
Abstract
Purpose
To confirm the pharmacodynamics and evaluate the efficacy of high-dose selenium (Se) administered by continuous infusion, following an initial loading bolus of selenite, on clinical outcome in critically ill patients with systemic inflammatory response syndrome (SIRS).
Methods
Prospective, placebo-controlled, randomized, single-blinded phase II study in a multidisciplinary university hospital intensive care unit (ICU). Two groups of patients with SIRS, age >18 years, and Acute Physiology and Chronic Health Evaluation (APACHE) II ≥15 (n = 35) were randomized to receive either placebo or intravenous selenite as a bolus-loading dose of 2,000 μg Se followed by continuous infusion of 1,600 μg Se per day for 10 days. Blood samples were analyzed before randomization (day 0) then at days 3, 7, and 10. Clinical outcome was assessed by Sequential Organ Failure Assessment (SOFA) score. Hospital-acquired pneumonia including ventilator-associated pneumonia (VAP), adverse events, and other safety parameters were monitored as secondary endpoints.
Results
SOFA score decreased significantly in the selenite group at day 10 (1.3 ± 1.2 versus 4.6 ± 2.0, p = 0.0001). Early VAP rate was lower in the selenite group (6.7% versus 37.5%, p = 0.04), and hospital-acquired pneumonia was lower after ICU discharge (p = 0.03). Glutathione peroxidase-3 (GPx-3) activity increased in both groups, reaching a maximum at day 7 (0.62 ± 0.24 versus 0.28 ± 0.14 U/mL, p = 0.001) in the selenite group. No adverse events attributable to selenite were observed.
Conclusions
Daily infusion of 1,600 μg Se (as selenite), following an initial bolus of 2,000 μg, is novel and without short-term adverse events. High-dose parenteral selenite significantly increases Se status, improves illness severity, and lowers incidence of hospital-acquired pneumonia including early VAP for SIRS patients in ICU.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Systemic inflammatory response syndrome (SIRS) involves a chain of events culminating in migration of neutrophils into inflamed tissue to release free radicals. In the lower respiratory tract SIRS is characterized by capillary congestion, leukocyte and macrophage infiltration into alveolar spaces. An inflammatory response accompanying hospital-acquired pneumonia in intensive care unit (ICU) patients with acute respiratory failure more than 48h after intubation is defined as ventilator associated pneumonia (VAP) [1]. VAP is a major event affecting up to 30% of the most vulnerable patients [2], increasing morbidity, mortality, length of stay (LOS), and costs [3]. Therapies to counteract the inflammation and reduce the occurrence of VAP are therefore attractive [4].
The trace element selenium (Se) has antioxidant, anti-inflammatory, and immunological functions [5, 6]. It is an important constituent of the glutathione peroxidase (GPx) selenoenzymes, consisting of eight isoforms that differ in their substrate specificity. GPx-3 accounts for 20–40% of total plasma Se [7] with a normal value for our Uruguayan subjects of 0.72 ± 0.16 U/mL [8]. Severe sepsis/septic shock are characterized by inflammation with high levels of circulating cytokines, reactive oxygen species (ROS), and phagocytic hyperactivity from polymorphonuclear neutrophils (PMN) due to delayed apoptosis and prolonged NF-κB activation [9]. Intravenous selenite has a biphasic action: firstly as a pro-oxidant and, after incorporation into selenoenzymes, as an antioxidant [7]. High concentrations of selenite inhibit DNA-binding activity of NF-κB in vitro, by reacting with its thiol groups [10, 11]. As an antioxidant and anti-inflammatory agent, Se is potentially important in SIRS [12–15].
Our previous supplementation study [16], showed that 2,000 µg (25.30 µmol) Se, administered as selenious acid by bolus, followed by daily continuous infusion of 1,600 µg (20.24 µmol) Se for 10 days, normalized GPx-3 activity from day 3 onwards without adverse events or increased mortality [16].
The purpose of this study is to confirm the pharmacodynamics and further evaluate the effectiveness of high-dose Se therapy, as an initial bolus of selenite, followed by continuous infusion, on illness severity, adverse events, and clinical outcome in SIRS patients.
