
Abstract
Purpose
To develop and validate a continuous non-invasive blood pressure (BP) monitoring system using photoplethysmography (PPG) technology through pulse oximetry (PO).
Methods
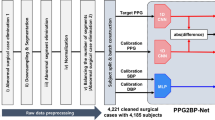
This prospective study was conducted at a critical care department and post-anesthesia care unit of a university teaching hospital. Inclusion criteria were critically ill adult patients undergoing invasive BP measurement with an arterial catheter and PO monitoring. Exclusion criteria were arrhythmia, imminent death condition, and disturbances in the arterial or the PPG curve morphology. Arterial BP and finger PO waves were recorded simultaneously for 30 min. Systolic arterial pressure (SAP), mean arterial pressure (MAP), and diastolic arterial pressure (DAP) were extracted from computer-assisted arterial pulse wave analysis. Inherent traits of both waves were used to construct a regression model with a Deep Belief Network-Restricted Boltzmann Machine (DBN-RBM) from a training cohort of patients and in order to infer BP values from the PO wave. Bland–Altman analysis was performed.
Results
A total of 707 patients were enrolled, of whom 135 were excluded. Of the 572 studied, 525 were assigned to the training cohort (TC) and 47 to the validation cohort (VC). After data processing, 53,708 frames were obtained from the TC and 7,715 frames from the VC. The mean prediction biases were −2.98 ± 19.35, −3.38 ± 10.35, and −3.65 ± 8.69 mmHg for SAP, MAP, and DAP respectively.
Conclusions
BP can be inferred from PPG using DBN-RBM modeling techniques. The results obtained with this technology are promising, but its intrinsic variability and its wide limits of agreement do not allow clinical application at this time.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Hemodynamic monitoring is essential in critically ill patients. Invasive continuous blood pressure (BP) monitoring is routinely implemented in these patients, usually through a catheter inserted in a peripheral artery, most commonly in radial or femoral arteries and less frequently in axillary or pedial arteries. However, arterial cannulation is an invasive maneuver with a potential for adverse effects such as distal ischemia, bleeding, thrombosis, and infection, which are all associated with increased morbidity and costs [1–3].
Blood pressure can also be monitored non-invasively. The two main non-invasive methods used for monitoring are the Korotkoff method, based on the sound of the brachial artery pulse when an arm cuff is deflated, and the oscillometric method, which also uses an occluding cuff but operates by sensing the magnitude of oscillations caused by the blood as it begins to flow again into the limb. However, these methods have been associated with measurement errors, namely underestimation of the systolic arterial pressure (SAP) and overestimation of the diastolic arterial pressure (DAP), especially in obese patients and in the presence of arrhythmia [4–6].
Pulse oximetry (PO) is commonly used for non-invasive assessment of oxygenation. It combines the principles of photoplethysmography (PPG) with the different wavelength absorbance of oxyhemoglobin and deoxyhemoglobin [7]. Typically, PO uses a pair of small light-emitting diodes facing a photodiode through a translucent part of the patient’s body, usually the fingertip or earlobe. The photodiode measures the variations in light intensity modified by the tissue between the diodes. The interaction between the light and the tissue is complex and includes the processes of light transmission, reflection, absorption, multiple dispersion, and fluorescence [8]. Furthermore, the change detected in the blood volume obtained from the capillary bed allows the recording of other variables such as heart rate, respiratory rate, and BP [9–11].
Given the similarity between the BP and the PPG waves, our hypothesis was that a BP value as reliable as those recorded with invasive methods could be inferred from the PPG signal analysis obtained by PO. The aim of this study was to develop and validate a new innovative method of continuous and non-invasive BP monitoring with a PPG signal obtained from PO.
Materials and methods
Study setting and population
This prospective study was conducted at the Critical Care Department and the Post-Anesthesia Care Unit of Vall d’Hebron University Hospital in Barcelona (Spain) from January 2010 to March 2012. The study was approved by the clinical research ethics committee [reference PR(AG)74/2010]. The need for informed consent was waived.
The study population included patients aged over 18 in whom BP was monitored invasively owing to their clinical condition. Exclusion criteria were the presence of arrhythmia, imminent death condition, and disturbances in the arterial or the PPG curve morphology due to patient movements, peripheral hypoperfusion, catheter artifacts (kinking, overdamping, underdamping), or PO displacement.
