ECLS [13, 52, 56]. This limited our ability to construct a meta-analysis establishing optimal ventilation targets in these patients given that these studies did not compare mechanical ventilation strategies. Since mechanical ventilation during ECLS may have important implications, our review provides a systematic summary of all of the currently available data. Next, detailed data on tidal volume in mL/kg PBW and plateau pressure were available in less than 50 % of the studies, with most studies reporting absolute tidal volume (mL) and peak inspiratory pressures. Since these values are not comparable with tidal volume (in mL/kg PBW and plateau pressure), we elected to exclude them from this analysis. Median values and interquartile ranges were used to summarize data from the studies that were included for analysis. Due to the heterogeneous design of these studies, these values should be interpreted cautiously as a general overview of the parameters described. While this review was able to separate studies examining ECCO2R exclusively, it was unable to separate patients treated with VV-ECMO and VA-ECMO to look for differences in ventilation strategy. For studies combining VV-ECMO and VA-ECMO, it is conceivable that ventilation goals were similar, but patients differed with respect to other factors (e.g., hemodynamic stability). Furthermore, the findings of this investigation would have been more informative if they included information regarding the mode of ventilation, as this can influence the achievement of ventilation targets (i.e., low plateau pressure versus low tidal volume) and weaning [9, 69–71]. Finally, the crude mortality data are likely confounded by a number of factors, and these results should be interpreted as hypothesis-generating. One could postulate that the lower mortality noted in the lower-intensity ventilation groups is because they had a less severe form of ARDS, thus allowing them to achieve lower-intensity ventilation. We feel the trend noted in the results reflecting an association between lower intensity of ventilation (beyond traditional lung protective targets) and an even lower mortality is intriguing and should be further investigated through prospective means in the context of ECLS.
References
Herridge MS, Tansey CM, Matté A et al (2011) Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med 364:1293–1304. doi:10.1056/NEJMoa1011802
Definition Task Force ARDS, Ranieri VM, Rubenfeld GD et al (2012) Acute respiratory distress syndrome: the Berlin Definition. JAMA 307:2526–2533. doi:10.1001/jama.2012.5669
Rubenfeld GD, Caldwell E, Peabody E et al (2005) Incidence and outcomes of acute lung injury. N Engl J Med 353:1685–1693. doi:10.1056/NEJMoa050333
Ferguson ND, Fan E, Camporota L et al (2012) The Berlin definition of ARDS: an expanded rationale, justification, and supplementary material. Intensive Care Med 38:1573–1582. doi:10.1007/s00134-012-2682-1
Slutsky AS, Ranieri VM (2014) Ventilator-induced lung injury. N Engl J Med 370:980. doi:10.1056/NEJMc1400293
Tremblay LN, Slutsky AS (2006) Ventilator-induced lung injury: from the bench to the bedside. Intensive Care Med 32:24–33. doi:10.1007/s00134-005-2817-8
Fan E, Needham DM, Stewart TE (2005) Ventilatory management of acute lung injury and acute respiratory distress syndrome. JAMA 294:2889–2896. doi:10.1001/jama.294.22.2889
Network ARDS (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The acute respiratory distress syndrome network. N Engl J Med 342:1301–1308. doi:10.1056/NEJM200005043421801
Del Sorbo L, Cypel M, Fan E (2014) Extracorporeal life support for adults with severe acute respiratory failure. Lancet Respir Med 2:154–164. doi:10.1016/S2213-2600(13)70197-8
Schmidt M, Pellegrino V, Combes A et al (2014) Mechanical ventilation during extracorporeal membrane oxygenation. Crit Care Lond Engl 18:203. doi:10.1186/cc13702
