
Abstract
Purpose
We aimed to determine the incidence, risk factors and outcome of acute kidney injury (AKI) in Finnish ICUs.
Methods
This prospective, observational, multi-centre study comprised adult emergency admissions and elective patients whose stay exceeded 24 h during a 5-month period in 17 Finnish ICUs. We defined AKI first by the Acute Kidney Injury Network (AKIN) criteria supplemented with a baseline creatinine and second with the Kidney Disease: Improving Global Outcomes (KDIGO) criteria. We screened the patients’ AKI status and risk factors for up to 5 days.
Results
We included 2,901 patients. The incidence (95 % confidence interval) of AKI was 39.3 % (37.5–41.1 %). The incidence was 17.2 % (15.8–18.6 %) for stage 1, 8.0 % (7.0–9.0 %) for stage 2 and 14.1 % (12.8–15.4 %) for stage 3 AKI. Of the 2,901 patients 296 [10.2 % (9.1–11.3 %)] received renal replacement therapy. We received an identical classification with the new KDIGO criteria. The population-based incidence (95 % CI) of ICU-treated AKI was 746 (717–774) per million population per year (reference population: 3,671,143, i.e. 85 % of the Finnish adult population). In logistic regression, pre-ICU hypovolaemia, diuretics, colloids and chronic kidney disease were independent risk factors for AKI. Hospital mortality (95 % CI) for AKI patients was 25.6 % (23.0–28.2 %) and the 90-day mortality for AKI patients was 33.7 % (30.9–36.5 %). All AKIN stages were independently associated with 90-day mortality.
Conclusions
The incidence of AKI in the critically ill in Finland was comparable to previous large multi-centre ICU studies. Hospital mortality (26 %) in AKI patients appeared comparable to or lower than in other studies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acute kidney injury (AKI) frequently complicates the course of critical illness and is associated with a substantial increase in morbidity and mortality. AKI, defined as a reduction in glomerular filtration rate (GFR) occurring during hours or days and leading to disturbances in fluid and electrolyte balance, is a multi-etiological disorder with a few known risk factors [1]. The detailed pathogenesis of AKI is still unclear [2, 3]. The current consensus for diagnosing and staging AKI has been the Acute Kidney Injury Network’s (AKIN) modification of the original RIFLE criteria (2007) [4]. The AKIN criteria divide AKI into three grades of severity (stages 1–3) based on urine output and serum/plasma creatinine (Cr) levels. In 2012 the Kidney Disease: Improving Global Outcomes (KDIGO) foundation published a new guideline for defining and classifying AKI in which the AKIN criteria are supplemented with some small changes [5]. The original RIFLE criteria have been validated in over half a million patients [6]. All RIFLE grades are independently predictive for hospital mortality [7]. The overall incidence of AKI in hospitalised patients has been reported as 20 % [8], but up to 67 % in the critically ill [9, 10]. Sepsis in particular is often complicated by AKI. Recent data suggest that the incidence of AKI is increasing [11].
AKI is associated with dismal outcomes. Hospital mortality of patients with stage 3 (RIFLE F) AKI is approximately 40 % [12], and the 5-year mortality is up to 70 % [13]. Even small and transient changes in serum/plasma Cr are associated with increased mortality [14].
No prospective population-based studies on the incidence of AKI in intensive care units (ICU) defined by the RIFLE, AKIN or the KDIGO criteria exist. Therefore, in this nationwide multi-centre, prospective observational cohort study we aimed to determine the incidence, risk factors and outcome of AKI in Finnish ICU patients.
Materials and methods
Data source
Seventeen Finnish ICUs participated in this prospective, observational study between 1 September 2011 and 1 February 2012 (a 5-month period). The Ethics Committee of the Department of Surgery in Helsinki University Hospital gave the nationwide approval for the study and for a deferred consent policy from the patient or proxy. The Finnish National Institute of Health and Welfare approved collection of data from medical records regarding deceased patients.
For the incidence calculations we obtained the number of adult (>18 years) population in the area of the participating hospitals from Statistics Finland (http://www.stat.fi, accessed 31 Dec 2011). The number of adult patients on chronic renal replacement therapy (N = 1,527) according to the Finnish Registry for kidney diseases [15] was extracted from the population. The total reference population for the calculations was 3,671,143 representing 85 % of the Finnish adult population.