Methods
Study design
This phase II prospective, placebo-controlled, randomized, single-center investigation planned to study 40 patients and evaluate the feasibility of a more powerful phase III safety and efficacy trial. Sample size was calculated on the basis of a type I error of 5% and a power of 80% to detect an increase in GPx-3 activity of 0.5 U/mL at day 10. Inclusions criteria were: SIRS patients with a minimal Acute Physiology and Chronic Health Evaluation (APACHE) II score ≥15 and predicted mechanical ventilation (MV) for >48 h. Exclusions were: age <18 years, pregnancy, brain injury after cardiopulmonary arrest, malignant disease, immune deficiency, chronic renal failure, participation in another trial, limitation of care, and refusal. The hospital Ethics Committee for Medical Research approved the protocol. Informed consent was obtained from all participants or their relatives before enrolment.
Patients were blinded to the intervention, and randomized within the first 24 h of ICU admission into two groups, receiving either high-dose selenious acid (Laboratories Rivero®, Buenos Aires, Argentina) in 0.9% sodium chloride solution (NaCl) or placebo. The selenite group received a bolus loading dose of 2,000 µg (25.30 µmol) Se over 2 h within 2 h after enrolment, and thereafter 1,600 µg/day (20.24 µmol/day) Se as a daily continuous infusion for 10 days (total dose of Se 18 mg, 227.7 µmol). Selenious acid ampoules, containing 400 µg Se per 10 ml (40 µg, 0.51 µmol/mL), were aseptically added to 250-mL bottles of 0.9% NaCl and administered by 24 h continuous infusion at 10 mL/h. Controls just received 0.9% NaCl. Serum samples in trace-element-free polyethylene vials were frozen at −20°C until analysis. GPx-3 activity was determined on days 0, 3, 7, and 10. Se measurements were not considered necessary because we had previously demonstrated that Se levels remained within the normal range during 10 days supplementation with this dose [16].
Clinical data
SIRS was diagnosed according to the ACCP/SCCM consensus [17]. Severity of illness was assessed by APACHE II and Sequential Organ Failure Assessment (SOFA) scores. SOFA was used for assessing organ dysfunction and clinical outcome. Hematological, biochemical, blood gas analyses, PaO2/FiO2 (P/F) ratio, and cultures from blood and infection sites were routine.
VAP was defined by a new and persistent chest X-ray infiltrate (unilobar, unilateral or bilateral) in patients receiving MV for at least 48 h, with two of three of the following: temperature >38°C or <35.5°C; white blood cell count >10,000/μL or <4,000/μL; new purulent respiratory secretions, confirmed with semiquantitative cultures of tracheal aspirate. According to our routine criteria, the cutoff point, which selectively excluded any persisting episodes of community-acquired pneumonia, was: early VAP ≤5 days, late VAP >5 days.
The details of organ dysfunction definition and GPx-3 determination are shown in the Electronic Supplementary Material.
Researchers did not direct medical, surgical or nutritional therapy. Standard protocols for enteral nutrition (EN) or parenteral nutrition (PN) were utilized within 48 h after admission. Protocol violations were predefined as: insufficient daily Se dose, interruption of Se administration for more than 12 h, or loading dose delay more than 2 h after inclusion.
Adverse events analysis
In addition to ICU and hospital mortality, adverse events potentially related to the selenite bolus were recorded and analyzed independently, including: seizures, brain injury (ischemic or hemorrhagic), acute brain dysfunction (at least one episode of an acute and fluctuating disturbance of consciousness and cognition), anemia, thrombocytopenia, severe arterial hypotension, acute respiratory distress syndrome (ARDS) [18], HD, acute kidney injury (AKI), and refractory shock [persistent circulatory failure with mean arterial pressure (MAP) <65 mmHg in spite of fluid resuscitation and norepinephrine 0.2 gamma/kg/min, associated with persisting lactic acidosis]. EN intolerance was defined by gastric residual volume ≥600 mL/day (measured every 4 h), vomiting, abdominal distension or ileus (our standard protocol prior to publication of the ASPEN-SCCM guidelines) [19].
Statistics
Data analysis was performed on an intention-to-treat (ITT) basis. Results are expressed as mean values ± standard deviation (SD) for continuous variables and as percentages for qualitative variables. Differences between groups and analysis of nonparametric continuous variables were assessed using the Mann–Whitney U test. Changes over time were compared using two-factor repeated-measures analysis of variance (ANOVA) for the effect of group, time, and treatment. Post hoc comparisons were carried out by Dunnett’s tests (effect of time versus baseline). Categorical variables were analyzed with chi-square test. For correlations, linear regression analysis, nonparametric Pearson correlation coefficient or Spearman tests were used, and the corresponding r 2 was calculated. Kaplan–Meier curves compared all pneumonias, and the effect of treatment was analyzed using the log-rank test.
p < 0.05 was considered to be statistically significant. Statistical analysis was carried out using SPSS 17.0 software (SPSS, Chicago, IL, USA) for Windows.
