
Abstract
Purpose
To determine to what extent intensive care unit environment affects family and patient satisfaction.
Methods
A before–after study was performed in one university hospital in The Netherlands, 2 months before and 2 months after the migration of an intensive care unit (ICU) with multiple beds on a ward to a newly built ICU with all single rooms. Family and patient satisfaction were determined by two surveys: family satisfaction with care in the ICU and patient satisfaction with care in the ICU, respectively.
Results
From 387 of 617 (63 %) discharged patients at least one survey (patient and/or family) was returned. Both family and patients were more satisfied with their overall ICU experience in the new ICU as compared with the old ICU. Mean scores for family satisfaction increased from 69.5 [standard deviation (SD) 16.6] to 74.1 (SD 15.2) for old and new ICU, respectively (p = 0.02). For patients, satisfaction rates increased from 63.6 (SD 18.9) to 69.6 (SD 18.3) for old and new ICU, respectively (p = 0.02). The largest differences on single items of the surveys were noted on environmental aspects.
Conclusions
This is the first study to quantify the effect of ICU environment on family and patient satisfaction. Family and patient satisfaction with ICU experience increased by 6 % in the new ICU environment with noise-reduced, single rooms with daylight, adapted colouring and improved family facilities.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Intensive care units (ICUs) provide a high-tech environment with life-saving treatment. The design of the built ICU environment has evolved over the years, from units with multiple beds in an open area divided by curtains, to units with single, private rooms [1]. It has been suggested that environmental improvements in ICU may affect family satisfaction [2, 3].
Satisfaction is an important outcome when assessing quality of care [4]. While patients are often unable to communicate or participate in decisions, family is considered a substitute decision-maker and important in evaluating satisfaction [5, 6]. Therefore, satisfaction with care in ICU is often focussed on family [7], usually involving evaluation of care, involvement in decision-making and communication [8–11]. Surveys evaluating patient satisfaction with ICU care are less common, and more directed towards measuring perception and experience of ICU patients [12], often by using general surveys of hospital care [13, 14].
Studies reveal that nursing competence, concern and caring for patients, completeness of information and environmental factors are associated with better overall family satisfaction in ICU [15]. However, the association between ICU environment and satisfaction was based on the comparison of different ICUs, with probable differences in staffing and work processes. It remained unclear whether efforts to renovate or rebuild the ICU environment might improve satisfaction ratings [16]. Furthermore, mainly family satisfaction has been studied. The impact of ICU environment on patient satisfaction has been suggested, based on studies in general wards [17, 18], but has not been studied thoroughly so far.
Recently, a new ICU with single, private rooms was opened at the University Medical Center in Utrecht, The Netherlands, which replaced an ICU with multiple beds on a ward. The new ICU incorporated the concept of healing environment, and all patient rooms have natural daylight, privacy, a view and reduced noise levels [19–21]. The migration of the old, ward-like ICU to the new ICU with only single rooms provided a unique opportunity to quantify the effect of ICU environment on both family and patient satisfaction. We hypothesized that a new patient-centred ICU environment with more privacy would decrease stress [18] and subsequently improve satisfaction. The aim of this study is to determine to what extent ICU environment affects both family and patient satisfaction.
Methods
Study design
We used a prospective before–after design. The study periods were January and February 2010 (before migration) and April and May 2010 (after migration). According to the Institutional Review Board the study was not subject to the Medical Research Involving Human Subjects Act, and therefore the necessity of informed consent was waived.
Study population
All patients in the mixed ICU of the University Medical Center Utrecht who were discharged in the study periods were eligible; the migration from the old ICU to the newly built environment was on March 1st, 2010. Exclusion criteria were admission and discharge on the same day for survivors or within 48 h for non-survivors, cross-over from the old to the new ICU and readmission to the ICU after the study period.
Intervention
The old 32 multi-bed ward ICU consisted of wards with 10–14 beds (12 m2 per bed) with no window view (Table 1). The design of the wards allowed for simultaneous monitoring of multiple patients, and for direct communication between staff.