MacLaren G, Combes A, Bartlett RH (2012) Contemporary extracorporeal membrane oxygenation for adult respiratory failure: life support in the new era. Intensive Care Med 38:210–220. doi:10.1007/s00134-011-2439-2
Batchinsky AI, Jordan BS, Regn D et al (2011) Respiratory dialysis: reduction in dependence on mechanical ventilation by venovenous extracorporeal CO2 removal. Crit Care Med 39:1382–1387. doi:10.1097/CCM.0b013e31820eda45
Peek GJ, Mugford M, Tiruvoipati R et al (2009) Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 374:1351–1363. doi:10.1016/S0140-6736(09)61069-2
Marhong JD, Telesnicki T, Munshi L et al (2014) Mechanical ventilation during extracorporeal membrane oxygenation. An international survey. Ann Am Thorac Soc 11:956–961. doi:10.1513/AnnalsATS.201403-100BC
Higgins JPT, Altman DG, Gøtzsche PC et al (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928
Töpfer L, Menk M, Weber-Carstens S et al (2014) Influenza A (H1N1) vs non-H1N1 ARDS: analysis of clinical course. J Crit Care 29:340–346. doi:10.1016/j.jcrc.2013.12.013
Kutleša M, Novokmet A, Josipovic Mraovic R et al (2014) Extracorporeal membrane oxygenation treatment for H1N1-induced acute respiratory distress syndrome (ARDS): results of the Croatian Referral Center for Respiratory ECMO. Int J Artif Organs 37:748–752. doi:10.5301/ijao.5000356
Guervilly C, Hraiech S, Gariboldi V et al (2014) Prone positioning during veno-venous extracorporeal membrane oxygenation for severe acute respiratory distress syndrome in adults. Minerva Anestesiol 80:307–313
Chiu L-C, Tsai F-C, Hu H-C et al (2015) Survival predictors in acute respiratory distress syndrome with extracorporeal membrane oxygenation. Ann Thorac Surg 99:243–250. doi:10.1016/j.athoracsur.2014.07.064
Guirand DM, Okoye OT, Schmidt BS et al (2014) Venovenous extracorporeal life support improves survival in adult trauma patients with acute hypoxemic respiratory failure: a multicenter retrospective cohort study. J Trauma Acute Care Surg 76:1275–1281. doi:10.1097/TA.0000000000000213
Schmidt M, Stewart C, Bailey M et al (2015) Mechanical ventilation management during extracorporeal membrane oxygenation for acute respiratory distress syndrome: a retrospective international multicenter study. Crit Care Med. doi:10.1097/CCM.0000000000000753
Lee JJ, Hwang SM, Ko JH et al (2015) Efficacy of veno-venous extracorporeal membrane oxygenation in severe acute respiratory failure. Yonsei Med J 56:212–219. doi:10.3349/ymj.2015.56.1.212
Bonacchi M, Harmelin G, Peris A, Sani G (2011) A novel strategy to improve systemic oxygenation in venovenous extracorporeal membrane oxygenation: the “χ-configuration”. J Thorac Cardiovasc Surg 142:1197–1204. doi:10.1016/j.jtcvs.2011.01.046
Park Y-H, Hwang S, Park H-W et al (2012) Effect of pulmonary support using extracorporeal membrane oxygenation for adult liver transplant recipients with respiratory failure. Transpl Proc 44:757–761. doi:10.1016/j.transproceed.2012.01.055
Lewandowski K, Rossaint R, Pappert D et al (1997) High survival rate in 122 ARDS patients managed according to a clinical algorithm including extracorporeal membrane oxygenation. Intensive Care Med 23:819–835
Peek GJ, Moore HM, Moore N et al (1997) Extracorporeal membrane oxygenation for adult respiratory failure. Chest 112:759–764
Terragni PP, Del Sorbo L, Mascia L et al (2009) Tidal volume lower than 6 ml/kg enhances lung protection: role of extracorporeal carbon dioxide removal. Anesthesiology 111:826–835. doi:10.1097/ALN.0b013e3181b764d2
Rossaint R, Pappert D, Gerlach H et al (1997) Extracorporeal membrane oxygenation for transport of hypoxaemic patients with severe ARDS. Br J Anaesth 78:241–246
Mols G, Loop T, Geiger K et al (2000) Extracorporeal membrane oxygenation: a ten-year experience. Am J Surg 180:144–154
