
Abstract
Objective
Infection is the most frequent cause of acute respiratory distress syndrome (ARDS). However, little is known about the influence of infection sites on ARDS. This study aimed to assess the associations of infection sites with ARDS development and mortality in critically ill infected patients.
Design
Prospective observational study.
Setting
Adult intensive care units (ICUs) of an academic medical center.
Patients
Study population included 1,973 consecutive patients admitted to ICUs with bacteremia, pneumonia or sepsis. During follow-up, 549 patients developed ARDS and 212 of them died within 60 days.
Main results
The distribution of infection sites in ARDS patients was: lung (77.2%), abdomen (19.3%), skin/soft tissues (6.0%), urinary tract (4.7%), unknown (2.6%), and multiple sites (17.7%). On multivariate analysis, lung was the only infection site associated with increased ARDS risk [adjusted odds ratio (OR) 3.49]. Urinary tract (adjusted OR 0.43), skin/soft tissue (adjusted OR 0.64), and unknown-site infections (adjusted OR 0.38) were associated with decreased risk. No association was found between individual infection site and ARDS mortality. However, unknown-site [adjusted hazard ratio (HR) 3.08] and multiple-site infections (adjusted HR 1.63) were associated with increased ARDS mortality. When grouping patients into pulmonary, nonpulmonary, and combined infections, nonpulmonary infection was associated with decreased ARDS risk (adjusted OR 0.28) and combined infections was associated with increased ARDS mortality (adjusted HR 1.69), compared with pulmonary infection.
Conclusions
In critically ill infected patients, pulmonary infection is associated with higher risk of ARDS development than are infections at other sites. Pulmonary versus nonpulmonary infection significantly affects ARDS development but not mortality.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Acute respiratory distress syndrome (ARDS) and its milder form acute lung injury (ALI) are common and devastating diseases occurring after certain pulmonary (direct) or nonpulmonary (indirect) insults [1]. Clinically, it is characterized by acute respiratory failure with bilateral pulmonary edema and severe hypoxemia. To date, ARDS remains an important burden in intensive care units (ICU), with mortality rate as high as 35–45% [2, 3].
Infection is the most frequent cause of human ARDS [4]. In animal studies of acute lung injury, infection-related models using lipopolysaccharide (19%) or live bacteremia (16%) are among the most commonly used models [5]. Many invading organisms can trigger host innate and acquired immune systems, and initiate the inflammatory cascade. Diffuse damage to the alveolar epithelium and capillary endothelium may occur in response to intense local (pulmonary) or systemic inflammation, leading to increased permeability and influx of protein-rich edema into the interstitial and air space. There are three major infection-related predisposing conditions for ARDS: pneumonia, sepsis, and bacteremia. Pneumonia is the major cause of direct lung injury, and sepsis is the major cause of indirect lung injury, while bacteremia, in the absence of pneumonia or sepsis, carries the lowest risk (<5%) [1, 6].
Although a prior study has shown that pulmonary versus nonpulmonary source of sepsis is not independently associated with mortality of ALI [7], less is known about its association with ARDS risk. The influences of specific infection sites on ARDS development and mortality are also unclear. This information could help clinicians to identify high-risk patients and may lead to more appropriate preventive or therapeutic interventions.
In this study, we describe the distribution of infection sites in a large population of critically ill infected patients, of whom 549 developed ARDS. We analyzed the associations of specific infection sites with the development and mortality of ARDS, using multivariate models. Since pulmonary (direct) and nonpulmonary (indirect) ARDS are different in pathophysiology [8], we also compared the associations of pulmonary and nonpulmonary infections with ARDS.
Patients and methods
Study design and study population
Study patients were recruited at Massachusetts General Hospital (Boston, MA, USA) from September 1999 to December 2008. Details of the study design have been described in our previous report [9]. Briefly, consecutive admissions to the ICUs were screened. Patients with predisposing conditions for ARDS including bacteremia, sepsis, pneumonia, trauma, aspiration, or multiple transfusions were eligible for inclusion. Exclusion criteria included age <18 years, diffuse alveolar hemorrhage, chronic lung diseases other than chronic obstructive pulmonary disease or asthma, directive to withhold intubation, immunosuppression, and treatment with granulocyte colony-stimulating factor (see Electronic Supplementary Material, ESM1, for details of the inclusion and exclusion criteria). Eligible patients were enrolled on ICU admission and followed daily for ARDS development, defined by the American–European Consensus Committee (AECC) criteria for ARDS [10], until death, ICU discharge, or 28 days after ICU admission. All ARDS patients were followed until death or 60 days after ARDS diagnosis. Patients with previous enrollment and patients admitted to ICUs without bacteremia, sepsis or pneumonia were excluded from analyses. The study was approved by the Human Subjects Committees of Massachusetts General Hospital and Harvard School of Public Health. Written informed consent was obtained from all subjects or surrogates.