Patients
We included (1) all emergency ICU admissions and (2) all elective patients with an ICU stay longer than 24 h. We excluded (1) patients under 18 years of age, (2) re-admitted patients who received renal replacement therapy (RRT) during their previous admission, (3) elective ICU patients treated for less than 24 h if discharged alive, (4) patients on chronic dialysis, (5) organ donors, (6) patients with no permanent residency in Finland or insufficient language skills, (7) transferred patients included in the study for 5 days and (8) intermediate care patients. Thus, each patient was included only once.
Definitions
Our AKI definition followed the AKIN modification of the original RIFLE criteria (later as AKIN) [4] with a continuous moving baseline for both the Cr and urine output. When available, we used Cr and urine output data starting from 48 h preceding ICU admission. Concerning the Cr-based staging we applied the requirement for the acute rise within 48 h. However, owing to evident limitations in the AKIN criteria in identifying all AKI patients [12], we modified the AKIN by adding a baseline preceding critical illness which was the most recent value from the previous year excluding the week preceding admission. If baseline Cr was not available we estimated it using the modification of diet in renal disease (MDRD) equation assuming a GFR of 75 ml/min/1.73 m2 [16]. Retrospectively, we recalculated the AKI staging using the newest KDIGO criteria [5]. We screened AKI and AKI risk factors at admission and during the first 5 days of admission including severe sepsis and disseminated intravascular coagulation (DIC) using the American College of Chest Physicians/Society of Critical Care Medicine (ACCP/SCCM) and International Society on Thrombosis and Haemostasis (ISTH) criteria [17, 18]. For each patient the highest AKIN stage served as the value for the incidence calculations. For re-admitted patients we chose the admission with the highest AKIN stage. The study entry time was ICU admission time.
Data collection
At the time of the study the Finnish Intensive Care Consortium (FICC) comprised 25 ICUs in university or central hospitals across Finland. The consortium maintains a database (Tieto Ltd, Helsinki, Finland), where routine data including demographics, ICU scores, length of stay (LOS), physiologic data and hospital mortality are prospectively collected. We measured serum/plasma Cr daily and urine output hourly and calculated an AKIN stage for each patient continuously based on every measured hourly urine output and Cr value. The AKIN stage calculations for the urine output criteria were performed by an automated calculator integrated into the study database. To augment the data collected by the database we completed a standardized case report form (CRF) at admission, daily for 5 days and at ICU discharge. The CRF data comprised of chronic and present health status, medications, detailed information on possible risk factors for AKI, evaluation of severe sepsis, DIC, other organ dysfunction, fluid balance and information on possible RRT. This additional study-specific CRF comprised 54 % of the study dataset variables. We monitored the reliability and completeness of the CRF data in eight randomly chosen study sites using a structured monitoring plan.
Statistical analyses
We analysed the data by using SPSS version 19 (SPSS, Chicago, Ill., USA). We present the data as medians with interquartile ranges (IQR), or as absolute numbers [percentage with 95 % confidence intervals (CI)]. We compared groups using the Mann–Whitney U test for continuous data and Fisher’s exact test or χ 2 test for categorical data, when applicable. Hospital mortality rates between different groups were compared by the χ 2 test. First, we analysed the association between AKI and risk factors by a univariate analysis. Second, we calculated independent odds ratios (OR with 95 % CI) for risk factors by backward conditional stepwise logistic regression analysis. A p value less than 0.05 was considered as statistically significant in all analyses.
Results
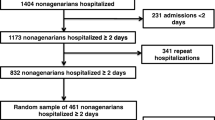
Altogether 2,901 patients were included in the study. The study flow chart is presented as Fig. 1. Baseline characteristics of the study patients are presented in Table 1. The incidence (95 % CI) of AKI was 1,141/2,901 patients [39.3 % (37.5–41.1 %]); including stage 1 AKI in 499 patients [17.2 % (15.8–18.6 %)], stage 2 AKI in 232 patients [8.0 % (7.0–9.0 %)] and stage 3 AKI in 410 patients [14.1 % (12.8–15.4 %)]. Retrospectively, the KDIGO criteria gave exactly the same AKI classification. Of the 2,901 patients, 296 [10.2 % (9.1–11.3 %)] received renal replacement therapy, of whom 272 (91.9 %) during the first five ICU days (Fig. 1). Table 2 illustrates the characteristics of the AKI patients according to their highest AKIN stage. The population-based incidence (95 % CI) of ICU-treated AKI was 746 (717–774) per million population (pmp) per year.