Data collection
Age, sex, weight, height, pathology on admission to an intensive care unit, placement and date of catheter insertion, vasoactive drugs (norepinephrine) requirement, and Acute Physiology and Chronic Health Evaluation (APACHE II) and Sequential Organ Failure Assessment (SOFA) scores were recorded.
Invasive BP and PPG measurement
The BP monitoring was performed through a 20-G catheter in the radial artery (Leader Cath, Vygon, Ecouen, France) or via a 16-G catheter in the femoral artery (Seldicath, Plastimed Division Prodimed, Le Plessis Bouchard, France) connected to a pressure transducer (Single Truwaves, Edwards Lifesciences LLC, Irvine, CA, USA). The decision to insert the catheter was taken on clinical grounds, and the location of the catheter was decided by the physician. The arterial catheter was calibrated and the square wave test was performed (see supplementary material). If there was evidence or suspicion of over/underdamping phenomena or artifacts in the BP wave, attempts were made to correct them. If these abnormalities persisted, the patient was excluded.
The PPG signal was received through the PO sensor Oxy-F4_GE (GE Healthcare Division, Firefield, CT, USA) placed on the second to fourth finger. The quality and reliability of the PPG curve were assessed. Curves with altered morphology were rejected. In patients with a radial artery catheter, the PO sensor was placed on the contralateral hand.
Both devices were connected to a processing module which was also attached to a General Electric Datex Ohmeda S/5 monitor (GE Healthcare division, Firefield, CT, USA). This monitor presented the data at the patient’s bedside and was also connected to the central network station. The BP data from the arterial catheter and from the PO were recorded by connecting an HP Compaq 6720s laptop (Hewlett-Packard Development Company, Palo Alto, CA, USA) with SS5 Collect Software (GE Healthcare division, Firefield, CT, USA) to the central network station located outside the patient’s room (see supplementary material Fig. 1).
Study phases
The study was divided into two phases. In the first period (January 2010–December 2011) data were collected in the first group of patients (the training cohort, TC) in order to train the system. The system was thus able to adjust potential bias in the estimation of the BP from the PPG signal. This was accomplished through the application of various mathematical algorithms to the PPG signal in order to calculate a set of parameters (and their variability) which were fed into a regression model based on Deep Belief Network-Restricted Boltzmann Machines (DBN-RBM) in order to obtain SAP, mean arterial pressure (MAP), and DAP.
Once the system had been trained, the second phase of the study was launched (January 2012–March 2012). In this phase the algorithm was applied in a second group of patients (the validation cohort, VC) following the same protocol in order to evaluate the system’s reliability.
Signal study
Simultaneous continuous recordings of the BP and PPG signals were implemented for every patient enrolled in the study for a period of 30 min. The protocol was only stopped if registration anomalies were observed because of catheter manipulation or unexpected events (e.g., cough or patient movements). The quality of the recorded curves was therefore optimal.
During the analysis of patient recordings, if there was evidence of over/underdamping phenomena, artifacts in BP or PPG waves, or extrasystole (supraventricular or ventricular) the patient was excluded. Each 30-min period was fragmented into frames of 10 s. Each frame was analyzed, and again those with BP or PPG waves presenting anomalies were excluded.
In compliance with the recommendations of the Association for the Advancement of Medical Instrumentation (AAMI) [12], ranges of BP curves were automatically established with limits defined by the maximum and minimum BP values (SAP, MAP, and DAP) obtained through the arterial catheter on each frame. We assessed whether the value calculated by the system fell inside the range between maximum and minimum values. If so, the error was assumed to be zero. Otherwise, when the values obtained by the system were not inside the cited range, the standard error was calculated by subtracting the value from the closest range limit (see supplementary material Fig. 2).
Statistical analysis
In our study, the BP reference values varied with time for each patient and so a statistical correction must be applied [13]. We used the Bland–Altman method, which estimates the mean bias and the standard deviation of the differences around the mean. This requires the estimation of two different variances: one for repeated differences between the two methods in the same patient and another for the differences between the averages of the two measurements (from the PO and from the catheter) across patients.
In this approach we modeled the observed difference as the sum of the mean difference (i.e., bias), heterogeneity (i.e., randomness between subjects) as well as the within-subject error: in other words bias, interpatient variability and intrapatient variability. These variances were estimated through one-way ANOVA, using the difference in matched pairs as a response and applying the corrections described by Bland–Altman [14].