The new ICU consists of 36 noise-reduced, single rooms (each 25 m2) with large windows and use of comfortable materials. Workflow was reorganised, and included the possibility for visual display of other patients via the bedside monitor. A satellite pharmacy at the ICU prepared medication, thereby reducing medication errors [22].
Data collection
To determine satisfaction with care, we used the family satisfaction with care in the intensive care unit survey (FS-ICU 34©) [23], which was developed and validated for assessing family satisfaction with overall ICU experience [4, 7]. We performed a cross-cultural adaptation, evaluating translation and cultural adaptation of the survey [24, 25]. The original, English FS-ICU 34© [23] was translated to Dutch (I.P.J., D.v.D., H.W.) and subsequently back-translated to English by a native speaker. Discrepancies in translation were resolved through discussion.
Since we were particularly interested in satisfaction with ICU environment, we added two questions concerning environmental aspects (Supplementary Material 1). The additional items were integrated into the original FS-ICU categories, and divided over two parts: satisfaction with care (part I, containing 21 questions) and satisfaction with decision-making (part II, containing 16 questions).
In order to measure patient satisfaction with ICU experience, we developed an abbreviated form of the survey, focussing on items that were directly related to patient care [6]. The items for this patient satisfaction with care in the intensive care unit survey (PS-ICU, see Supplementary Material 2) were selected by the researchers (I.P.J., D.v.D., H.W., C.M.R., M.M.S.) and ultimately contained 19 items, again divided over two subscales: “care” and “decision-making”.
In surviving patients, the FS-ICU (to hand over to the primary family member) and PS-ICU (to be filled in by the patient) were sent to the patient, 10 weeks after discharge from the ICU. When both patient and family did not respond, a reminder was sent after 4 weeks. In non-survivors, the FS-ICU was sent to the family 10 weeks after the patient died in or was discharged from the ICU. No reminders were sent to family of non-survivors.
The surveys were labelled with a study number, to be able to link them to patient characteristics from the patient data management system (MetaVision®; iMDsoft, Leiden, The Netherlands). Characteristics of family respondents were provided via the survey. Data were stored and analysed anonymously.
Validity of surveys
Validity, including face and content validity, has been demonstrated previously for the original FS-ICU, as well as for the German translation [4, 7, 26]. However, since we translated the survey and added two items, we assessed internal consistency by calculating Cronbach’s alpha (α), thereby evaluating the extent to which the different items of a subscale or total scale measure the same concept [27, 28]. For this analysis, we excluded three FS-ICU items with >60 % missing data (spiritual support, social work and pastoral care). We found α = 0.96 for both FS-ICU and PS-ICU (Supplementary Table III). Furthermore, we examined the corrected item-total correlation, thereby analysing the correlation of one item and the sum score of the other items in a subscale. For one item in the FS-ICU, the corrected item-scale correlation was weak (<0.30): “hope recovery patient”. Therefore, this item was removed from subscale and overall analysis [27]. In PS-ICU, all items had corrected item-scale correlation >0.30 and were included in the analyses.
Statistical analysis
For family satisfaction with overall ICU experience (primary outcome), we calculated a sample size. Based on previous studies we assumed that family satisfaction with overall ICU experience would be rated 75 % [4, 8, 11, 26], and hypothesized that improvement of environment could increase satisfaction to 80 % (small effect of environment) [11]. Therefore, we needed 175 patients in each study period, with α = 0.05 and β = 0.80. With the number of admissions of >2,000 per year and an expected non-response rate of 50 % [7, 10, 26], we planned 2 months of data collection per study period.
Descriptive analyses were used to summarize demographic characteristics of patients [age, gender, acute physiology and chronic health evaluation (APACHE) IV score, admission diagnosis, length of ICU stay, length of hospital stay, survival status] and of family respondents (age, gender, relation to patient).
Scores on the FS-ICU and PS-ICU were computed according to the validated coding and scoring procedures of the original FS-ICU [4], and presented in percentages, with 100 % representing highest satisfaction and 0 % lowest satisfaction. The primary outcome, satisfaction with overall ICU experience, was calculated by averaging the available single items, provided that per individual ≥70 % of questions were answered [4]. Secondary outcome measures were scores on the subscales “satisfaction with care” and “satisfaction with decision-making”.
