
Abstract
Purpose
An International Consensus Conference proposed classifying weaning into simple, difficult, and prolonged weaning. However, the usefulness of this classification in a respiratory intensive care unit (ICU) is unknown. The aims of the study were: (1) to compare the clinical characteristics and outcomes of patients from the three weaning groups in a respiratory ICU; and (2) to assess predictors for prolonged weaning and survival.
Methods
We prospectively studied 181 mechanically ventilated patients (131, 72% with chronic respiratory disorders) in whom weaning had been initiated, divided into simple (78, 43%), difficult (70, 39%), and prolonged (33, 18%) weaning. We compared the characteristics and outcomes among the three groups and determined the factors associated with prolonged weaning and survival in multivariate analysis.
Results
Patients with simple and difficult weaning had similar characteristics and outcomes. A higher proportion of patients with prolonged weaning had chronic obstructive pulmonary disease, and these patients also had more complications, a longer stay and lower survival. Increased heart rate (≥105 min−1, p < 0.001) and PaCO2 (≥54 mmHg, p = 0.001) during the spontaneous breathing trial independently predicted prolonged weaning. In addition, the need for reintubation (p < 0.001) and hypercapnia during the spontaneous breathing trial (p = 0.003) independently predicted a decreased 90-day survival.
Conclusion
Because of the similar characteristics and outcomes, the differentiation between simple and difficult weaning had no relevant clinical consequences in a respiratory ICU. Patients with prolonged weaning had the worst outcomes. For the overall population, hypercapnia at the end of spontaneous breathing predicts prolonged weaning and a worse survival, and clinicians should implement measures aimed at improving weaning outcome.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Weaning from mechanical ventilation (MV) is a challenging period that represents 40–50% of the duration of MV [1–4], and furthermore there is an increasing burden on the health-care system related to prolonged MV [5]. Different approaches have been proposed to optimize the weaning process [6, 7], including weaning protocols [3, 8, 9], automated systems [10], daily spontaneous breathing trials (SBT) [11], and pressure-support ventilation [12]. In spite of this, it is estimated that 20–30% of patients cannot be extubated at the first weaning attempt [2, 6].
An International Consensus Conference (ICC) on weaning from MV [6] proposed a new classification based on the difficulty and duration of the weaning period: simple, difficult, and prolonged weaning. Although it is considered that prolonged weaning is associated with the lowest survival [13, 14], this classification was based solely on expert opinion. Moreover, previous studies have analysed the factors associated with prolonged MV [15] and reintubation [16], but the factors involved in prolonged weaning have not yet been assessed. The identification of these factors could be important in influencing the survival of ventilated patients in whom weaning has been initiated. The ICC recommended further research on the basis of careful testing and scrutiny of groups of patients who undergo weaning, and stressed the need for studies assessing the outcome of patients with difficult and prolonged weaning [6].
A recent study in medical and surgical intensive care units (ICU) has shown that prolonged weaning is associated with increased mortality and morbidity [17]. However, the proportion of difficult and prolonged weaning is low in the general ICU population [2, 6]. Moreover, factors associated with prolonged weaning were not assessed in that study [17]. Applying this classification in specific settings with higher proportions of difficult and prolonged weaning would add valuable information regarding the factors associated with prolonged weaning. A large proportion of patients admitted to respiratory ICUs have chronic respiratory disorders, which are associated with a longer duration of weaning [6, 12]. Consequently, a respiratory ICU seems an optimal setting to assess the outcome of patients with difficult and prolonged weaning due to the expected higher proportion of such patients compared with the general ICU population [6]. In fact, chronic respiratory failure is more frequent in patients with prolonged weaning [17].
The aims of the present study were: (1) to compare the clinical characteristics and outcomes of patients with simple, difficult and prolonged weaning in a respiratory ICU; and (2) to determine predictive factors associated with prolonged weaning and its potential association with mortality, as this was expected in the group with worst outcomes [6].