Study flow chart. Critically ill patients stratified by AKI using highest Acute Kidney Injury Network (AKIN)/Kidney Disease: Improving Global Outcomes (KDIGO) stage. AKI acute kidney injury, RRT renal replacement therapy
The majority of AKI patients (N = 950, 83 %) had AKI at admission or during the first two ICU days. The progression of AKI is presented as Fig. 2. Including all risk factors, preceding AKI severe sepsis, pre-ICU hypovolaemia and pre-ICU hypotension were more frequent in patients with AKI (Table 3). In a multivariable logistic regression analysis [covariates entered: pre-ICU hypovolaemia, pre-ICU use of diuretics, pre-ICU use of colloids (52 % gelatin, 40 % starch and 8 % both), hypertension and chronic kidney disease] pre-ICU hypovolaemia [OR (95 % CI) 2.20 (1.85–2.62)], pre-ICU use of diuretics [OR (95 % CI) 1.68 (1.41–2.00)] or colloids [OR (95 % CI) 1.35 (1.13–1.61)] and chronic kidney disease [OR (95 % CI) 2.64 (1.88–3.71)] were independent risk factors for AKI.

Progression of acute kidney injury (AKI) from admission (day 1) to day 2 in all patients (N = 2,901)
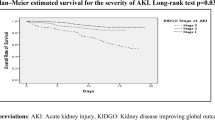
The median ICU LOS (interquartile range) for AKI patients was 3.7 (1.9–6.4) days compared to that of 1.9 (1.0–4.0) in patients without AKI (P < 0.001). Of the 1,141 AKI patients 853 (74.8 %) received mechanical ventilation compared to 1,159 (65.9 %) of patients without AKI (P < 0.001). Overall hospital mortality (95 % CI) for AKI patients was 292/1,141 [25.6 % (23.0–28.2 %)] compared to 179/1,760 [10.2 % (8.7–11.6 %)] in patients with no AKI. The 90-day mortality (95 % CI) for patients with and without AKI was 385/1,141 [33.7 % (30.9–36.5 %)] versus 293/1,760 [16.6 % (14.9–18.4 %)], respectively. There was a linear increase in the 90-day mortality (95 % CI) with advancing stage of AKI: 29.3 % (25.2–33.3 %) for stage 1, 34.1 % (27.8–40.3 %) for stage 2 and 39.0 % (34.2–43.8 %) for stage 3. Of the patients who received RRT, 116/296 [39.2 % (38.6–39.8 %)] had died and 34/296 [11.5 % (7.8–15.2 %)] were still dependent on RRT at day 90. The 90-day survival of patients with and without AKI is presented in Fig. 3. In a logistic regression analysis AKI was independently associated with increased 90-day mortality [ORs (95 % CI) 1.71 (1.31–2.23), 1.78 (1.26–2.51), 1.71 (1.28–2.29) for AKIN stages 1–3, respectively]. In this analysis non-operative admission (OR 2.21), age (OR 1.04), and highest lactate from the first 24 h of admission (OR 1.17) were also independently associated with 90-day mortality.

Kaplan–Meier 90-day survival curves. a Patients with and without acute kidney injury (AKI). b Patients without AKI and patients with different Acute Kidney Injury Network (AKIN)/Kidney Disease: Improving Global Outcomes (KDIGO) stages of AKI
Discussion
In this study we found that the population-based incidence of ICU-treated AKI was 746 pmp/year. The incidence of AKI in adult ICU patients in Finland was 39 %. Independent factors associated with AKI were pre-ICU hypovolaemia, pre-ICU use of diuretics and colloids, and chronic kidney disease. The 90-day mortality for AKI patients was 34 %.
To the best of our knowledge no previous study has evaluated the population-based incidence of ICU-treated AKI using a prospective, multi-centre, nationwide study design and standardized complete RIFLE, AKIN or KDIGO criteria. A retrospective study from one county area (population 124,277) from the USA reported a very high incidence of ICU-treated AKI (2,900 pmp/year) compared to our study [19]. In another retrospective study from one region in Scotland (population 523,390) the incidence of AKI was reported as 2,147 pmp/year [20]. Results from recent epidemiological AKI studies using original RIFLE or AKIN criteria are not uniform and report AKI incidences from 10 to 70 % among ICU patients [7, 9, 10, 12, 21, 22]. Variations in AKI definitions and study populations may partly explain the differences. Our results are comparable to two large retrospective studies using the AKIN criteria that reported AKI incidences of 37.1 % [7] and 28.5 % [12]. We found a higher incidence of stage 3 AKI (14 %), which may be explained by the fact that RRT data were not completely available in the other two large studies [7, 12]. The number of RRT patients in our study was in close agreement with a previous retrospective report from Finland [23].