Definitions and data collection
The definitions of bacteremia, sepsis, septic shock, pneumonia, trauma, multiple transfusions, and aspiration are shown in ESM1. Bacteremia, sepsis, and pneumonia were considered as the infection-related predisposing conditions, whereas trauma, multiple transfusions, and aspiration were considered as the non-infection-related predisposing conditions. The infections and infection sites in this study referred to those events leading to ICU admission and not infections acquired during ICU stay. Infection sites were determined based upon the clinical judgments of the treating physicians, imaging studies, and/or microbiologic tests collected within 48 h before or after ICU admission. These data were all recorded prospectively. Infections of upper and lower urinary tracts were grouped as urinary tract infection; infections of bone, joint, skin, soft tissue, and wound as skin/soft tissue infection; and infections of upper respiratory tract, line or device, endocarditis, meningitis, encephalitis, and others as other-site infection. Bacteremia with unknown source was considered as unknown infection site. When there were two or more infection sites identified, the patient was considered to have multiple infection sites.
Demographics and baseline clinical data were recorded on enrollment into the study. Vital signs and laboratory values in the first 24 h of ICU admission were collected, and Acute Physiology and Chronic Health Evaluation (APACHE) III scores were calculated accordingly. Data regarding treatments with vasopressors and activated protein C (APC), and ventilatory parameters were also collected. Body mass index (BMI, kg/m2) was calculated based on admission height and weight. Lung injury score was calculated based on chest X-ray, PaO2/FiO2 ratio, and positive end-expiratory pressure (PEEP) on ARDS day 1 [11]. To consider the possible effects of pre-ICU hospital stay on infection and ARDS, we created a variable indicating pre-ICU hospital stay ≥48 h or not. Patients transferred from other hospitals were considered to have pre-ICU hospital stay ≥48 h. We used development of ARDS as the primary outcome and all-cause 60-day mortality in ARDS as the secondary outcome.
Statistical analysis
All data were analyzed by using Statistical Analysis System (SAS) software package (version 9.1; SAS Institute, Cary, NC, USA). Categorical variables were compared by using chi-square test or Fisher’s exact test as appropriate. All continuous variables in this study were not normally distributed and thus were compared by nonparametric Wilcoxon rank-sum test. In multivariate models, we replaced missing values of BMI (12.1%) by overall median value. Other variables had missing values in <1%.
We used conditional logistic regression, stratified by calendar year, to analyze the associations of infection sites with ARDS development. Covariates in the multivariate models included age, gender, ethnicity, APACHE III score, ARDS risk factors (bacteremia, septic shock, and non-infection-related predisposing conditions), and clinical factors associated with ARDS development, with P < 0.20, in univariate analyses (BMI, diabetes, liver cirrhosis, history of alcohol abuse, and pre-ICU stay ≥48 h). For the final logistic regression model, we calculated the condition index (<21.7) and variance inflation factors (<1.5) to detect multicollinearity.
We used Cox proportional hazards regression, stratified by calendar year, to analyze the influence of infection sites on ARDS mortality. Covariates in the multivariate models included age, gender, ethnicity, APACHE III score, and clinical factors associated with ARDS mortality, with P < 0.20, in univariate analyses (BMI, bacteremia, liver cirrhosis, metastatic/hematological malignancies, pre-ICU stay ≥48 h, treatment with APC, PEEP level, and vasopressors used on ARDS day 1). For the final Cox regression model, we used Kolmogorov-type supremum tests to check the proportional hazards assumption (all P > 0.87). False discovery rate (FDR) adjustment was used to correct for multiple comparisons. The level of statistical significance was set at P ≤ 0.05 (two-sided).