Methods
Patients
In this prospective observational study, patients intubated and mechanically ventilated for more than 48 h were considered eligible when the following criteria for initiating weaning were fulfilled [18–20]: (1) improvement or resolution of the underlying causes of acute respiratory failure; (2) no fever (≥38°C) or hypothermia (<35°C); (3) blood haemoglobin concentration ≥70 g/l; (4) haemodynamic stability; (5) alertness and ability to communicate after discontinuing sedation; and (6) arterial O2 tension >60 mmHg with fraction of inspired oxygen (FIO2) ≤0.4 and positive end-expiratory pressure ≤5 cmH2O. For the purposes of this study, patients with previous tracheostomy were not considered eligible, and patients were excluded on the basis of the following criteria: (1) scheduled use of non-invasive ventilation (NIV) to facilitate the weaning process; (2) lack of cooperation for reliable measurements during the SBT; and (3) a previous decision to limit life-sustaining treatments. The study was approved by the Ethics Committee of the institution, but informed consent was not required.
Setting
The study was conducted in the Respiratory ICU of Hospital Clinic, Barcelona. This six-bed ICU serves patients with severe acute respiratory failure needing either invasive ventilation or NIV, difficult weaning with either NIV or tracheostomy, and monitoring. Patients with other non-respiratory organ system failures are also attended.
Study protocol
A SBT was performed with a T-piece. Prior to the SBT, assisted-control or pressure-support ventilation was used depending on the patient’s preference or tolerance. We defined SBT failure as the presence and persistence of one of the following criteria [18–20]: (1) respiratory frequency >35 min−1; (2) arterial O2 saturation by pulse oximetry <90% at FIO2 ≥0.40; (3) heart rate >140 or <50 min−1, or increases or decreases of more than 20% compared to MV; (4) systolic blood pressure >180 or <70 mmHg, or increases or decreases of more than 20% compared to MV; (5) decreased consciousness, agitation or diaphoresis; and (6) thoracic-abdominal paradoxical movement. If no signs of SBT failure appeared after 30–120 min [13, 18–20], the trial was considered successful. If the patient had adequate mental status, adequate cough, and ability to expectorate, extubation was performed. Alternatively, if signs of spontaneous breathing failure appeared during this period, the patient was reconnected to the ventilator, and other attempts were performed on subsequent days if the patient still fulfilled the inclusion criteria. If the patient could not be disconnected from MV after several attempts without positive evolution of the weaning process, a tracheostomy was considered [21]. Tracheostomy was also performed after reintubation if the patient was unable to clear or remove secretions.
Definitions
The weaning process included the period from the first SBT to extubation. If a tracheostomy was performed, the weaning period was considered finished at the point when the patient had bee breathing spontaneously for at least 48 h without ventilatory support. Patients were divided into three groups as previously described [6]: (1) simple weaning (patients who proceeded from initiation of weaning to extubation on the first attempt without difficulty); (2) difficult weaning (patients who failed initial weaning and required up to three SBT or as long as 7 days from the first SBT to achieve successful weaning); and (3) prolonged weaning (patients who failed at least three weaning attempts or required >7 days of weaning after the first SBT).
The patient was immediately reintubated if any of the following major events occurred: respiratory or cardiac arrest, respiratory pauses with loss of consciousness or gasping for air, psychomotor agitation inadequately controlled by sedation, massive aspiration, persistent inability to remove respiratory secretions, heart rate below 50 min−1 with loss of alertness, and severe haemodynamic instability without response to fluids and vasoactive drugs [18–20]. In addition to the immediate reintubation criteria, respiratory failure after extubation was also defined as the presence and persistence, within 48 h of extubation, of at least two of the following: (1) respiratory acidosis (arterial pH <7.35 plus PaCO2 >45 mmHg); (2) arterial O2 saturation by pulse oximetry <90% or PaO2 <60 mmHg at inspired O2 fraction ≥0.5; (3) respiratory frequency >35 min−1; (4) decreased consciousness, agitation or diaphoresis; and (5) clinical signs suggestive of respiratory muscle fatigue and/or increased work of breathing, such as the use of respiratory accessory muscles, paradoxical abdominal motion, or retraction of the intercostal spaces [19, 20, 22]. NIV was used to avoid reintubation in the patents with respiratory failure after extubation if immediate reintubation was not necessary [19, 20].
Ventilator-associated pneumonia (VAP) was defined as pneumonia that arises more than 48 h after endotracheal intubation [23]. For this study, only VAP episodes occurring after the onset of weaning were registered.