This is the first AKI incidence study evaluation the newly published KDIGO criteria. At the time of this study the KDIGO criteria were not yet available. However, we were able to retrospectively use the KDIGO criteria. In this population, our ‘modified AKIN’ and the KDIGO criteria resulted in exactly the same classification of the patients to different AKI stages.
Coincidental risk factors and chronic comorbidities such as old age, hypovolaemia, diabetes, heart or lung disease are considered to predispose patients to AKI [5]. In agreement, in our study the AKI patients were older, and had more baseline comorbidities, and medications (Table 1). Hypertension, arteriosclerosis, diabetes and chronic kidney disease were frequent in AKI patients. Over one-third of the AKI patients used diuretics, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, or statins, were hypovolaemic, had severe sepsis, or were hypotensive prior to AKI onset (Table 3). In this respect two other multi-centre, prospective studies on AKI have had comparable findings [21, 22]. Before ICU admission a larger proportion of AKI patients had received diuretics and colloids (starch and gelatin) compared to patients without AKI. However, during ICU treatment a smaller proportion of AKI patients received diuretics and the use of colloids did not differ between patients with and without AKI. Of the patients that received colloids before ICU admission half received gelatin, 40 % received starch and less then 10 % received both.
The hospital mortality of AKI patients (26 %) corroborated with that of a previous large multi-centre study (25 %) [7]. Hospital mortality in different AKIN stages 1–3 (20, 26 and 32 %, respectively) were comparable to a previous Finnish retrospective study [24]. In a study by Joannidis et al. [12] the reported hospital mortality for AKIN stage 1 (34.5 %), stage 2 (29.0 %) and stage 3 (41.2 %) were higher compared to our study. Regrettably, no studies reporting 90-day mortality of ICU-treated AKI patients (34 % in this study) classified according to RIFLE or AKIN exist.
Our study has some limitations. First, we focused our study on ICU-treated AKI. Concomitantly, the number of AKI patients treated in ordinary wards is plausibly substantial. Second, we decided to screen patients for AKI for 5 days and were therefore unable to register the late AKIs. However, in this study 83 % of the AKI patients developed AKI on day 1 or day 2. Third, we could obtain actual baseline serum/plasma Cr values for 64 % of patients and estimated those lacking a baseline Cr with MDRD calculation, as suggested [25]. However, the MDRD method may lead to a slight over- or underestimation of AKI [26, 27]. Fourth, owing to limited data we were not able to analyse the independent association of starch/gelatin with risk of AKI. Finally, we excluded elective admissions with an expected ICU LOS of less than 1 day, but we included those patients if their ICU stay exceeded 24 h. The strength of our study is the multi-centre, prospective design covering the majority of the adult population in Finland. Additionally, we were able to include the 90-day mortality data and, thus, to present the actual long-term outcome of the AKI patients.
In this nationwide prospective study we found that the incidence of AKI in Finnish ICUs was in close agreement with the few other studies using comparable AKI criteria. The hospital mortality (26 %) of critically ill patients with AKI was comparable or lower than in other studies. Of note, two-thirds of the AKI patients were still alive at day 90.