The sample size of 47 patients for VC was chosen on the basis of recognized standards (Food and Drug Administration and the American National Standards Institute) for evaluation of any non-invasive BP monitor. The AAMI SP10 specifies that a minimum of 15 patients and 10 readings for each patient should be reported [12]. With 15 patients, the statistical power would be lower than 50 %. In order to obtain a statistical power of at least 80 %, we decided to include 47 patients.
Continuous parameters were expressed as means and standard deviations and absolute values as percentages. Student’s t test and the χ 2 test were used to check for differences between the groups. Means and variances of errors were assessed through a paired t test and a two-sample F test, respectively. All analyses were performed using the Matlab Statistics Toolbox software (Version 2010a, Mathworks, Natick, MA, USA).
Results
Seven hundred and seven patients were assessed for eligibility. During BP and PPG waveform analysis 135 patients were excluded (see supplementary material Fig. 3). Finally, 572 patients were studied: 525 patients in the TC and 47 in the VC.
Table 1 shows the characteristics for the population under study. APACHE II was higher in the VC, whereas height and catheter days were lower. Primary admission diagnoses are reported in the supplementary material.
The distributions for the BP obtained invasively through an arterial catheter along with a Gaussian fit are shown in supplementary material (Fig. 4). Table 2 shows the values of SAP, MAP, and DAP for the TC, VC, and entire population. All patients were hemodynamically stable during invasive BP and PPG measurement.
After data processing and exclusion of altered segments, 53,708 frames were obtained from the TC and 7,715 from the VC, with a total time of recording of 149.2 h for the TC and 21.4 h for the VC.
The mean bias for VC were −2.98 ± 19.35, −3.38 ± 10.35, and −3.65 ± 8.69 mmHg for SAP, MAP, and DAP, respectively (Fig. 1).

Bland–Altman plot of agreement between PPG and invasive BP in 7,715 corresponding measurements from 47 patients (VC) for; a systolic arterial pressure—the limits of agreement (±1.96 SD) are [−40.91, 34.94 mmHg] with a systematic error (Bland–Altman slope) of 0.47; b mean arterial pressure—the limits of agreement (±1.96 SD) are [−23.73, 16.90 mmHg] with a systematic error (Bland–Altman slope) of 0.36; and c diastolic arterial pressure—the limits of agreement (±1.96 SD) are [−20.68, 13.38 mmHg] with a systematic error (Bland–Altman slope) of 0.16
BP is strongly affected by respiratory variability. Assessing this intrinsic variability for our population, we found values of 8.37 ± 4.65, 6.13 ± 3.19, and 4.62 ± 2.59 mmHg for SAP, MAP, and DAP, respectively. Thus, intrinsic variability accounted for at least 20, 10, and 8 % of the SAP, MAP, and DAP bias, respectively.
Discussion
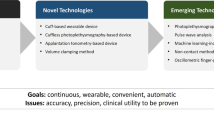
To the best of our knowledge, this is the first study to demonstrate the feasibility of non-invasive and continuous measuring of the BP through the PPG signal obtained by PO. The main advantages of our system are its non-invasiveness, its continuous character, its ease of application, and its independence from calibration. The system has been compared to the gold standard of invasive, real-time, beat-to-beat BP monitoring.
Non-invasive continuous BP monitoring has been an issue of interest for many years. In the 1980s an innovative device able to obtain the values of BP continuously and non-invasively through the pulse wave in a finger was commercialized [15] (Finapres®, TNO, Biomedical Instrumentation, Amsterdam, Netherlands). This device used the volume clamp method which is based on measuring changes in the blood input volume in the monitored vessels, first described by Peñaz [16]. Since then, the system has been modified and optimized, and other devices have been developed, namely Portapres® and Finometer® (TNO, Biomedical Instrumentation, Amsterdam, Netherlands), Nexfin® (BMEYE, Amsterdam, Netherlands), and more recently the CNAP® (CNSystems Medizintechnik AG, Graz, Austria).