Results
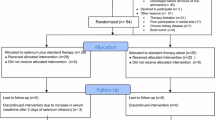
Between December 2006 and January 2008, 40 patients were considered for enrolment, and 35 were randomized. The mean time between admission and start of intervention was 16 ± 6 versus 13 ± 6 h (p = 0.29) in selenite and placebo group, respectively. All patients were followed up for the entire study (Supplementary Fig. 1) except one selenite patient and three placebo patients, later excluded because of errors in enrolment criteria. One additional placebo group patient, who died within 48 h, was included in the final analysis according to the ITT principle. Baseline characteristics and daily EN Se (77 ± 21 µg versus 73 ± 16 µg, p = 0.85) (Table 1) were similar.
Clinical
Early VAP was diagnosed in one (6.7%) patient in the selenite group and six (37.5%) patients in the placebo group (p = 0.04). Late VAP incidence was similar in the two groups (13.3% versus 6.3%, p = 0.68), but hospital-acquired pneumonia at 28 days after ICU discharge was observed only in the placebo group (three episodes, p = 0.03) (Table 2). The time to occurrence of hospital-acquired pneumonia (including VAP) indicates that the proportion of patients without pneumonia was higher in the selenite group (p = 0.024, by stratified log-rank test) (Fig. 1).

Kaplan–Meier plot for all episodes of hospital-acquired pneumonia occurring in the first 28 days in both groups. Red line represents selenium supplemented group, and blue line represents placebo group. Log rank: p = 0.024
There was no significant difference between the groups (selenite versus placebo, respectively) in terms of days of antibiotic use (8.8 ± 5.3 versus 9.5 ± 2.5, p = 0.19), days of catecholamines therapy (2.1 ± 1.4 versus 4.0 ± 4.3, p = 0.69), AKI incidence (44% versus 50%, p = 0.82), days of insulin therapy (1.8 ± 3.4 versus 3.4 ± 4.5, p = 0.42), ICU LOS (14 ± 11 versus 13 ± 6 days, p = 0.56), ICU mortality (20% versus 31%, p = 0.55) or hospital discharge mortality (33.3% versus 43.5%, p = 0.95). No patients required RRT. The P/F index and SOFA respiratory scores did not differ between groups (Table 2).
SOFA score reduced in both groups with a negative, but not significant, correlation with GPx-3 at admission (r 2 = 0.084, p = 0.09). There was no significant difference on day 3 (5.7 ± 3.3 versus 5.6 ± 2.9, p = 0.75), but the mean SOFA score decreased significantly only in the selenite versus placebo group, respectively (1.3 ± 1.2 versus 4.6 ± 2.0, p = 0.0001) at day 10 (Table 3, Fig. 2).

Evolution of SOFA scores. At day 10, SOFA score decreased significantly in the selenite group (1.3 ± 1.2 versus 4.6 ± 2.0, p = 0.01, in the selenite and placebo group, respectively)
Pharmacodynamics
At day 3, GPx-3 activity was 0.52 ± 0.28 versus 0.26 ± 0.08 U/mL (p = 0.001), at day 7 it was 0.62 ± 0.24 versus 0.28 ± 0.14 U/mL, (p = 0.001), and at day 10 it was 0.39 ± 0.09 versus 0.27 ± 0.09 (p = 0.09) for selenite and placebo groups, respectively. Maximum levels were achieved at day 7 in both groups, but were significantly higher and only reached normal in the selenite group. GPx-3 subsequently decreased between day 7 and 10, despite continued selenite supplementation (Fig. 3).

GPx-3 pharmacodynamics profile during the study period. In the selenite group, GPx-3 increased until day 7 (at day 7: 0.62 ± 0.24 versus 0.28 ± 0.14, p = 0.001 in the selenite and placebo group, respectively) and then declined to day 10, despite continued supplementation. Solid and broken lines represent mean ± SD normal GPx-3 activity. Normal range for healthy subjects: 0.72 ± 0.16 U/mL. GPx-3 glutathione peroxidase-3
Adverse events
No adverse events potentially attributable to selenite were noted (Table 4), and GPx-3 activity never exceeded our upper normal range (Fig. 3). The incidence of AKI, refractory shock, severe arterial hypotension, ARDS, brain injury, seizures, delirium, anemia, thrombocytopenia, HD, and EN intolerance were similar during the bolus or continuous infusion.