Differences between the ward-like and single-room ICU in overall satisfaction were calculated by using two-sample T tests, since data were normally distributed. Additionally, we used analysis of variance (ANOVA) tests to calculate differences in satisfaction ratings per month, comparing results in more detail before and after the migration. To determine importance of items for overall satisfaction, we calculated Spearman correlations. For satisfaction with overall ICU experience, linear regression analyses were used to estimate the change in satisfaction that was associated with the migration to the single-room ICU, and to adjust for possible confounding. It has been suggested that increased age [29], male gender [30], higher severity of illness [11, 30], longer length of stay [31] and need for mechanical ventilation [15] are associated with higher satisfaction rates, as well as family of non-survivors [8, 11]. Therefore, we included these variables for adjustment. Multicollinearity was tested in advance, and all covariates were included (r < 0.8).
All statistical analyses were performed with IBM® SPSS® version 20 (IBM Corporation, Somers, NY). p-Value <0.05 was considered statistically significant.
Results
During the study periods, 709 patients were discharged (376 from the ward-like ICU, 333 from the single-room ICU) (Fig. 1). Of these, 92 patients were excluded, mainly because of short length of stay (<24 h) or unknown address of family of non-survivors. In all, from 387 of 617 discharged patients (63 %) at least one survey (FS-ICU and/or PS-ICU) was returned. From 255 discharged patients, both patient and a family member returned the survey.

Flow diagram. FS-ICU family satisfaction in intensive care unit, PS-ICU patient satisfaction in intensive care unit, LOS length of stay, ICU intensive care unit, pt patient, fam family
Family respondents returned 342 (55 %) of 617 FS-ICU surveys. On 19 of these surveys, all questions were left blank or marked “not applicable”. In written comments, family stated that they were satisfied, or that they did not fill in the survey since their loved-one died. Therefore, 323 surveys were included in analysis. Most of the family respondents were female partners with a mean age of 55 years (Table 2).
Of 568 PS-ICU surveys sent to patients who survived, 328 (58 %) were returned. On 54 surveys all questions were marked “not applicable” or left blank, with a written explanation that the patient had no memory of ICU admission. Therefore, 274 PS-ICU surveys were included in quantitative analysis. Most patient responders were male, with median age of 63 years at time of ICU admission and a median length of ICU stay of 2 days (Table 2).
Responders had a slightly higher median APACHE IV score as compared with non-responders (49 [IQR 35–68] and 47 [IQR 33–58], respectively; p = 0.04). There were no significant differences in gender, age or length of ICU stay between responders and non-responders (Supplementary Table IV).
Family satisfaction
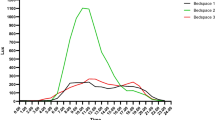
Mean family satisfaction with overall ICU experience increased from 69.5 in the ward-like ICU to 74.1 in the single-room ICU (p = 0.02) (Table 3). Mean scores on subscale “care” increased, from 65.1 to 70.8, respectively (p < 0.01). Monthly satisfaction rates after migration were higher as compared with rates before migration, though not significantly (p = 0.13) (Fig. 2). The correlation between environmental items (items 15–18) and overall satisfaction was 0.65, 0.69, 0.60 and 0.57, respectively (p < 0.001). When focussing on single items, significant differences in ratings were found on items “atmosphere ICU”, “visiting possibilities”, “atmosphere waiting room” and “facilities waiting room” (all p < 0.01) and on items “emotional support”, “courtesy toward family”, “overall experience”, “questions answered” and “amount of care”, all in favour of the new ICU (all p < 0.05) (Supplementary Table V). After adjustment for possible confounders using linear regression analyses, family satisfaction was higher in the single-room environment as compared with the ward-like ICU [β adj = 5.5, 95 % confidence interval (CI) 1.4–9.5, p < 0.01] (Table 4).