Data collection
All relevant data from the medical records and bedside flow charts of patients were reviewed at admission, including the Acute Physiology and Chronic Health Evaluation II (APACHE-II) score [24], and at the onset and the end of the weaning process. Patient follow-up was extended to 90 days. Physiological parameters were obtained on the day the weaning process was started.
Statistical analyses
Sample size estimation
The main outcome of our study was mortality. No previous studies had assessed mortality using the ICC classification when we started collecting patients. We estimated from a previous study [18] that 23% of the patients in our respiratory ICU required prolonged weaning. Assuming the ICU mortality rates estimated for the different weaning groups in the ICC report [6], we expected to include at least 178 patients to observe differences in the main outcome [confidence level (1 − α) 95%, power level (1 − β) 80%].
Comparison between the three groups
Data were analysed with SPSS 16.0 and are presented as number (percentage) or mean ± SD unless otherwise stated. Quantitative continuous variables were compared among the three groups using one-way analysis of variance, with Tukey post hoc comparisons. Categorical variables were compared using the chi-squared test. The level of significance was set at 0.05.
Risk factors for prolonged weaning and mortality
To assess the risk factors for prolonged weaning, patients were divided in prolonged and non-prolonged (simple plus difficult) weaning. Univariate and multivariate analyses were performed with logistic regression. Receiver operating characteristics curves were made to determine the optimal cut-off values of quantitative variables. Univariate and multivariate analyses of 90-day survival were performed with Cox proportional hazard regression. A conditional stepwise forward model (p in <0.10, p out <0.05) was used to correct for colinearity, and adjusted odds ratios and 95% confidence intervals were computed for variables independently associated with these events in all multivariate analyses.
Results
Patient characteristics
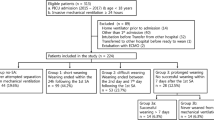
We included 181 consecutive patients over a 5-year period: 78 (43%) with simple, 70 (39%) with difficult, and 33 (18%) with prolonged weaning (Fig. 1). The baseline characteristics of the patients are summarized in Table 1. Except for a higher proportion of patients with chronic obstructive pulmonary disease (COPD) or chronic bronchitis who required prolonged weaning (p = 0.018), the patient characteristics were similar between the three groups. Pulmonary function tests were available in 70 patients with chronic respiratory disorders (53%), without differences between the three groups.

Schematic representation of the studied population. Non-eligible patients were those who, prior to the start the weaning process, had died during the inclusion period, had been transferred to other units or hospitals, or had had a tracheostomy. The main reasons for excluding patients were scheduled use of NIV to facilitate the weaning process (n = 105), lack of cooperation that impeded reliable measurements during the SBT (n = 25), previous decision to limit life-sustaining treatments (n = 18). Two patients with relevant data missing were also excluded
The physiological parameters on the day of the first SBT are shown in Table 2. Patients with simple and difficult weaning were similar. Patients with prolonged weaning had a higher PaCO2 (p = 0.006) and heart rate (p = 0.044), and a tendency to a lower arterial pH and oxygenation during MV prior to the SBT. Likewise, the frequency-to-tidal volume ratio at the beginning of the SBT was higher in this group (p = 0.002). At the end of the SBT in patients with prolonged weaning, PaCO2 (p = 0.001), heart rate (p < 0.001) and systolic blood pressure (p = 0.013) were also higher, and arterial pH lower (p = 0.001), with a tendency to lower oxygenation.
Length of stay and complications
Patients with prolonged weaning had longer duration of ventilation and stay, as well as a higher rate of subsequent VAP. These data are presented in (Table 3).
The rate of respiratory failure after extubation was higher in patients with prolonged weaning (p = 0.031), with a trend to a higher rate among patients with difficult weaning compared with simple weaning. The proportion of patients who needed reintubation, including those with immediate criteria and those who failed treatment with NIV, tended to be higher in the prolonged weaning group. Tracheostomy during the course of weaning or after reintubation was more frequently performed among patients with prolonged weaning (p < 0.001). There were no significant differences between the simple and difficult weaning groups for any of these outcomes. When comparing patients with difficult weaning who failed one or more than one SBT, we did not find significant differences in any outcome variable.