Discussion
Our phase II study in SIRS patients has demonstrated that high-dose selenious acid administered first as a bolus, providing 2,000 µg (25.3 µmol) Se over 2 h, and thereafter 1,600 µg/day (20.24 µmol) Se as a continuous infusion, lowered SOFA scores, reduced the occurrence of early VAP, and decreased the episodes of hospital-acquired pneumonia after ICU discharge [20]. Se was efficacious in maximizing serum GPx-3 at day 7, and was not associated with a higher incidence of adverse events during 28 days follow-up.
The contribution of VAP to morbidity, mortality, and ICU costs makes prevention an imperative. Se pharmaconutrition is now proposed as a new strategy for incorporation into care bundles for VAP prevention [21].
Pulmonary injury results from an interaction of PMN with endothelial cells. Within minutes of injury, macrophages release neutrophils and inflammatory cytokines, which interact with the walls of postcapillary venules. Lung endothelial cells are stimulated to express surface adhesion molecules, which bind to circulating neutrophils, facilitating their migration into the interstitium and the alveolus, whilst concomitantly triggering a burst of free radicals into the lungs [22].
Immune function is often suboptimal in Se deficiency, the functions of neutrophils and macrophages are impaired, and bacteria adhere to the respiratory mucosa, leading to infection [23] and increased incidence of multiple organ failure (MOF) and hospital-acquired pneumonia (16% versus 3.9%) in patients with low Se (<0.6 μmol/L) [14]. However, can repletion of Se stores minimize these common complications in the critically ill? Aggregating results from two randomized supplementation trials, Berger et al. [24] found that enhancing trace elements status with zinc, copper, and Se (315–380 μg/day) in burns patients was associated with a decrease of hospital-acquired pneumonia (80% versus 33%, p < 0.001) and fewer VAP episodes (13 versus 6, p = 0.023). Subsequently, they showed that trace elements reduced infectious complications in the first 30 days, primarily related to a lower number of pulmonary infections (18 versus 9, p = 0.03) [25]. Additionally, results from the Scottish Intensive Care Glutamine or Selenium Evaluative Trial (SIGNET) [26] showed a significant [odds ratio 0.53 (0.30 to 0.93)] reduction in the incidence of pneumonia when selenite (500 µg/day) was given in PN for at least 5 days.
However, none of these trials reduced mortality, and none utilized the bolus loading dose of selenite that could stimulate the anti-inflammatory process in SIRS. Evidence supporting this concept comes from the Selenium in Intensive Care (SIC) study [27], which did incorporate an initial bolus in the regimen. Per-protocol analysis confirmed that a bolus of 1,000 µg selenite on the first day, followed by daily continuous infusion of 1,000 µg Se for 14 days, reduced 28-day mortality in septic patients, but as in our study, Se did not reduce length of MV [27].
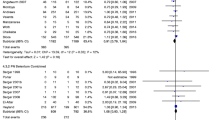
The first meta-analysis of antioxidant supplementation trials in ICU revealed a tendency to decreased mortality with Se doses higher than 500 µg/day [relative risk (RR) 0.52, 95% confidence interval (CI) 0.24–1.14, p = 0.10] [28]. However, the updated meta-analysis, incorporating a new study (see below) that did not administer a loading bolus dose, confirmed that Se decreases mortality but not significantly (RR 0.84, 95% CI 0.67–1.05, p = 0.13) [29].
Forceville et al. [30] administered 4,000 µg Se as sodium selenite in the first 24 h by continuous infusion, but with no initial bolus, followed by 1,000 µg/day for 9 days, but could not reduce mortality nor the incidence of pneumonia in septic shock (45% placebo versus 55% Se; p = 0.438). This contrasts with previous achievements, leading the authors to speculate that the different results are due to omission of this initial pro-oxidant bolus-loading dose of selenite [7]. Animal research by the same investigators [31, 32] adds further weight to this hypothesis. A Se bolus (2,000 µg), as selenite, was associated with improved hemodynamics and response to fluid replacement (p < 0.05), in a sheep model of septic shock [31]. Most recently, Schäper et al. [32] reported that a selenite bolus (0.4 mg/kg) in endotoxemic rats may have a beneficial effect on leukocyte–endothelium interaction by improving microcirculation.