Noah MA, Peek GJ, Finney SJ et al (2011) Referral to an extracorporeal membrane oxygenation center and mortality among patients with severe 2009 influenza A(H1N1). JAMA 306:1659–1668. doi:10.1001/jama.2011.1471
Beurtheret S, Mastroianni C, Pozzi M et al (2012) Extracorporeal membrane oxygenation for 2009 influenza A (H1N1) acute respiratory distress syndrome: single-centre experience with 1-year follow-up. Eur J Cardio Thorac Surg Off J Eur Assoc Cardio-Thorac Surg 41:691–695. doi:10.1093/ejcts/ezr082
Cianchi G, Bonizzoli M, Pasquini A et al (2011) Ventilatory and ECMO treatment of H1N1-induced severe respiratory failure: results of an Italian referral ECMO center. BMC Pulm Med 11:2. doi:10.1186/1471-2466-11-2
Haneya A, Philipp A, Foltan M et al (2012) First experience with the new portable extracorporeal membrane oxygenation system Cardiohelp for severe respiratory failure in adults. Perfusion 27:150–155. doi:10.1177/0267659111432330
Kipping V, Weber-Carstens S, Lojewski C et al (2013) Prone position during ECMO is safe and improves oxygenation. Int J Artif Organs 36:821–832. doi:10.5301/ijao.5000254
Noah MA, Ramachandra G, Hickey MM et al (2013) Extracorporeal membrane oxygenation and severe acute respiratory distress secondary to Legionella: 10 year experience. ASAIO J Am Soc Artif Intern Organs 1992 59:328–330. doi:10.1097/MAT.0b013e31829119c6
Schmidt M, Tachon G, Devilliers C et al (2013) Blood oxygenation and decarboxylation determinants during venovenous ECMO for respiratory failure in adults. Intensive Care Med 39:838–846. doi:10.1007/s00134-012-2785-8
Bryner B, Miskulin J, Smith C et al (2014) Extracorporeal life support for acute respiratory distress syndrome due to severe Legionella pneumonia. Perfusion 29:39–43. doi:10.1177/0267659113497229
Müller T, Philipp A, Luchner A et al (2009) A new miniaturized system for extracorporeal membrane oxygenation in adult respiratory failure. Crit Care Lond Engl 13:R205. doi:10.1186/cc8213
Freed DH, Henzler D, White CW et al (2010) Extracorporeal lung support for patients who had severe respiratory failure secondary to influenza A (H1N1) 2009 infection in Canada. Can J Anaesth J Can Anesth 57:240–247. doi:10.1007/s12630-009-9253-0
Egan TM, Duffin J, Glynn MF et al (1988) Ten-year experience with extracorporeal membrane oxygenation for severe respiratory failure. Chest 94:681–687
Lindén V, Palmér K, Reinhard J et al (2000) High survival in adult patients with acute respiratory distress syndrome treated by extracorporeal membrane oxygenation, minimal sedation, and pressure supported ventilation. Intensive Care Med 26:1630–1637
Pranikoff T, Hirschl RB, Steimle CN et al (1997) Mortality is directly related to the duration of mechanical ventilation before the initiation of extracorporeal life support for severe respiratory failure. Crit Care Med 25:28–32
Kolla S, Awad SS, Rich PB et al (1997) Extracorporeal life support for 100 adult patients with severe respiratory failure. Ann Surg 226:544–564 (discussion 565–566)
Macha M, Griffith BP, Keenan R et al (1996) ECMO support for adult patients with acute respiratory failure. ASAIO J Am Soc Artif Intern Organs 1992 42:M841–M844
Ullrich R, Lorber C, Röder G et al (1999) Controlled airway pressure therapy, nitric oxide inhalation, prone position, and extracorporeal membrane oxygenation (ECMO) as components of an integrated approach to ARDS. Anesthesiology 91:1577–1586
Hemmila MR, Rowe SA, Boules TN et al (2004) Extracorporeal life support for severe acute respiratory distress syndrome in adults. Ann Surg 240:595–605 (discussion 605–607)
Roch A, Lepaul-Ercole R, Grisoli D et al (2010) Extracorporeal membrane oxygenation for severe influenza A (H1N1) acute respiratory distress syndrome: a prospective observational comparative study. Intensive Care Med 36:1899–1905. doi:10.1007/s00134-010-2021-3