Another method for non-invasive and continuous monitoring of BP values is arterial tonometry (T-line® Tensymeter, Tensys Medical Inc., San Diego, CA, USA and Vasotrac®, Medwave Inc., Arden Hills, MN, USA). This method uses a transducer located in a peripheral artery and records the changes in artery wall tension in each hemodynamic cycle. Several studies have demonstrated its effectiveness [17–21]. However, in some situations (e.g., in liver transplant patients), the BP measurements are not as precise as those obtained with the invasive method and cannot replace direct arterial BP monitoring [22]. The determination of BP using the T-Line TL-200 system is feasible in unselected critically ill medical patients but the high limits of agreement (particularly of SAP and DAP) preclude its use as a single source of BP information in unstable critically ill patients [23]. The major limitation of arterial tonometry is the requirement of optimal placement of the device on the artery to obtain exact BP values; as a result, the risk of operator-dependent bias is high.
The alternating signal of PPG is similar to that of BP, so it seems reasonable that it might be possible to infer BP values from the analysis of this signal. In the last decade, some studies have described the implementation of PPG sensors located on the arm [9] or on the finger [11], in order to obtain BP data from the PPG signal after cuff deflation. The main limitations of these systems were the fact that only SAP was monitored, the register was not continuous, and a cuff was required. Suzuki and Oguri [24, 25] developed a cuffless non-invasive system for BP estimation using a PPG sensor to measure the capacity pulse wave, but their system is not continuous and measures only SAP. Monte-Moreno described a non-invasive system of BP estimation from PPG by means of machine learning techniques, but this system does not measure BP continuously and was not compared with the reference method of invasive measurement [26].
In this study we used DBN-RBM. These are a particular kind of neural networks that build probabilistic generative models comprising a bipartite graph separating hidden and observed variables. In a sense, they can be understood as analogous to the factor analysis model. In our implementation, we also used a deep architecture (Deep Belief Network), which stacks three layers of restricted Boltzmann machines. The top layer was used to build the regression models. The lower layers receive top-down, direct connections from the layer above. The states of the units in the lowest layer represent a data vector [27, 28].
Values of SAP, MAP, and DAP were obtained through a mathematical algorithm application that detects the maximum amplitude of the PPG oscillations. We observed systematic deviations between the BP values derived from our system and those derived from invasive monitoring, especially in the SAP. Our findings are consistent with other studies that compared other non-invasive systems with invasive BP monitoring. T-Line 200 presents several discrepancies: −9.01 ± 14.52 mmHg for SAP, 0.47 ± 8.67 mmHg for MAP, and 5.22 ± 9.55 mmHg for DAP when compared with simultaneous femoral invasive BP measurements [23] and 2.3 ± 7.8 mmHg for SAP, 2.3 ± 5.9 mmHg for MAP, and 1.7 ± 6.2 mmHg for DAP when compared with radial invasive BP measurements [29]. Recently, Lehman et al. [30] described discrepancies between the BP obtained by oscillometric techniques and invasive methods, mainly in hypotensive patients. The discrepancies were basically associated with SAP, whereas there was a good correlation for MAP. Our results support the notion that MAP is more reliable than SAP for monitoring and even for treating critically ill patients.
Unlike other systems for non-invasive BP monitoring, our system uses PPG without the need for a cuff, thus minimizing invasiveness and optimizing patient comfort. Moreover, no continuous calibration is needed and the system is easy to use and can be put in place rapidly to offer an instantaneous hemodynamic evaluation and continuous reading of the tendency of the SAP, MAP, and DAP. The system also monitors continuously and gives the value of PO.
In clinical practice, a new monitoring technique is useful if its efficiency is comparable to that of the standard method. According to the AAMI, differences of ±5 mmHg or less for the mean values and ±8 mmHg for the standard deviation between the new technique and the reference method are acceptable [12]. Our mean values meet these criteria, but not the standard deviation, especially in SAP. Moreover, the limits of agreement are excessively wide, and so clinical application is not possible at this time. We think that the bias in the accuracy can be attributed in part to the respiratory variability. BP is strongly influenced by changes in intrathoracic pressure; this phenomenon was expressed in the form of intrinsic variability and was responsible for a 20 % bias in the SAP, and for biases of 10 and 8 % in MAP and DAP, respectively.