A selenite bolus could have three effects: (a) reversible inhibition of NF-κB binding to DNA [10, 11], (b) induction of apoptosis and cytotoxicity in activated pro-inflammatory cells, and (c) a direct virucidal or bactericidal effect [7], and each could contribute to our observed reduction in the incidence of early VAP [20].
Our small study did not show any significant differences in mortality, gas exchange or respiratory SOFA score. However, the overall reduction in SOFA score confirms the finding by Mishra et al. [33], albeit using a lower dose (50 µg per day decreasing to 32 µg per day over 14 days), suggesting that Se supplementation greater than the recommended daily amount (RDA), may lead to more rapid resolution of MOF. The trend towards increased length of MV and LOS for supplemented patients, but without any significant difference in the incidence of respiratory failure, could be due to a higher (but not significant) incidence of late VAP in the Se group (13.3% versus 6.3%, p = 0.68) and a trend toward a decline in ICU mortality (20% versus 31%, p = 0.47).
Our novel data endorse the therapeutic approach originated by the SIC study [27] and support the theory that the pro-oxidant effect of a large selenite bolus prior to continuous infusion may be anti-inflammatory and hence clinically beneficial. High-dose Se therapy has been advocated in severe sepsis/septic shock [7, 16, 27, 30, 34], and recent guidelines support the use of this pharmaconutrient [19, 35]. However, the safety of pharmacological doses of an active substrate is of paramount importance. It has been suggested that Se doses greater than 400 µg/day could be harmful [15], but this is the 1996 World Health Organization (WHO) tolerable upper intake level (TUIL) for daily oral intake (>3 months) in healthy subjects. Maximum acute doses up to 800 μg/day have been proposed [36] but without evidence that higher doses are unsafe. Experimental data suggest negligible respiratory excretion of Se metabolites at doses <100 µg/kg, with toxic symptoms only occurring at doses >1,000 µg/kg [37]. Se toxicosis results from long-term oral intakes up to 38,000 μg/day by populations living in seleniferous regions [38], but no selenosis has been reported from bolus injection or continuous infusion over 5–14 days to critically ill SIRS patients.
Supplementing with 1,600 µg/day, following a bolus of 2,000 µg, and taking into account the EN contribution, our patients received a total of 19,000 µg over 10 days. Although this amount is five times the TUIL, it is approximately half the daily intake recorded for induction of selenosis, and is comparable to the mean highest doses in half the studies on depleted patients reviewed by Andrews [39]. We observed no acute toxicity symptoms and no higher incidence of adverse events (Table 4).
Selenite pharmacodynamics in SIRS patients confirmed increased GPx-3 activity from day 1 through day 3 to a maximum at day 7, within our previously published [8, 16] physiological range for non-SIRS and healthy subjects (0.61 ± 0.13 to 0.72 ± 0.16 U/mL), then declining to day 10, despite continued supplementation. Similarly, Valenta et al. [40] report, without comment, a decrease in whole-blood GPx from day 10, notwithstanding an initial selenite bolus of 1,000 µg Se on day 1 and 14 days supplementation at 500 µg/day.
This enzyme inhibition or saturation could be due to insufficient synthesis of precursors such as hydrogen selenide or selenocysteine, and/or limitation of glutathione (GSH) synthesis by lack of glutamine or cysteine. We therefore hypothesize that depleted GSH or precursor stores need to be replenished to maintain GPx-3 intracellular levels in SIRS [34].
Our study has limitations: ICU admissions were heterogeneous; small patient sample size means the protocol was insufficiently powered to show a real benefit on VAP incidence or mortality; serum Se, biomarkers of oxidative stress, and pro-inflammatory response were not measured. Nevertheless, our strategy of administering a bolus-loading dose, followed by daily continuous infusion, was free of short-term adverse events, and acute toxicity. The therapy is capable of decreasing illness severity in SIRS patients, as evaluated by SOFA score at day 10, can significantly reduce early VAP, and potentially decreases the incidence of pneumonia at discharge.
Conclusions
This pilot study demonstrates that an initial loading bolus of 2,000 μg selenite followed by high-dose selenite as a continuous infusion providing 1,600 μg selenite per day was efficacious for critically ill patients with systemic inflammation. Selenium therapy significantly improved illness severity and early VAP with no obvious adverse events indicative of toxicity whilst lowering the incidence of pneumonia post ICU discharge. In our opinion, this therapeutic approach is sufficiently robust to seek confirmation in a more adequately powered clinical trial and to evaluate synergistic combinations of pharmaconutrients such as glutamine, cysteine, and selenium that could prolong GPx-3 levels with potential improvements in clinical outcome.