References
de Mendonca A, Vincent JL, Suter PM, Moreno R, Dearden NM, Antonelli M, Takala J, Sprung C, Cantraine F (2000) Acute renal failure in the ICU: risk factors and outcome evaluated by the SOFA score. Intensive Care Med 26:915–921
Bonventre JV (2010) Pathophysiology of AKI: injury and normal and abnormal repair. Contrib Nephrol 165:9–17
Wen X, Murugan R, Peng Z, Kellum JA (2010) Pathophysiology of acute kidney injury: a new perspective. Contrib Nephrol 165:39–45
Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, Levin A (2007) Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Crit Care 11:R31
Liet JM, Dejode JM, Joram N, Gaillard Le Roux B, Pereon Y (2012) Bedside diagnosis of bilateral diaphragmatic paralysis. Intensive Care Med. doi:10.1007/s00134-012-2729-3
Ricci Z, Cruz D, Ronco C (2008) The RIFLE criteria and mortality in acute kidney injury: a systematic review. Kidney Int 73:538–546
Bagshaw SM, George C, Bellomo R (2008) A comparison of the RIFLE and AKIN criteria for acute kidney injury in critically ill patients. Nephrol Dial Transplant 23:1569–1574
Uchino S, Bellomo R, Goldsmith D, Bates S, Ronco C (2006) An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit Care Med 34:1913–1917
Ostermann M, Chang RW (2007) Acute kidney injury in the intensive care unit according to RIFLE. Crit Care Med 35:1837–1843 quiz 1852
Hoste EA, Clermont G, Kersten A, Venkataraman R, Angus DC, De Bacquer D, Kellum JA (2006) RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care 10:R73
Bagshaw SM, George C, Bellomo R (2007) Changes in the incidence and outcome for early acute kidney injury in a cohort of Australian intensive care units. Crit Care 11:R68
Joannidis M, Metnitz B, Bauer P, Schusterschitz N, Moreno R, Druml W, Metnitz PG (2009) Acute kidney injury in critically ill patients classified by AKIN versus RIFLE using the SAPS 3 database. Intensive Care Med 35:1692–1702
Åhlstrom A, Tallgren M, Peltonen S, Räsänen P, Pettilä V (2005) Survival and quality of life of patients requiring acute renal replacement therapy. Intensive Care Med 31:1222–1228
Uchino S, Bellomo R, Bagshaw SM, Goldsmith D (2010) Transient azotaemia is associated with a high risk of death in hospitalized patients. Nephrol Dial Transplant 25:1833–1839
Pappalardo F, Pieri M, Greco T, Patroniti N, Pesenti A, Arcadipane A, Ranieri VM, Gattinoni L, Landoni G, Holzgraefe B, Beutel G, Zangrillo A (2012) Predicting mortality risk in patients undergoing venovenous ECMO for ARDS due to influenza A (H1N1) pneumonia: the ECMOnet score. Intensive Care Med. doi:10.1007/s00134-012-2747-1
Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, Hogg RJ, Perrone RD, Lau J, Eknoyan G (2003) National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med 139:137–147
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G (2003) 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Crit Care Med 31:1250–1256
Taylor FB Jr, Toh CH, Hoots WK, Wada H, Levi M (2001) Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost 86:1327–1330
Cartin-Ceba R, Kojicic M, Li G, Kor DJ, Poulose J, Herasevich V, Kashyap R, Trillo-Alvarez C, Cabello-Garza J, Hubmayr R, Seferian EG, Gajic O (2011) Epidemiology of critical care syndromes, organ failures, and life-support interventions in a suburban US community. Chest 140:1447–1455
Ali T, Khan I, Simpson W, Prescott G, Townend J, Smith W, Macleod A (2007) Incidence and outcomes in acute kidney injury: a comprehensive population-based study. J Am Soc Nephrol 18:1292–1298
Cruz DN, Bolgan I, Perazella MA, Bonello M, de Cal M, Corradi V, Polanco N, Ocampo C, Nalesso F, Piccinni P, Ronco C (2007) North East Italian prospective hospital renal outcome survey on acute kidney injury (NEiPHROS-AKI): targeting the problem with the RIFLE criteria. Clin J Am Soc Nephrol 2:418–425
Piccinni P, Cruz DN, Gramaticopolo S, Garzotto F, Dal Santo M, Aneloni G, Rocco M, Alessandri E, Giunta F, Michetti V, Iannuzzi M, Belluomo Anello C, Brienza N, Carlini M, Pelaia P, Gabbanelli V, Ronco C (2011) Prospective multicenter study on epidemiology of acute kidney injury in the ICU: a critical care nephrology Italian collaborative effort (NEFROINT). Minerva Anestesiol 77:1072–1083
Vaara ST, Pettilä V, Reinikainen M, Kaukonen KM (2012) Population-based incidence, mortality and quality of life in critically ill patients treated with renal replacement therapy: a nationwide retrospective cohort study in Finnish intensive care units. Crit Care 16:R13
Åhlstrom A, Kuitunen A, Peltonen S, Hynninen M, Tallgren M, Aaltonen J, Pettilä V (2006) Comparison of 2 acute renal failure severity scores to general scoring systems in the critically ill. Am J Kidney Dis 48:262–268
Srisawat N, Kellum JA (2011) Acute kidney injury: definition, epidemiology, and outcome. Current opinion in critical care 17:548–555
Gaiao S, Cruz DN (2010) Baseline creatinine to define acute kidney injury: is there any consensus? Nephrol Dial Transplant 25:3812–3814
Ricci Z, Cruz DN, Ronco C (2011) Classification and staging of acute kidney injury: beyond the RIFLE and AKIN criteria. Nat Rev Nephrol 7:201–208
Acknowledgments
We thank Tieto Healthcare and Welfare Ltd for database management. We received Clinical Research funding (EVO) TYH 2010109/2011210 and T102010070 from Helsinki University Hospital and grants from the Finnish Society of Intensive Care, the Academy of Finland and the Juselius Foundation. SN has received a grant from the Finnish Society of Anaesthesiologists.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Members of the FINNAKI Study Group are listed in the Appendix.