Our study has several limitations. First, the system was studied in patients with a stable invasive BP recording, but the precision of the system may not be optimal in the presence of abrupt BP variations. The identification of these transient BP variations through monitoring methods that use the PPG signal is not easy and has been the object of debate in the literature [31]. Our results cannot be extrapolated to clinical circumstances different to those established in the study. Further studies are needed to assess the validity of the system in these particular hemodynamic situations by applying it more extensively or in patients with changeable hemodynamic conditions. Second, patients with arrhythmias were not included in the study, because this condition is related to anomalies in the BP waves’ intrinsic bias in the values derived. Eighty-five patients were excluded because of anomalies in their BP curves. Strict exclusion criteria were applied in order to generate a sample as homogeneous as possible, so as to obtain the most reliable correlation between the waveform of the PPG and the catheter. Third, our PPG was processed by the GE monitor and GE SP02 module, and significantly influenced our results because we know that it affects the shape of the pulses obtained as well as their spectral properties. The neural stochastic network protocols may differ depending on the model of the connected devices, so the compatibility of the system with other equipment must be demonstrated. Finally, the problems arising from the intrinsic variability due to respiratory oscillation and wide limits of agreement of our system mean that clinical application is not possible at this time. Future studies should focus on solving this problem.
Conclusions
Arterial BP can be inferred non-invasively and continuously by the analysis of the PPG signal with stochastic neural networks. This technology is promising, but its intrinsic variability and its wide limits of agreement do not allow clinical application at this time.
Abbreviations
- AAMI:
-
Association for the Advancement of Medical Instrumentation
- ANOVA:
-
Analysis of variance
- APACHE II:
-
Acute Physiology and Chronic Health Evaluation II
- BP:
-
Blood pressure
- DAP:
-
Diastolic arterial pressure
- DBN-RBM:
-
Deep Belief Network-Restricted Boltzmann Machines
- GE:
-
General Electric
- MAP:
-
Mean arterial pressure
- PO:
-
Pulse oximetry
- PPG:
-
Photoplethysmography
- SAP:
-
Systolic arterial pressure
- SOFA:
-
Sequential Organ Failure Assessment
- TC:
-
Training cohort
- VC:
-
Validation cohort
References
Warren DK, Quadir WW, Hollenbeak CS et al (2006) Attributable cost of catheter-associated bloodstream infections among intensive care patients in a nonteaching hospital. Crit Care Med 34:2084–2089
Scheer BV, Perel A, Pfeiffer UJ (2002) Clinical review: complications and risk factors of peripheral arterial catheters used for haemodynamic monitoring in anaesthesia and intensive care medicine. Crit Care 6:198–204
Lorente L, Galvan R, Martín MM et al (2003) Trate of intravascular catheter infection line days. Med Intensiva 27:224–228
Stolt M, Sjönell G, Aström H et al (1993) Improved accuracy of indirect blood pressure measurement in patients with obese arms. Am J Hypertens 6:66–71
Bur A, Hirschl MM, Herkner H et al (2000) Accuracy of oscillometric blood pressure measurement according to the relation between cuff size and upper-arm circumference in critically ill patients. Crit Care Med 28:371–376
Jones DW, Apple LJ, Sheps SG et al (2003) Measuring blood pressure accurately. New and persistent changes. JAMA 289:1027–1030
Allen J (2007) Photoplethysmography and its applications in clinical physiological measurement. Physiol Meas 28:R1–R39
Anderson RR, Parrish JA (1981) The optics of human skin. J Invest Dermatol 77:13–19
Laurent C, Jönsson B, Vergfors M et al (2005) Non-invasive measurement of systolic blood pressure on the arm utilising photoplethysmography: development of methodology. Med Biol Eng Comput 43:131–135
Nitzan M, Faib I, Friedman H (2006) Respiration-induced changes in tissues blood volume distal to occluded artery, measured by photoplethysmography. J Biomed Opt 11:040506
Nitzan M, Patron A, Glik Z et al (2009) Automatic non-invasive measurement of systolic blood pressure using photoplethysmography. Biomed Eng Online 8:28
Association for the Advancement of Medical Instrumentation. American National Standard (2002) Manual, Electronic or Automated Sphygmomanometers. ANSI/AAMI SP10. ANSI, Arlington, VA