References
Meduri GU, Johanson WG (1992) International consensus conference: clinical investigation of VAP. Chest 102:551S–552S
Young G, Ridley SA (1999) Ventilator-associated pneumonia. Anaesthesia 54:1183–1197
Safdar N, Dezfulian C, Collard HR, Saint S (2005) Clinical and economic consequences of ventilator-associated pneumonia: a systematic review. Crit Care Med 33:2184–2193
Rello J, Ollendorf DA, Oster G, Vera-Llonch M, Bellm L, Redman R, Kollef MH, VAP Outcomes Scientific Advisory Group (2002) Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest 122:2115–2121
Rayman MP (2000) The importance of selenium to human health. Lancet 356:233–241
Hardy G, Hardy I (2004) Selenium: the Se-XY nutraceutical. Nutrition 20:590–593
Vincent JL, Forceville X (2008) Critically elucidating the role of selenium. Curr Opin Anaesthesiol 21:148–154
Manzanares W, Biestro A, Galusso F, Torre MH, Mañay N, Pittini G, Facchín G, Hardy G (2009) Serum selenium and glutathione peroxidase-3 activity: biomarkers of systemic inflammation in the critically ill. Intensive Care Med 35:882–889
Kim IY, Stadtman TC (1997) Inhibition of NF-kB DNA binding and NO induction in human T cells and lung adenocarcinoma cells by selenite treatment. Proc Natl Acad Sci USA 94:12904–12907
Kretz-Remy C, Arrigo AP (2001) Selenium: a key element that controls NF-κB activation and IκBα half-life. BioFactors 14:117–125
Maehira F, Miyagi I, Eguchi Y (2003) Selenium regulates transcription factor NF-kB activation during the acute phase reaction. Clin Chem Acta 334:163–171
Eaton S (2006) The biochemical basis of antioxidant therapy in critical illness. Proc Nutr Soc 65:242–249
Berger MM (2005) Can oxidative damage be treated nutritionally? Clin Nutr 24:172–183
Forceville X, Vitoux D, Gauzit R, Combes A, Lahilaire P, Chappuis P (1998) Selenium, systemic immune response syndrome, sepsis and outcome in critically ill patients. Crit Care Med 26:1536–1544
Shenkin A (2009) Selenium in intravenous nutrition. Gastroenterology 137:S61–S69
Manzanares W, Biestro A, Galusso F, Torre MH, Mañay N, Facchín G, Hardy G (2010) High-dose selenium for critically ill patients with systemic inflammation: a pilot study. Nutrition 26:634–640
Members of the American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference (1992) Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 20:864–873
Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, Legall JR, Morris A, Spragg R (1994) The American-European consensus conference on ARDS. Definition, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 149:818–824
Martindale RG, McClave SA, Vanek VW, McCarthy M, Roberts P, Taylor B, Ochoa JB, Napolitano L, Cresci G, American College of Critical Care Medicine, A.S.P.E.N. Board of Directors (2009) Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: society of critical care medicine and American society of parenteral and enteral nutrition. Crit Care Med 37:1751–1761
Manzanares W, Biestro A, Torre MH, Galusso F, Facchín G, Hardy G (2009) Clinical effects of high dose selenious acid in critically ill patients with systemic inflammation. J Parent Enteral Nutr 33:186 (Abstr. S36–34)
Rello J, Lode H, Cornaglia G, Masterton R, VAP Care Bundle Contributors (2010) A European care bundle for prevention of ventilator-associated pneumonia. Intensive Care Med 36:773–780
Weiss SJ (1989) Tissue destruction by neutrophils. N Engl J Med 329:365–376
Rao L, Puschner B, Prolia TA (2001) Gene expression profiling of low selenium status in the mouse intestine. J Nutr 131:3175–3181
Berger MM, Eggimann P, Heyland DK, Chioléro RL, Revelly JP, Day A, Raffou W, Shenkin A (2006) Reduction of nosocomial pneumonia after major burns by trace element supplementation: aggregation of two randomised trials. Critical Care 10:R153