The FINNAKI study group
The FINNAKI study group
Central Finland Central Hospital: Raili Laru-Sompa, Anni Pulkkinen, Minna Saarelainen, Mikko Reilama, Sinikka Tolmunen, Ulla Rantalainen, Marja Miettinen. East Savo Central Hospital: Markku Suvela, Katrine Pesola, Pekka Saastamoinen, Sirpa Kauppinen. Helsinki University Central Hospital: Ville Pettilä, Kirsi-Maija Kaukonen, Anna-Maija Korhonen, Sara Nisula, Suvi Vaara, Raili Suojaranta-Ylinen, Leena Mildh, Mikko Haapio, Laura Nurminen, Sari Sutinen, Leena Pettilä, Helinä Laitinen, Heidi Syrjä, Kirsi Henttonen, Elina Lappi, Hillevi Boman. Jorvi Central Hospital: Tero Varpula, Päivi Porkka, Mirka Sivula Mira Rahkonen, Anne Tsurkka, Taina Nieminen, Niina Prittinen. Kanta-Häme Central Hospital: Ari Alaspää, Ville Salanto, Hanna Juntunen, Teija Sanisalo. Kuopio University Hospital: Ilkka Parviainen, Ari Uusaro, Esko Ruokonen, Stepani Bendel, Niina Rissanen, Maarit Lång, Sari Rahikainen, Saija Rissanen, Merja Ahonen, Elina Halonen, Eija Vaskelainen. Lapland Central Hospital: Meri Poukkanen, Esa Lintula, Sirpa Suominen. Länsi Pohja Central Hospital: Jorma Heikkinen, Timo Lavander, Kirsi Heinonen, Anne-Mari Juopperi. Middle Ostrobothnia Central Hospital: Tadeusz Kaminski, Fiia Gäddnäs, Tuija Kuusela, Jane Roiko. North Karelia Central Hospital: Sari Karlsson, Matti Reinikainen, Tero Surakka, Helena Jyrkönen, Tanja Eiserbeck, Jaana Kallinen. Satakunta Hospital District: Vesa Lund, Päivi Tuominen, Pauliina Perkola, Riikka Tuominen, Marika Hietaranta, Satu Johansson. South Karelia Central Hospital: Seppo Hovilehto, Anne Kirsi, Pekka Tiainen, Tuija Myllärinen, Pirjo Leino, Anne Toropainen. Tampere University Hospital: Anne Kuitunen, Ilona Leppänen, Markus Levoranta, Sanna Hoppu, Jukka Sauranen, Jyrki Tenhunen, Atte Kukkurainen, Samuli Kortelainen, Simo Varila. Turku University Hospital: Outi Inkinen, Niina Koivuviita, Jutta Kotamäki, Anu Laine. Oulu University Hospital: Tero Ala-Kokko, Jouko Laurila, Sinikka Sälkiö. Vaasa Central Hospital: Simo-Pekka Koivisto, Raku Hautamäki, Maria Skinnar.
Rights and permissions
About this article
Cite this article
Nisula, S., Kaukonen, KM., Vaara, S.T. et al. Incidence, risk factors and 90-day mortality of patients with acute kidney injury in Finnish intensive care units: the FINNAKI study. Intensive Care Med 39, 420–428 (2013). https://doi.org/10.1007/s00134-012-2796-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-012-2796-5