Results
Patient enrollment and follow-up
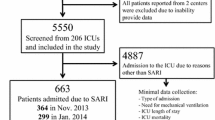
The enrollment and follow-up of study patients are illustrated in Fig. 1. During the study period, 3,668 patients were admitted to ICUs with required predisposing conditions for ARDS. Among those, 1,228 patients without consent were not enrolled. We excluded 97 patients previously enrolled and 370 patients without sepsis, pneumonia or bacteremia, leaving a total of 1,973 patients for analysis. Five hundred forty-nine (27.8%) patients developed ARDS, and 212 (38.6%) of them died in 60 days.

Enrollment and follow-up of study patients
Characteristics of study patients
Demographic and baseline characteristics of study population are shown in Table 1. Patients with ARDS were younger, and had higher APACHE III scores and BMI. Septic shock, pneumonia, and non-infection-related predisposing conditions were more commonly seen in ARDS patients than in non-ARDS patients. ARDS patients had a lower proportion of diabetes and a higher proportion of liver cirrhosis/failure than non-ARDS patients. History of alcohol abuse, and pre-ICU hospital stay ≥48 h were also more common in ARDS patients than in non-ARDS patients.
Clinical characteristics between ARDS survivors and nonsurvivors are shown in ESM2. Nonsurvivors were older, had higher APACHE III scores, lower BMI, and higher proportions of bacteremia and liver cirrhosis/failure, and were more likely to have pre-ICU hospital stay ≥48 h than survivors. More nonsurvivors had vasopressors used within 24 h after ARDS diagnosis, and more survivors received treatment with APC. There were no significant differences between survivors and nonsurvivors in lung injury score, pH value, PaO2/FiO2 ratio, PaCO2, PEEP, and tidal volume upon diagnosis of ARDS.
Associations of specific infection sites with ARDS development and mortality
The distributions of infection sites between ARDS and non-ARDS patients are shown in Table 2. In ARDS patients, lung was the most common infection site (77.2%), followed by abdomen (19.3%), skin/soft tissues (6.0%), and urinary tract (4.7%). Logistic regression analyses showed that lung was the only infection site significantly associated with increased risk of developing ARDS [adjusted odds ratio (OR) 3.49, 95% confidence interval (CI) 2.72–4.48]. Infections of urinary tract (adjusted OR 0.43, 95% CI 0.27–0.68), skin/soft tissue (adjusted OR 0.64, 95% CI 0.42–0.97), and other sites (adjusted OR 0.43, 95% CI 0.27–0.68) were all significantly associated with decreased risk. Abdominal infection was also associated with decreased risk of ARDS development (adjusted OR 0.78, 95% CI 0.59–1.02), but the association did not reach statistical significance (P = 0.071). Unknown infection site was significantly associated with decreased risk of developing ARDS (adjusted OR 0.38, 95% CI 0.20–0.70), whereas multiple infection sites was significantly associated with increased risk (adjusted OR 1.44, 95% CI 1.07–1.94).
The distributions of infection sites between ARDS survivors and nonsurvivors are shown in Table 3. Cox regression analyses revealed no specific infection site significantly associated with 60-day mortality in patients with ARDS. However, unknown-site infection [adjusted hazard ratio (HR) 3.08, 95% CI 1.37–6.90] and multiple-site infection (adjusted HR 1.63, 95% CI 1.13–2.35) were associated with increased mortality.
Associations of pulmonary versus nonpulmonary infection with ARDS development and mortality
Of the 1,973 study patients, 915 (46.4%) had pulmonary infection, 823 (41.7%) had nonpulmonary infection, and 235 (11.9%) had both pulmonary and nonpulmonary infections, with ARDS incidences of 36.4%, 15.2%, and 38.7%, respectively (Table 4). Multivariate analysis revealed that nonpulmonary infection was significantly associated with decreased risk of developing ARDS in patients admitted with infection (adjusted OR 0.28, 95% CI 0.22–0.37), compared with pulmonary infection.
Of the 549 ARDS patients, 333 (60.6%) had pulmonary infection, 125 (22.8%) had nonpulmonary infection, and 91 (16.6%) had both pulmonary and nonpulmonary infections, with 60-day mortality rates of 36.9%, 38.4%, and 45.1%, respectively (Table 5). Multivariate analysis revealed that combined pulmonary and nonpulmonary infections was significantly associated with increased risk of death in patients with infection-related ARDS (adjusted HR 1.69, 95% CI 1.14–2.49), compared with pulmonary infection.