Factors predicting prolonged weaning
Several variables were associated with prolonged weaning in the univariate analysis (Table 4). In the multivariate analysis, higher values of heart rate (p < 0.001) and PaCO2 at the end of the first SBT (p = 0.001) were independent predictors of prolonged weaning. Heart rate ≥105 min−1 and PaCO2 ≥54 mmHg had the best discriminative capacity to predict prolonged weaning. Figure 2 shows the individual values of PaCO2 at the end of the SBT for the three groups of patients.

Individual values of PaCO2 at the end of the SBT in patients from the three weaning groups. PaCO2 was significantly higher in the prolonged weaning group, compared with the simple and the difficult weaning groups (p = 0.001)
Analysis of survival
The ICU, hospital and 90-day mortalities were higher in the prolonged weaning group (Table 3; Fig. 3). No differences were observed between the simple and the difficult weaning groups.

Kaplan-Meier survival curves for patients over 90 days from entry into the study. The cumulative survival probability was significantly lower in the prolonged weaning group (log-rank test). No differences were observed between patients with simple and difficult weaning
Among the variables associated with decreased 90-day survival in the univariate analysis (Table 5), reintubation (p < 0.001) and higher PaCO2 at the end of the first SBT (p = 003) were independent predictors of decreased 90-day survival in the multivariate analysis. PaCO2 ≥45 mmHg had the best discriminative capacity to predict decreased 90-day survival.
Relationship between hypercapnia and outcome variables in patients with non-prolonged weaning
Since higher levels of PaCO2 were associated with both prolonged weaning and worse survival, we analysed separately patients with non-prolonged (simple plus difficult) weaning in order to compare those with and without hypercapnia during the SBT. Patients with hypercapnia had worse oxygenation during spontaneous breathing (p < 0.001), a higher rate of respiratory failure after extubation (p = 0.007, Fig. 4; although the reintubation rate was not significantly different), and a lower 90-day survival (p = 0.033), indicating that hypercapnia remained associated with worse clinical condition and outcomes even in the absence of prolonged weaning.

Rate of respiratory failure after extubation, reintubation, and 90-day survival in patients with non-prolonged (simple plus difficult) weaning comparing patients with and without hypercapnia during the first SBT
Discussion
Summary of results
Patients with prolonged weaning had more complications, longer stay and higher mortality than those with simple and difficult weaning. However, patients with simple and difficult weaning had similar outcomes. An increased cardiorespiratory stress (higher heart rate and PaCO2) during the first SBT were independently associated with prolonged weaning. Likewise, hypercapnia when breathing spontaneously and reintubation were independently associated with decreased 90-day survival.
Duration of the weaning process
The ICC has estimated that around 69% patients can be extubated at the first weaning attempt (simple weaning), while around 31% need more than one SBT (difficult plus prolonged weaning) [6]. In a recent prospective study in medical and surgical ICUs, 59% of patients were classified as simple, 26% as difficult, and 14% as prolonged weaning [17].
We prospectively evaluated for the first time the new classification into three groups proposed by the ICC [6] in a respiratory ICU. As expected, the rate of simple weaning in our study was lower (43%) than in previous studies [2, 6, 17]. This is explained by the higher proportion of patients with chronic respiratory disorders (72%), and particularly COPD or chronic bronchitis (52%) in our study, compared with 16% with chronic respiratory failure in the study by Funk et al. [17]. Patients in our respiratory ICU also have worse outcomes than medical and surgical ICU patients [17], with higher mortality rates for each of the three weaning categories. One potential explanation for this finding is the higher proportion of reintubated patients observed in all the groups in our study. In fact, reintubation was independently associated with higher mortality, as has been reported previously [25, 26].
As previously shown in medical and surgical ICU patients [17], no differences in mortality between simple and difficult weaning patients were observed in our respiratory ICU. The average total duration of MV were 1 day longer in patients with difficult weaning from our population than in those with simple weaning, but the difference did not reach statistical significance. As mortality increases with the duration of MV [4], this may explain the similar outcomes observed in the two groups of patients. Therefore, an initial failure of the SBT has no impact in outcome if patients are extubated in the next following days. Conversely, patients with prolonged weaning had substantially longer duration of MV, thus explaining the higher rate of complications associated with prolonged ventilation and mortality.