Mean satisfaction ratings per month: January and February, multi-bed ICU; April and May, single-bed ICU
Patient satisfaction
Mean patient satisfaction with overall ICU experience increased from 63.6 in the ward-like ICU to 69.6 in the single-room ICU (p = 0.02) (Table 3). On the subscale “care”, mean ratings increased from 63.6 in the ward-like ICU to 70.3 in the single-room ICU (p = 0.01). Again, monthly satisfaction rates were higher after migration (p = 0.11) (Fig. 2). The correlation between the three environmental items and overall satisfaction was 0.73 (“atmosphere ICU”), 0.61 (“silence ICU”) and 0.65 (“visiting possibilities”) (all p < 0.001). Patients discharged from the new ICU rated the following items significantly higher as compared with the old ICU: “courtesy”, “atmosphere ICU”, “silence ICU” and “visiting possibilities” (all p < 0.01) and items “pain management”, “staff recognizable” and “overall experience” (all p < 0.05) (Supplementary Table VI). After adjustment for possible confounders, patient satisfaction was still higher in the single-room ICU as compared with the ward-like ICU [β adj = 5.8, 95 % CI 0.7–10.9, p = 0.03] (Table 4).
Discussion
This is the first study to quantify the effect of ICU environment on both family and patient satisfaction. In both groups, satisfaction with overall ICU experience increased by 6 % in a new, single-room ICU, as compared with an old, ward-like ICU with multi-bed areas.
In our study, environmental aspects were strongly correlated with overall satisfaction, which is in agreement with other studies [11, 32]. The increase in satisfaction was slightly higher than hypothesized, and congruent with the suggestion that single rooms and environmental aspects, such as colour and lighting, improve overall satisfaction [9, 33, 34]. Furthermore, environment may have a positive impact on the burden of delirium and on family health, in reducing the likelihood of family post-traumatic stress or anxiety [35, 36].
As a consequence of the new setting, organisation of work flow, such as monitoring of patients and distribution of staff in the ICU, changed as well. Though staff may perceive a decreased ability to monitor multiple patients [37], simultaneous monitoring of patients was possible via visual display on the bedside monitor. Furthermore, since stocking of materials and medication was reorganised as well, nurse–patient ratios were comparable both before and after the migration.
As compared with other studies using the FS-ICU, satisfaction scores in our study were lower (72 versus 78–85 for our study and other studies, respectively) [4, 8, 11, 32]. This might be due to survey timing; we sent the surveys 10 weeks after discharge, while in most other studies surveys were distributed at discharge [4, 6, 7, 9, 10, 38]. It has been suggested that increasing time results in poorer satisfaction ratings, but results are not conclusive and consensus for timing of sending surveys has not been reached yet [29, 39, 40]. Another explanation for the difference in rating might be that this is due to cross-cultural or demographic differences [29]. Patients in our study had a shorter length of ICU stay (median 2 days as compared with 4–8 days), were more often admitted for cardiovascular reasons (where admission to ICU is often predictable) and were more likely to have their partner responding to the survey [4, 6, 8].
The use of a before–after design to study effect of migration to a new, single-room ICU was a natural experiment, with potential threats to validity. One of the limitations is the risk of selection bias. The response rate was 55 and 58 % for family and patients, respectively. This is in line with other studies that used the FS-ICU, which had response rates of 28–74 % [7, 8, 16, 26, 32, 38, 41]. It has been suggested that people are more likely to respond when they have strong feelings, either positive or negative, and that older respondents are generally more satisfied [29]. However, we compared patient characteristics of responders and non-responders and did not find differences.
We performed a cross-cultural adaptation of the FS-ICU 34©. In the original survey and in a German translation, validity was considered satisfactory [4, 7, 26]. Therefore, we did not further validate the Dutch FS-ICU, nor did we pretest and validate the PS-ICU.
We did not take into account staff satisfaction. The migration might have influenced staff satisfaction, either positively (new environment with reduced noise levels, daylight and more space) or negatively (change in routine, reduced possibilities for staff communication). However, there is no evidence yet to support or refute the impact of environment on work-related outcomes in healthcare staff [42].