Discussion
Although most ARDS cases are caused by infection, no study has comprehensively examined the influence of infection sites on ARDS. In this large prospective study, we were able to address the associations of infection sites with ARDS development and mortality in a population of nearly 2,000 critically ill infected patients. Our data showed that lung was the most common infection site in infection-related ARDS, and also the only infection site significantly associated with increased risk of developing ARDS. In contrast, nonpulmonary infection was associated with decreased ARDS risk. Although pulmonary versus nonpulmonary infection had a significant impact on ARDS development, it was not associated with ARDS mortality. However, ARDS patients with combined pulmonary and nonpulmonary sources of infections did have higher mortality. We also found that unknown-site infection was associated with decreased ARDS risk and increased ARDS mortality, while multiple-site infection was associated with both increased ARDS risk and mortality.
The distribution of infection sites in our entire study population was consistent with a previous report in critically ill infected patients [12]. However, there were significant differences in infection sites between ARDS and non-ARDS patients. ARDS patients had more pulmonary infections and less nonpulmonary infections than non-ARDS patients. We found that 77.2% of ARDS patients had pneumonia, with 21.5% of them also having nonpulmonary infection. The percentage of pneumonia in ALI/ARDS patients found in this study is higher than the percentages (around 50%) reported in other studies [3, 7, 13–18]. Indeed, these results may not be directly comparable because of different definitions of study population. We excluded patients with non-infection-related ARDS from analyses, which made the percentage of pneumonia higher in our study. Moreover, we used the criteria for ARDS, not the milder form ALI. Since ALI patients with pulmonary sepsis have higher lung injury scores than those with nonpulmonary sepsis [7], it is possible that the percentage of pneumonia is higher in patients with ARDS than in patients with ALI.
It is not surprising that pulmonary infection is associated with a higher risk of developing ARDS than nonpulmonary infection. The lung, with the largest epithelial surface area of the body, is repeatedly exposed to airborne particles and microorganisms. The highly integrated pulmonary defense system is capable of initiating rapid and intense immune responses to invading microbes, resulting in profound local and systemic inflammation [19, 20]. Pneumonia is the major cause of direct lung injury. Pneumonia is also the most common infection leading to sepsis, which is the major cause of indirect lung injury. The pathophysiology differs between direct and indirect lung injuries. The primary structure injured after a direct insult is the alveolar epithelium, while the first target of damage after an indirect insult is the pulmonary vascular endothelium [8]. When patients with pneumonia also develop sepsis, which was the case in 94% of our pneumonia patients, direct and indirect mechanisms may be triggered together, thus predisposing patients to a higher risk of developing ARDS.
Our result that pulmonary versus nonpulmonary infection was not associated with ARDS mortality confirmed the finding of a recent study [7]. Sevransky and colleagues analyzed 288 patients with sepsis-induced ALI and found lower severity of illness in ALI patients with pulmonary sepsis and no independent association between pulmonary source of sepsis and ALI mortality after multivariate analysis. Our study has advantages over the previous work. We had a larger sample size and thus greater statistical power to detect differences in hypothesized associations. In addition, 235 of our study patients had combined pulmonary and nonpulmonary infections. We categorized these patients into a third group, making the pulmonary and nonpulmonary groups more homogenous during comparison.
In patients with severe sepsis, multiple-site infection is associated with higher mortality [21, 22] and higher workload and cost [23]. Its influence on ARDS, however, remains unknown. Our study showed that multiple-site infection was associated with increased ARDS risk. Further analysis suggested that the association may be driven by pneumonia. Pneumonia was found in 86.4% of patients with multiple-site infection, but in only 53.8% of those with single-site infection (P < 0.001). This was further supported by the finding that combined pulmonary and nonpulmonary infection was not associated with increased ARDS risk when compared with pulmonary infection. We also found that multiple-site infection was associated with increased ARDS mortality, which was independent of pneumonia. Compared with pulmonary infection, combined pulmonary and nonpulmonary infection was also associated with increased ARDS mortality.