Higher PaCO2 and heart rate during the initial SBT were independently related to the prolongation of weaning. These findings are consistent with those of previous studies showing that patients develop increased cardiopulmonary stress during an unsuccessful SBT [27–31]. This is directly associated with the imbalance between ventilatory demands and capacity in patients who are not yet ready to be disconnected from the ventilator, which is influenced by many different factors [32]. However, the large overlap of PaCO2 values between patients from the three groups, as shown in Fig. 2, limits the discriminative value of this individual variable. Heart rate and PaCO2 during MV before the SBT were also higher in patients with prolonged weaning; this suggests that patients more likely to require prolonged weaning begin the weaning process in a worse condition than those less likely to.
Factors related to survival
Although prolonged weaning was associated with decreased 90-day survival, reintubation and hypercapnia during the SBT were the only independent predictors of 90-day mortality. Reintubation has already been described as an independent risk factor of hospital mortality [25]. The need for reintubation may serve as an additional independent marker of increased severity of illness, and may be aetiologically related to poor outcomes such as VAP [26]. The association of hypercapnia during a SBT with decreased survival has already been described in patients with persistent weaning failure [18]. In addition, patients with hypercapnia before extubation have poor outcomes when no ventilatory support is provided after extubation [19, 20, 33]. Increased PaCO2 therefore appears to be an accurate indicator of clinical deterioration after recovery from an acute episode of respiratory failure. Alternatively, this may also reflect the presence of advanced chronic respiratory disease, since hypercapnic patients had worse lung function than non-hypercapnic patients (their FEV1 was 34 ± 11% predicted and 48 ± 19% predicted, respectively, p = 0.008).
Potential clinical implications
If hypercapnia is detected while the patient is breathing spontaneously at onset of weaning, the clinician should implement measures such as the early application of NIV after extubation. This may help shorten the weaning period [18, 34] and prevent further respiratory deterioration [19, 20], resulting in improved survival in the respiratory ICU population. By contrast, using NIV to treat respiratory failure after extubation in mixed ICU populations is not efficient and may be harmful [22, 35].
Limitations
This study was conducted in a respiratory ICU of a single centre with a high proportion of patients with chronic respiratory disorders; this resulted in higher proportions of difficult and prolonged weaning than found in general ICU series [2, 17]. Although the most relevant findings of this study were also observed when patients with COPD and chronic bronchitis were excluded from the analysis, these results may not be extrapolated to other populations of critically ill patients. Moreover, the proposed PaCO2 thresholds to predict prolonged weaning and worse survival deserve further prospective validation.
Conclusion
In a respiratory ICU, patients with simple and difficult weaning had similar characteristics and outcomes; this differentiation has therefore no relevant clinical implications in this population. Patients with prolonged weaning had the worst outcomes. For the overall population, increased CO2 retention during spontaneous breathing strongly predicts prolonged weaning and worse survival. If high levels of PaCO2 are detected in the patient at the onset of weaning, the clinician should implement measures aimed at improving the outcome of weaning from MV.