The increase in satisfaction in both family and patients could potentially be attributed to other factors, such as secular trends or seasonal effects. Secular trends, i.e. improvements over time unrelated to the intervention, may not be feasible, since we covered a short period of time (5 months) and neither staffing nor protocols changed between settings. Besides, breaking up the data into four monthly periods revealed a change between February and April, when the ICU migrated. Since study periods covered different seasons (winter and spring), it might be possible that seasonal effects influenced satisfaction ratings. However, the effect of season on satisfaction ratings has not been identified so far.
As a strength, this is one of the few studies showing that both family and patient satisfaction are associated with an intervention, and therefore responsive to change. In cancer patients, effect of educative interventions on satisfaction has been studied, and though both patients and family seemed more satisfied, results have not been conclusive so far [43–45]. As far as we know, responsiveness of family and patient satisfaction to an intervention in ICU has never been studied before.
This study demonstrated that environment is an important factor in family and patient satisfaction, and that a single-room design improves satisfaction as compared with an ICU with multiple beds on a ward. When considering redesigning an ICU, a single-room design should be preferred.
Conclusions
This is the first study to quantify the effect of ICU environment on both family and patient satisfaction, within a migrating ICU including a change in workflow, but with unaltered nurse–patient ratios, physician staffing and protocols. We demonstrated that family and patient satisfaction with ICU experience increased by 6 %, respectively, in the new ICU environment consisting of noise-reduced, single rooms with daylight, adapted colouring and improved family facilities.
References
Bartley J, Streifel AJ (2010) Design of the environment of care for safety of patients and personnel: does form follow function or vice versa in the intensive care unit? Crit Care Med 38:S388–S398. doi:10.1097/CCM.0b013e3181e6d0c1
Zborowsky T, Hellmich LB (2011) Impact of place on people and process: the integration of research on the built environment in the planning and design of critical care areas. Crit Care Nurs Q 34:268–281. doi:10.1097/CNQ.0b013e31822c3831
Bazuin D, Cardon K (2011) Creating healing intensive care unit environments: physical and psychological considerations in designing critical care areas. Crit Care Nurs Q 34:259–267. doi:10.1097/CNQ.0b013e31822b8f76
Wall RJ, Engelberg RA, Downey L, Heyland DK, Curtis JR (2007) Refinement, scoring, and validation of the family satisfaction in the intensive care unit (FS-ICU) survey. Crit Care Med 35:271–279. doi:10.1097/01.CCM.0000251122.15053.50
Kryworuchko J, Heyland DK (2009) Using family satisfaction data to improve the processes of care in ICU. Intensive Care Med 35:2015–2017. doi:10.1007/s00134-009-1612-3
Stricker KH, Kimberger O, Brunner L, Rothen HU (2011) Patient satisfaction with care in the intensive care unit: can we rely on proxies? Acta Anaesthesiol Scand 55:149–156. doi:10.1111/j.1399-6576.2010.02293.x
Heyland DK, Tranmer JE (2001) Measuring family satisfaction with care in the intensive care unit: the development of a questionnaire and preliminary results. J Crit Care 16:142–149. doi:10.1053/jcrc.2001.30163
Wall RJ, Curtis JR, Cooke CR, Engelberg RA (2007) Family satisfaction in the ICU: differences between families of survivors and nonsurvivors. Chest 132:1425–1433. doi:10.1378/chest.07-0419
Henrich NJ, Dodek P, Heyland D, Cook D, Rocker G, Kutsogiannis D, Dale C, Fowler R, Ayas N (2011) Qualitative analysis of an intensive care unit family satisfaction survey. Crit Care Med 39:1000–1005. doi:10.1097/CCM.0b013e31820a92fb