Berger MM, Baines M, Raffoul W, Benathan M, Chiolero RL, Reeves C, Revelly JP, Cayeux MC, Sénéchaud I, Shenkin A (2007) Trace element supplementation after major burns modulates antioxidant status and clinical course by way of increased tissue trace element concentrations. Am J Clin Nutr 85:1293–1300
Andrews PJD, Avenell A, Noble DW, Campbell MK, Croal BL, Simpson WG, Vale LD, Battison CG, Jenkinson DJ, Cook JA, and the SIGNET Trials Group (2011) Randomised trial of glutamine, selenium, or both, to supplement parenteral nutrition for critically ill patients. BMJ 342:d1542. doi:10.1136/bmj.d1542. Epub ahead of print
Angstwurm MWA, Engelmann L, Zimmermann T, Lehmann C, Abel P, Strauss R, Meier-Hellmann A, Insel R, Radke J, Schuttler J, Gartner R (2007) Selenium in Intensive Care (SIC) study. Results of a prospective, randomized, placebo-controlled, multiple-center study in patients with severe systemic inflammatory response syndrome, sepsis, and septic shock. Crit Care Med 35:118–126
Heyland DK, Dhaliwal R, Suchner U, Berger MM (2005) Antioxidant nutrients: a systematic review of trace elements and vitamins in the critically ill patient. Intensive Care Med 31:327–337
Canadian clinical practice guidelines for nutrition support in mechanically ventilated, critically ill adult patients. Supplemental antioxidants nutrients: parenteral selenium (2009) http://www.criticalcarenutrition.com. Last access: April 2010
Forceville X, Laviolle B, Annane D, Vitoux D, Bleichner G, Korach JM, Cantais E, Georges H, Soubirou JL, Combes A, Bellissant E (2007) Effects of high doses of selenium, as sodium selenite, in septic shock: a placebo controlled, randomized, double-blind, phase II study. Crit Care 11:R73
Wang Z, Forceville X, Van Antwerpen P, Piagnerelli M, Ahishakiye D, Macours P, De Backer D, Neve J, Vincent JL (2009) A large bolus, but not a continuous infusion, of sodium selenite improves outcome in peritonitis. Shock 32:140–146
Schäper J, Samapaty R, Zakrzewicz A, Pries AR, Forceville X (2010) Effect of sodium selenite on LPS endothelial injury. Intensive Care Med 36(Suppl 2):S169
Mishra V, Baines M, Perry SE, McLaughlin PJ, Carson J, Wenstone R, Shenkin A (2006) Effect of selenium supplementation on biochemical markers and outcome in critically ill patients. Clin Nutr 26:41–50
Manzanares W, Hardy G (2009) Selenium supplementation in the critically ill. Posology and pharmacokinetics. Curr Opin Clin Nutr Metab Care 12:273–280
Singer P, Berger MM, Van den Berghe G, Biolo G, Calder P, Forbes A, Griffiths R, Kreyman G, Leverve X, Pichard C (2009) ESPEN Guidelines on parenteral nutrition: intensive care. Clin Nutr 28:387–400
Heyland DK (2007) Selenium supplementation in critically ill patients: can too much of a good thing be a bad thing? Crit Care 11:R153
Bopp BA, Sonders RC, Kesterson JW (1982) Metabolic fate of selected selenium compounds in laboratory animals and man. Drug Metab Rev 13:271–318
Glover JR, Chu B (1970) Selenium and its industrial toxicity. Indust Med Surg 39:50–54
Andrews P (2010) Selenium and glutamine supplements: where are we heading? A critical care perspective. Curr Opin Clin Nutr Met Care 13:192–197
Valenta J, Brodska H, Drabek T, Hendl J, Kazda A (2011) High-dose selenium substitution in sepsis: a prospective randomized clinical trial. Intensive Care Med. doi 10.1007/s00134-011-2153-0. Epub ahead of print
Acknowledgments
This work was supported in part by grant from the Comisión Sectorial para la Investigación Científica (CSIC)—UdeLaR and the Fondo Clemente Estable 2004/10.072, DyCIT. Ministerio de Educación y Cultura, Uruguay.
Conflict of interest
All authors declare no competing interests.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Manzanares, W., Biestro, A., Torre, M.H. et al. High-dose selenium reduces ventilator-associated pneumonia and illness severity in critically ill patients with systemic inflammation. Intensive Care Med 37, 1120–1127 (2011). https://doi.org/10.1007/s00134-011-2212-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-011-2212-6