References
Esteban A, Alia I, Ibañez J, Benito S, Tobin MJ; the Spanish Lung Failure Collaborative Group (1994) Modes of mechanical ventilation and weaning. A national survey of Spanish hospitals. The Spanish Lung Failure Collaborative Group. Chest 106:1188–1193
Esteban A, Ferguson ND, Meade MO, Frutos-Vivar F, Apezteguia C, Brochard L, Raymondos K, Nin N, Hurtado J, Tomicic V, Gonzalez M, Elizalde J, Nightingale P, Abroug F, Pelosi P, Arabi Y, Moreno R, Jibaja M, D’Empaire G, Sandi F, Matamis D, Montanez AM, Anzueto A (2008) Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med 177:170–177
Ely EW, Baker AM, Dunagan DP, Burke HL, Smith AC, Kelly PT, Johnson MM, Browder RW, Bowton DL, Haponik EF (1996) Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med 335:1864–1869
Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart TE, Benito S, Epstein SK, Apezteguia C, Nightingale P, Arroliga AC, Tobin MJ (2002) Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA 287:345–355
Zilberberg MD, de Wit M, Pirone JR, Shorr AF (2008) Growth in adult prolonged acute mechanical ventilation: implications for healthcare delivery. Crit Care Med 36:1451–1455
Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, Pearl R, Silverman H, Stanchina M, Vieillard-Baron A, Welte T (2007) Weaning from mechanical ventilation. Eur Respir J 29:1033–1056
Tobin MJ, Jubran A (2006) Discontinuation of mechanical ventilation. In: Tobin MJ (ed) Principles and practice of mechanical ventilation, 2nd edn. McGraw-Hill, New York, pp 1185–1220
Vitacca M, Vianello A, Colombo D, Clini E, Porta R, Bianchi L, Arcaro G, Vitale G, Guffanti E, Lo CA, Ambrosino N (2001) Comparison of two methods for weaning patients with chronic obstructive pulmonary disease requiring mechanical ventilation for more than 15 days. Am J Respir Crit Care Med 164:225–230
Kollef MH, Shapiro SD, Silver P, St John RE, Prentice D, Sauer S, Ahrens TS, Shannon W, Baker-Clinkscale D (1997) A randomized, controlled trial of protocol-directed versus physician-directed weaning from mechanical ventilation. Crit Care Med 25:567–574
Burns KE, Lellouche F, Lessard MR (2008) Automating the weaning process with advanced closed-loop systems. Intensive Care Med 34:1757–1765
Esteban A, Frutos F, Tobin MJ, Alía I, Solsona JF, Valverdú I, Fernández R, de la Cal MA, Benito S, Tomás R, Carriedo D, Macías S, Blanco J (1995) A comparison of four methods of weaning patients from mechanical ventilation. Spanish Lung Failure Collaborative Group. N Engl J Med 332:345–360
Brochard L, Rauss A, Benito S, Conti G, Mancebo J, Rekik N, Gasparetto A, Lemaire F (1994) Comparison of three methods of gradual withdrawal from ventilatory support during weaning from mechanical ventilation. Am J Respir Crit Care Med 150:896–903
Esteban A, Alía I, Tobin MJ, Gil A, Gordo F, Vallverdú I, Blanch L, Bonet A, Vázquez A, de Pablo R, Torres A, de la Cal MA, Macías S (1999) Effect of spontaneous breathing trial duration on outcome of attempts to discontinue mechanical ventilation. Spanish Lung Failure Collaborative Group. Am J Respir Crit Care Med 159:512–518
Vallverdú I, Calaf N, Subirana M, Net A, Benito S, Mancebo J (1998) Clinical characteristics, respiratory functional parameters, and outcome of a two-hour T-piece trial in patients weaning from mechanical ventilation. Am J Respir Crit Care Med 158:1855–1862
MacIntyre NR, Epstein SK, Carson S, Scheinhorn D, Christopher K, Muldoon S (2005) Management of patients requiring prolonged mechanical ventilation: report of a NAMDRC consensus conference. Chest 128:3937–3954
Epstein SK, Ciubotaru RL (1998) Independent effects of etiology of failure and time of reintubation on outcome for patients failing extubation. Am J Respir Crit Care Med 158:489–493
Funk GC, Anders S, Breyer MK, Burghuber OC, Edelmann G, Heindl W, Hinterholzer G, Kohansal R, Schuster R, Schwarzmaier-D’Assie A, Valentin A, Hartl S (2010) Incidence and outcome of weaning from mechanical ventilation according to new categories. Eur Respir J 35:88–94
Ferrer M, Esquinas A, Arancibia F, Bauer TT, Gonzalez G, Carrillo A, Rodriguez-Roisin R, Torres A (2003) Noninvasive ventilation during persistent weaning failure. A randomized controlled trial. Am J Respir Crit Care Med 168:70–76
Ferrer M, Valencia M, Nicolas JM, Bernadich O, Badia JR, Torres A (2006) Early noninvasive ventilation averts extubation failure in patients at risk: a randomized trial. Am J Respir Crit Care Med 173:164–170