In this study, unknown-site infection was associated with decreased risk of ARDS development and increased risk of ARDS mortality. Our further analysis of patients with unknown infection site showed that 59/101 patients had bacteremia alone and the rest had sepsis of unknown etiology. Patients with bacteremia alone have been reported to have lower risk of ARDS compared with those with pneumonia and systemic infection [6]. Some patients with sepsis of unknown etiology, although fulfilling systemic inflammatory response syndrome (SIRS) criteria and having clinical suspicion of being infected, might not have had an infection and thus carried a lower risk of developing ARDS. Similar to our finding, an earlier study in ARDS patients also found worse mortality in bacteremic patients with unknown infection site [24]. Autopsy results of patients with unknown infection site showed that patients with bacteremia had infections requiring surgical drainage, and septic patients without bacteremia had pneumonia. Reasons are unclear, but unknown infection site has been shown to be independently associated with inappropriate empiric antibiotic treatment and fatal outcome [12, 25–28]. Given the relatively small sample size and the discrepancy between unadjusted and adjusted analyses in our study, the association between unknown-site infection and ARDS mortality needs to be confirmed in other studies.
This study has a major strength in that it was conducted within a large, well-defined, multiple-ICU population. We included ARDS cases and at-risk non-ARDS controls, and thus were able to assess the associations of infection sites with both ARDS risk and mortality. The large sample size provided adequate statistical power to evaluate the effects of individual nonpulmonary infections, unknown-site infection, and multiple-site infection on ARDS. In addition, these prospectively collected data were analyzed in multivariate models, adjusting for possible confounders. We also considered the advances in critical care over time, and performed all multivariate analyses with stratification by calendar year. Nevertheless, we acknowledge several limitations of our study. First, we did not collect data regarding antibiotic appropriateness, time to antibiotics, delay to recognize and treat severe sepsis, and time to meeting resuscitation goals, which might influence ARDS risk and outcomes in patients with sepsis [13]. Second, deaths in the early stages of critical illness may have occurred before ARDS could be recognized. However, analysis of our data indicated that this is a limited problem, as only 23 (1.2%) patients died within 72 h without having developed ARDS (see ESM3 for detailed discussion). Third, misclassification of infection sites is possible because of the complex nature and somewhat imprecise definitions of infections. Fourth, we did not take into account the specific role of individual pathogens in the development and mortality of ARDS, which remains unclear and needs further studies to elucidate [29]. Fifth, our study design limited the ability to assess causality of the associations found. Finally, this study was conducted in an ICU setting; any generalization to the general population should be made with caution.
Conclusions
This study demonstrates that lung is the most common infection site in patients with infection-related ARDS, and also the only infection site significantly associated with increased risk of developing ARDS in critically ill infected patients. In contrast, nonpulmonary infections are associated with decreased risk. Pulmonary versus nonpulmonary infection significantly affects ARDS risk but not mortality. Unknown-site and multiple-site infections are associated with increased ARDS mortality. These data provide important information relevant to the prevention and management of infected patients at risk for ARDS.