Bland JM, Altman DG (2007) Agreement between methods of measurement with multiple observations per individual. J Biopharm Stat 17:571–582
Bland JM, Altman DG (1999) Measuring agreement in method comparison studies. Stat Methods Med Res 8:135–160
Van Egmond J, Hasenbos M, Crul JF (1985) Invasive versus non-invasive measurement of arterial pressure. Comparison of two automatic methods and simultaneously measured direct intra-arterial pressure. Br J Anaesth 57:434–444
Peñaz J (1973) Photoelectric measurement of blood pressure, volume and flow in the finger. In: Albert A, Vogt W, Hellig W (eds) Digest of the 10th International Conference on Medical and Biological Engineering. International Federation for Medical and Biological Engineering, Dresden, Germany, p 104
Janelle GM, Gravenstein N (2006) An accuracy evaluation of the T-Line® Tensymeter (continuous non-invasive blood pressure management device) versus conventional invasive radial artery monitoring in surgical patients. Anesth Analg 102:484–490
Belani KG, Buckley JJ, Poliac MO (1999) Accuracy of radial artery blood pressure determination with the Vasotrac. Can J Anaesth 46:488–496
McCann ME, Hill D, Thomas KC et al (2005) A comparison of radial artery blood pressure determination between the Vasotrac device and invasive arterial blood pressure monitoring in adolescents undergoing scoliosis surgery. Anesth Analg 101:978–985
Belani K, Ozaki M, Hynson J et al (1999) A new non-invasive method to measure blood pressure. Anesthesiology 91:686–692
Szmuk P, Pivalizza E, Warters RD et al (2008) An evaluation of the T-Line© Tensymeter continuous non-invasive blood pressure device during induced hypotension. Anaesthesia 63:307–312
Findlay JY, Gali B, Keegan MT et al (2006) Vasotrac® arterial blood pressure and direct arterial blood pressure monitoring during liver transplantation. Anesth Analg 102:690–693
Saugel B, Fassio A, Hapfelmeier A et al (2012) The T-Line TL-200 system for continuous non-invasive blood pressure measurement in medical intensive care unit patients. Intensive Care Med 38:1471–1477
Suzuki S, Oguri K (2008) Cuffless and non-invasive systolic blood pressure estimation for aged class by using a photoplethysmograph. Conf Proc IEEE Eng Med Biol Soc 2008:1327–1330
Suzuki S, Oguri K (2009) Cuffless blood pressure estimation by error-correcting output coding method based on an aggregation of adaboost with a photoplethysmograph sensor. Conf Proc IEEE Eng Med Biol Soc 2009:6765–6768
Monte-Moreno E (2011) Non-invasive estimate of blood glucose and blood pressure from a photoplethysmograph by means of machine learning techniques. Artif Intell Med 53:127–138
Hinton GE, Onsidero S, Teh YW (2006) A fast learning algorithm for deep belief nets. Neural Comput 18:1527–1554
Hinton GE, Salkhutdinov RR (2006) Reducing the dimensionality of data with neural networks. Science 313:504–507
Dueck R, Goedje O, Clopton P (2012) Nonivasive continuous beat-to-beat radial pressure artery via TL-200 applanation tonometry. J Clin Monit Comput 26:75–839
Lehman LH, Saeed M, Talmor D et al (2013) Methods of blood pressure measurement in the ICU. Crit Care Med 41:34–40
Panerai RB, Sammons EL, Smith SM et al (2007) Transient drift between finapres and continuous intra-aortic measurement of blood pressure. Blood Pres Monit 12:369–376
Acknowledgments
This work was supported in part by Sabirmedical SL (Parc Cientific de Barcelona, Barcelona, Spain), and by “Avanza” grants (Ministry of Industry, Tourism and Trade, Government of Spain, TSI-020100-2009-204 and TSI-020100-2010-625).
Conflicts of interest
J.C. Ruiz-Rodriguez and J. Caballero have received grant support for travel expenses from Sabirmedical SL. J.C. Ruiz-Rodriguez, J. Caballero, A. Ruiz-Sanmartin, J. Riera, S. García-Roche, and J. Rello have collaborated with Sabirmedical SL in other research projects or in an advisory capacity. V. Ribas was the scientific director of Sabirmedical. O. de Sola-Morales was Sabirmedical’s medical and market access director. No other authors report any financial disclosures.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Ruiz-Rodríguez, J.C., Ruiz-Sanmartín, A., Ribas, V. et al. Innovative continuous non-invasive cuffless blood pressure monitoring based on photoplethysmography technology. Intensive Care Med 39, 1618–1625 (2013). https://doi.org/10.1007/s00134-013-2964-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-013-2964-2