Ferrer M, Sellares J, Valencia M, Carrillo A, Gonzalez G, Badia JR, Nicolas JM, Torres A (2009) Non-invasive ventilation after extubation in hypercapnic patients with chronic respiratory disorders: randomised controlled trial. Lancet 374:1082–1088
Kollef MH, Ahrens TS, Shannon W (1999) Clinical predictors and outcomes for patients requiring tracheostomy in the intensive care unit. Crit Care Med 27:1714–1720
Esteban A, Frutos-Vivar F, Ferguson ND, Arabi Y, Apezteguía C, González M, Epstein SK, Hill NS, Nava S, Soares MA, D’Empaire G, Alía I, Anzueto A (2004) Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med 350:2452–2460
American Thoracic Society; Infectious Diseases Society of America (2005) Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 171:388–416
Knaus WA, Draper EA, Wagner DP, Zimmerman JE (1985) APACHE II: a severity of disease classification system. Crit Care Med 13:818–829
Epstein SK, Ciubotaru RL, Wong J (1997) Effect of failed extubation on the outcome of mechanical ventilation. Chest 112:186–192
Torres A, Gatell JM, Aznar E, El-Ebiary M, Puig de la Bellacasa J, González J, Ferrer M, Rodriguez-Roisin R (1995) Re-intubation increases the risk of nosocomial pneumonia in patients needing mechanical ventilation. Am J Respir Crit Care Med 152:137–141
Lemaire F, Teboul J, Cinotti L, Giotto G, Abrouk F, Steg G, Macquin-Mavier I, Zapol W (1988) Acute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation. Anesthesiology 69:171–179
Grasso S, Leone A, De Michele M, Anaclerio R, Cafarelli A, Ancona G, Stripoli T, Bruno F, Pugliese P, Dambrosio M, Dalfino L, Di Serio F, Fiore T (2007) Use of N-terminal pro-brain natriuretic peptide to detect acute cardiac dysfunction during weaning failure in difficult-to-wean patients with chronic obstructive pulmonary disease. Crit Care Med 35:96–105
Tobin MJ, Perez W, Guenther SM, Semmes BJ, Mador MJ, Allen SJ, Lodato RF, Dantzker DR (1986) The pattern of breathing during successful and unsuccessful trials of weaning from mechanical ventilation. Am Rev Respir Dis 134:1111–1118
Jubran A, Tobin MJ (1997) Pathophysiologic basis of acute respiratory distress in patients who fail a trial of weaning from mechanical ventilation. Am J Respir Crit Care Med 155:906–915
Jubran A, Mathru M, Dries D, Tobin MJ (1998) Continuous recordings of mixed venous oxygen saturation during weaning from mechanical ventilation and the ramifications thereof. Am J Respir Crit Care Med 158:1763–1769
MacIntyre NR (2005) Respiratory mechanics in the patient who is weaning from the ventilator. Respir Care 50:275–286
El Solh AA, Aquilina A, Pineda L, Dhanvantri V, Grant B, Bouquin P (2006) Noninvasive ventilation for prevention of post-extubation respiratory failure in obese patients. Eur Respir J 28:588–595
Nava S, Ambrosino N, Clini E, Prato M, Orlando G, Vitacca M, Brigada P, Fracchia C, Rubini F (1998) Noninvasive mechanical ventilation in the weaning of patients with respiration failure due to chronic obstructive pulmonary disease. A randomized, controlled trial. Ann Intern Med 128:721–728
Keenan SP, Powers C, McCormack DG, Block G (2002) Noninvasive positive-pressure ventilation for postextubation respiratory distress: a randomized controlled trial. JAMA 287:3238–3244
Acknowledgments
The authors wish to thank Roger Marshall for his editing aid. The authors also thank the respiratory therapy and nursing staff, and the attending physicians of the respiratory ICU, for their cooperation in this study. The authors also acknowledge the support of the Centro de Investigación Biomédica En Red-Enfermedades Respiratorias (CibeRes, CB06/06/0028)-Instituto de Salud Carlos III (ISCiii), Suport a Grups de Recerca (2009 SGR 911), a European Respiratory Society (ERS) Fellowship, and the Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS).
Conflicts of interest
None of the authors have a financial relationship with the organizations that sponsored the research.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is discussed in the editorial available at: doi:10.1007/s00134-011-2202-8.
Rights and permissions
About this article
Cite this article
Sellares, J., Ferrer, M., Cano, E. et al. Predictors of prolonged weaning and survival during ventilator weaning in a respiratory ICU. Intensive Care Med 37, 775–784 (2011). https://doi.org/10.1007/s00134-011-2179-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-011-2179-3