Heyland DK, Rocker GM, Dodek PM, Kutsogiannis DJ, Konopad E, Cook DJ, Peters S, Tranmer JE, O’Callaghan CJ (2002) Family satisfaction with care in the intensive care unit: results of a multiple center study. Crit Care Med 30:1413–1418
Stricker KH, Kimberger O, Schmidlin K, Zwahlen M, Mohr U, Rothen HU (2009) Family satisfaction in the intensive care unit: what makes the difference? Intensive Care Med 35:2051–2059. doi:10.1007/s00134-009-1611-4
Simini B (1999) Patients’ perceptions of intensive care. Lancet 354:571–572. doi:10.1016/S0140-6736(99)02728-2
Clark PA (2007) Intensive care patients’ evaluations of the informed consent process. Dimens Crit Care Nurs 26:207–226. doi:10.1097/01.DCC.0000286826.57603.6a
Regaira ME, Sola IM, Goni VR, Del Barrio LM, Margall Coscojuela MA, siain Erro MC (2010) Care quality in intensive care evaluated by the patients using a service quality scale (SERVQUAL). Enferm Intensiva 21:3–10. doi:10.1016/j.enfi.2009.10.001
Hunziker S, McHugh W, Sarnoff-Lee B, Cannistraro S, Ngo L, Marcantonio E, Howell MD (2012) Predictors and correlates of dissatisfaction with intensive care. Crit Care Med 40:1554–1561. doi:10.1097/CCM.0b013e3182451c70
Osborn TR, Curtis JR, Nielsen EL, Back AL, Shannon SE, Engelberg RA (2012) Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control and ICU atmosphere. Chest 142:1185–1192. doi:10.1378/chest.11-3277
Trochelman K, Albert N, Spence J, Murray T, Slifcak E (2012) Patients and their families weigh in on evidence-based hospital design. Crit Care Nurse 32:e1–e10. doi:10.4037/ccn2012785
Kesecioglu J, Schneider MM, van der Kooi AW, Bion J (2012) Structure and function: planning a new ICU to optimize patient care. Curr Opin Crit Care 18:688–692. doi:10.1097/MCC.0b013e328358d4bd
Stichler JF (2001) Creating healing environments in critical care units. Crit Care Nurs Q 24:1–20
Thompson DR, Hamilton DK, Cadenhead CD, Swoboda SM, Schwindel SM, Anderson DC, Schmitz EV, St Andre AC, Axon DC, Harrell JW, Harvey MA, Howard A, Kaufman DC, Petersen C (2012) Guidelines for intensive care unit design. Crit Care Med 40:1586–1600. doi:10.1097/CCM.0b013e3182413bb2
Valentin A, Ferdinande P (2011) Recommendations on basic requirements for intensive care units: structural and organizational aspects. Intensive Care Med 37:1575–1587. doi:10.1007/s00134-011-2300-7
Dehmel C, Braune SA, Kreymann G, Baehr M, Langebrake C, Hilgarth H, Nierhaus A, Dartsch DC, Kluge S (2011) Do centrally pre-prepared solutions achieve more reliable drug concentrations than solutions prepared on the ward? Intensive Care Med 37:1311–1316. doi:10.1007/s00134-011-2230-4
Canadian researchers at the end of life network (CARENET) (2006) Family satisfaction in the intensive care unit (FS-ICU) survey. http://www.thecarenet.ca/docs/fss/FS_ICU_34.pdf. Accessed 10 November 2009
Beaton DE, Bombardier C, Guillemin F, Ferraz MB (2000) Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 25:3186–3191
Guillemin F, Bombardier C, Beaton D (1993) Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol 46:1417–1432
Stricker KH, Niemann S, Bugnon S, Wurz J, Rohrer O, Rothen HU (2007) Family satisfaction in the intensive care unit: cross-cultural adaptation of a questionnaire. J Crit Care 22:204–211. doi:10.1016/j.jcrc.2006.12.008
Polit DF, Beck CT (2012) Nursing research: generating and assessing evidence for nursing practice. Wolters Kluwer/Lippincott Williams & Wilkins, Philadelphia
Bland JM, Altman DG (1997) Cronbach’s alpha. BMJ 314:572. doi:10.1136/bmj.314.7080.572
Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, Thomas H (2002) The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature. Health Technol Assess 6:1–244
Nguyen Thi PL, Briancon S, Empereur F, Guillemin F (2002) Factors determining inpatient satisfaction with care. Soc Sci Med 54:493–504