Biderman P, Einav S, Fainblut M et al (2013) Extracorporeal life support in patients with multiple injuries and severe respiratory failure: a single-center experience? J Trauma Acute Care Surg 75:907–912. doi:10.1097/TA.0b013e3182a8334f
Park M, Azevedo LCP, Mendes PV et al (2012) First-year experience of a Brazilian tertiary medical center in supporting severely ill patients using extracorporeal membrane oxygenation. Clin São Paulo Braz 67:1157–1163
Pham T, Combes A, Rozé H et al (2013) Extracorporeal membrane oxygenation for pandemic influenza A(H1N1)-induced acute respiratory distress syndrome: a cohort study and propensity-matched analysis. Am J Respir Crit Care Med 187:276–285. doi:10.1164/rccm.201205-0815OC
Schmidt M, Zogheib E, Rozé H et al (2013) The preserve mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med 39:1704–1713. doi:10.1007/s00134-013-3037-2
Frenckner B, Palmér P, Lindén V (2002) Extracorporeal respiratory support and minimally invasive ventilation in severe ARDS. Minerva Anestesiol 68:381–386
Michaels AJ, Hill JG, Long WB et al (2013) Reducing time on for extra-corporeal membrane oxygenation for adults with H1N1 pneumonia with the use of the volume diffusive respirator. Am J Surg 205:500–504. doi:10.1016/j.amjsurg.2013.01.024
Gattinoni L, Pesenti A, Mascheroni D et al (1986) Low-frequency positive-pressure ventilation with extracorporeal CO2 removal in severe acute respiratory failure. JAMA 256:881–886
Wagner PK, Knoch M, Sangmeister C et al (1990) Extracorporeal gas exchange in adult respiratory distress syndrome: associated morbidity and its surgical treatment. Br J Surg 77:1395–1398
Nierhaus A, Frings D, Braune S et al (2011) Interventional lung assist enables lung protective mechanical ventilation in acute respiratory distress syndrome. Minerva Anestesiol 77:797–801
Iglesias M, Martinez E, Badia JR, Macchiarini P (2008) Extrapulmonary ventilation for unresponsive severe acute respiratory distress syndrome after pulmonary resection. Ann Thorac Surg 85:237–244. doi:10.1016/j.athoracsur.2007.06.004 (discussion 244)
Bein T, Weber F, Philipp A et al (2006) A new pumpless extracorporeal interventional lung assist in critical hypoxemia/hypercapnia. Crit Care Med 34:1372–1377. doi:10.1097/01.CCM.0000215111.85483.BD
Morris AH, Wallace CJ, Menlove RL et al (1994) Randomized clinical trial of pressure-controlled inverse ratio ventilation and extracorporeal CO2 removal for adult respiratory distress syndrome. Am J Respir Crit Care Med 149:295–305. doi:10.1164/ajrccm.149.2.8306022
Zimmermann M, Bein T, Arlt M et al (2009) Pumpless extracorporeal interventional lung assist in patients with acute respiratory distress syndrome: a prospective pilot study. Crit Care Lond Engl 13:R10. doi:10.1186/cc7703
Brunet F, Belghith M, Mira JP et al (1993) Extracorporeal carbon dioxide removal and low-frequency positive-pressure ventilation. Improvement in arterial oxygenation with reduction of risk of pulmonary barotrauma in patients with adult respiratory distress syndrome. Chest 104:889–898
Brunet F, Mira JP, Belghith M et al (1994) Extracorporeal carbon dioxide removal technique improves oxygenation without causing overinflation. Am J Respir Crit Care Med 149:1557–1562. doi:10.1164/ajrccm.149.6.8004313
Bein T, Weber-Carstens S, Goldmann A et al (2013) Lower tidal volume strategy (≈3 ml/kg) combined with extracorporeal CO2 removal versus “conventional” protective ventilation (6 ml/kg) in severe ARDS: the prospective randomized Xtravent-study. Intensive Care Med 39:847–856. doi:10.1007/s00134-012-2787-6
Hager DN, Krishnan JA, Hayden DL et al (2005) Tidal volume reduction in patients with acute lung injury when plateau pressures are not high. Am J Respir Crit Care Med 172:1241–1245. doi:10.1164/rccm.200501-048CP