Soufi G, Belayachi J, Himmich S, Ahid S, Soufi M, Zekraoui A, Abouqal R (2010) Patient satisfaction in an acute medicine department in Morocco. BMC Health Serv Res 10:149. doi:10.1186/1472-6963-10-149
Schwarzkopf D, Behrend S, Skupin H, Westermann I, Riedemann NC, Pfeifer R, Gunther A, Witte OW, Reinhart K, Hartog CS (2013) Family satisfaction in the intensive care unit: a quantitative and qualitative analysis. Intensive Care Med. doi: 10.1007/s00134-013-2862-7
Davidson JE, Powers K, Hedayat KM, Tieszen M, Kon AA, Shepard E, Spuhler V, Todres ID, Levy M, Barr J, Ghandi R, Hirsch G, Armstrong D (2007) Clinical practice guidelines for support of the family in the patient-centered intensive care unit: American College of Critical Care Medicine task force 2004–2005. Crit Care Med 35:605–622. doi:10.1097/01.CCM.0000254067
Jastremski CA, Harvey M (1998) Making changes to improve the intensive care unit experience for patients and their families. New Horiz 6:99–109
Davidson JE (2011) The family experience with intensive care unit care: more than mere satisfaction. Crit Care Med 39:1207–1208. doi:10.1097/CCM.0b013e318211f90a
Zaal IJ, Spruyt CF, Peelen LM, van Eijk MM, Wientjes R, Schneider MM, Kesecioglu J, Slooter AJ (2012) Intensive care unit environment may affect the course of delirium. Intensive Care Med. doi: 10.1007/s00134-012-2726-6
Shahheidari M, Homer C (2012) Impact of the design of neonatal intensive care units on neonates, staff, and families: a systematic literature review. J Perinat Neonatal Nurs 26:260–266. doi:10.1097/JPN.0b013e318261ca1d
Dodek PM, Wong H, Heyland DK, Cook DJ, Rocker GM, Kutsogiannis DJ, Dale C, Fowler R, Robinson S, Ayas NT (2012) The relationship between organizational culture and family satisfaction in critical care. Crit Care Med 40:1506–1512. doi:10.1097/CCM.0b013e318241e368
Saal D, Nuebling M, Husemann Y, Heidegger T (2005) Effect of timing on the response to postal questionnaires concerning satisfaction with anaesthesia care. Br J Anaesth 94:206–210. doi:10.1093/bja/aei024
Bjertnaes OA (2012) The association between survey timing and patient-reported experiences with hospitals: results of a national postal survey. BMC Med Res Methodol 12:13. doi:10.1186/1471-2288-12-13
Kross EK, Engelberg RA, Shannon SE, Curtis JR (2009) Potential for response bias in family surveys about end-of-life care in the ICU. Chest 136:1496–1502. doi:10.1378/chest.09-0589
Tanja-Dijkstra K, Pieterse ME (2011) The psychological effects of the physical healthcare environment on healthcare personnel. Cochrane Database Syst Rev. doi: 10.1002/14651858.CD006210
Harden J, Falahee M, Bickes J, Schafenacker A, Walker J, Mood D, Northouse L (2009) Factors associated with prostate cancer patients’ and their spouses’ satisfaction with a family-based intervention. Cancer Nurs 32:482–492. doi:10.1097/NCC.0b013e3181b311e9
Okamura H, Fukui S, Nagasaka Y, Koike M, Uchitomi Y (2003) Psychoeducational intervention for patients with primary breast cancer and patient satisfaction with information: an exploratory analysis. Breast Cancer Res Treat 80:331–338
Chan RJ, Webster J, Marquart L (2011) Information interventions for orienting patients and their carers to cancer care facilities. Cochrane Database Syst Rev. doi: 10.1002/14651858.CD008273
Acknowledgments
The authors thank all patients and their families for filling in the surveys, and Marie-Louise Luiking for the back-translation of the FS-ICU.
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Jongerden, I.P., Slooter, A.J., Peelen, L.M. et al. Effect of intensive care environment on family and patient satisfaction: a before–after study. Intensive Care Med 39, 1626–1634 (2013). https://doi.org/10.1007/s00134-013-2966-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-013-2966-0