Terragni PP, Rosboch G, Tealdi A et al (2007) Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am J Respir Crit Care Med 175:160–166. doi:10.1164/rccm.200607-915OC
Needham DM, Colantuoni E, Mendez-Tellez PA et al (2012) Lung protective mechanical ventilation and two year survival in patients with acute lung injury: prospective cohort study. BMJ 344:e2124
Frank JA, Gutierrez JA, Jones KD et al (2002) Low tidal volume reduces epithelial and endothelial injury in acid-injured rat lungs. Am J Respir Crit Care Med 165:242–249. doi:10.1164/ajrccm.165.2.2108087
Jaswal DS, Leung JM, Sun J et al (2014) Tidal volume and plateau pressure use for acute lung injury from 2000 to present: a systematic literature review. Crit Care Med 42:2278–2289. doi:10.1097/CCM.0000000000000504
Aurigemma NM, Feldman NT, Gottlieb M et al (1977) Arterial oxygenation during hemodialysis. N Engl J Med 297:871–873. doi:10.1056/NEJM197710202971607
Dembinski R, Hochhausen N, Terbeck S et al (2007) Pumpless extracorporeal lung assist for protective mechanical ventilation in experimental lung injury. Crit Care Med 35:2359–2366
Vieillard-Baron A, Jardin F (2003) Right level of positive end-expiratory pressure in acute respiratory distress syndrome. Am J Respir Crit Care Med 167:1576. doi:10.1164/ajrccm.167.11.952 (author reply 1576–1577)
Lachmann B (1992) Open up the lung and keep the lung open. Intensive Care Med 18:319–321
Madjdpour C, Jewell UR, Kneller S et al (2003) Decreased alveolar oxygen induces lung inflammation. Am J Physiol Lung Cell Mol Physiol 284:L360–L367. doi:10.1152/ajplung.00158.2002
Carpenter TC, Stenmark KR (2001) Hypoxia decreases lung neprilysin expression and increases pulmonary vascular leak. Am J Physiol Lung Cell Mol Physiol 281:L941–L948
Meade MO, Cook DJ, Guyatt GH et al (2008) Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA 299:637–645. doi:10.1001/jama.299.6.637
De Wit M, Miller KB, Green DA et al (2009) Ineffective triggering predicts increased duration of mechanical ventilation. Crit Care Med 37:2740–2745
Mauri T, Bellani G, Foti G et al (2011) Successful use of neurally adjusted ventilatory assist in a patient with extremely low respiratory system compliance undergoing ECMO. Intensive Care Med 37:166–167. doi:10.1007/s00134-010-2030-2
Mauri T, Bellani G, Grasselli G et al (2013) Patient-ventilator interaction in ARDS patients with extremely low compliance undergoing ECMO: a novel approach based on diaphragm electrical activity. Intensive Care Med 39:282–291. doi:10.1007/s00134-012-2755-1
ELSO Guidelines for Cardiopulmonary Extracorporeal Life Support Extracorporeal Life Support Organization, Version 1:1. April 2009 http://www.elso.med.umich.edu/WordForms/ELSO%20Guidelines%20General%20All%20ECLS%20Version1.1.pdf. Accessed 21 Feb 2015
ClinicalTrials.gov (2013) EOLIA trial. http://www.clinicaltrials.gov/show/NCT01470703. Accessed 21 Feb 2015
Conflicts of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
J. D. Marhong and L. Munshi contributed equally to this work.
Take-home message:
ECLS facilitated provision of lung protective ventilation, as compared with baseline (pre-ECLS) settings, in the majority of studies included in our review. Use of “ultra”-protective tidal volumes and plateau pressures was common, but the benefit of this approach remains unclear. Future investigations should focus on establishing the optimal tidal volume, plateau pressure, and PEEP targets to be used for patients with ARDS supported on ECLS. The impact of these parameters on pulmonary recovery, VILI, and mortality remain to be established.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Marhong, J.D., Munshi, L., Detsky, M. et al. Mechanical ventilation during extracorporeal life support (ECLS): a systematic review. Intensive Care Med 41, 994–1003 (2015). https://doi.org/10.1007/s00134-015-3716-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-015-3716-2