References
Ware LB, Matthay MA (2000) The acute respiratory distress syndrome. N Engl J Med 342:1334–1349
Phua J, Badia JR, Adhikari NK, Friedrich JO, Fowler RA, Singh JM, Scales DC, Stather DR, Li A, Jones A, Gattas DJ, Hallett D, Tomlinson G, Stewart TE, Ferguson ND (2009) Has mortality from acute respiratory distress syndrome decreased over time? A systematic review. Am J Respir Crit Care Med 179:220–227
Rubenfeld GD, Herridge MS (2007) Epidemiology and outcomes of acute lung injury. Chest 131:554–562
Matthay MA, Zimmerman GA, Esmon C, Bhattacharya J, Coller B, Doerschuk CM, Floros J, Gimbrone MA Jr, Hoffman E, Hubmayr RD, Leppert M, Matalon S, Munford R, Parsons P, Slutsky AS, Tracey KJ, Ward P, Gail DB, Harabin AL (2003) Future research directions in acute lung injury: summary of a National Heart, Lung, and Blood Institute working group. Am J Respir Crit Care Med 167:1027–1035
Matute-Bello G, Frevert CW, Martin TR (2008) Animal models of acute lung injury. Am J Physiol Lung Cell Mol Physiol 295:L379–L399
Niederman MS, Fein AM (1990) Sepsis syndrome, the adult respiratory distress syndrome, and nosocomial pneumonia. A common clinical sequence. Clin Chest Med 11:633–656
Sevransky JE, Martin GS, Mendez-Tellez P, Shanholtz C, Brower R, Pronovost PJ, Needham DM (2008) Pulmonary vs. nonpulmonary sepsis and mortality in acute lung injury. Chest 134:534–538
Pelosi P, D’Onofrio D, Chiumello D, Paolo S, Chiara G, Capelozzi VL, Barbas CS, Chiaranda M, Gattinoni L (2003) Pulmonary and extrapulmonary acute respiratory distress syndrome are different. Eur Respir J Suppl 42:48s–56s
Gong MN, Thompson BT, Williams P, Pothier L, Boyce PD, Christiani DC (2005) Clinical predictors of and mortality in acute respiratory distress syndrome: potential role of red cell transfusion. Crit Care Med 33:1191–1198
Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, Legall JR, Morris A, Spragg R (1994) The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 149:818–824
Murray JF, Matthay MA, Luce JM, Flick MR (1988) An expanded definition of the adult respiratory distress syndrome. Am Rev Respir Dis 138:720–723 (published erratum appears in Am Rev Respir Dis 1989 139:1065)
Alberti C, Brun-Buisson C, Goodman SV, Guidici D, Granton J, Moreno R, Smithies M, Thomas O, Artigas A, Le Gall JR (2003) Influence of systemic inflammatory response syndrome and sepsis on outcome of critically ill infected patients. Am J Respir Crit Care Med 168:77–84
Iscimen R, Cartin-Ceba R, Yilmaz M, Khan H, Hubmayr RD, Afessa B, Gajic O (2008) Risk factors for the development of acute lung injury in patients with septic shock: an observational cohort study. Crit Care Med 36:1518–1522
Brun-Buisson C, Minelli C, Bertolini G, Brazzi L, Pimentel J, Lewandowski K, Bion J, Romand JA, Villar J, Thorsteinsson A, Damas P, Armaganidis A, Lemaire F (2004) Epidemiology and outcome of acute lung injury in European intensive care units. Results from the ALIVE study. Intensive Care Med 30:51–61
Erickson SE, Martin GS, Davis JL, Matthay MA, Eisner MD (2009) Recent trends in acute lung injury mortality: 1996–2005. Crit Care Med 37:1574–1579
Wind J, Versteegt J, Twisk J, van der Werf TS, Bindels AJ, Spijkstra JJ, Girbes AR, Groeneveld AB (2007) Epidemiology of acute lung injury and acute respiratory distress syndrome in The Netherlands: a survey. Respir Med 101:2091–2098
Irish Critical Care Trials Group (2008) Acute lung injury and the acute respiratory distress syndrome in Ireland: a prospective audit of epidemiology and management. Crit Care 12:R30
Squara P, Dhainaut JF, Artigas A, Carlet J (1998) Hemodynamic profile in severe ARDS: results of the European Collaborative ARDS Study. Intensive Care Med 24:1018–1028
Delclaux C, Azoulay E (2003) Inflammatory response to infectious pulmonary injury. Eur Respir J Suppl 42:10s–14s
Zhang P, Summer WR, Bagby GJ, Nelson S (2000) Innate immunity and pulmonary host defense. Immunol Rev 173:39–51
Adrie C, Francais A, Alvarez-Gonzalez A, Mounier R, Azoulay E, Zahar JR, Clec’h C, Goldgran-Toledano D, Hammer L, Descorps-Declere A, Jamali S, Timsit JF (2009) Model for predicting short-term mortality of severe sepsis. Crit Care 13:R72
Brun-Buisson C, Doyon F, Carlet J, Dellamonica P, Gouin F, Lepoutre A, Mercier JC, Offenstadt G, Regnier B (1995) Incidence, risk factors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study in intensive care units. French ICU Group for Severe Sepsis. JAMA 274:968–974
Adrie C, Alberti C, Chaix-Couturier C, Azoulay E, De Lassence A, Cohen Y, Meshaka P, Cheval C, Thuong M, Troche G, Garrouste-Orgeas M, Timsit JF (2005) Epidemiology and economic evaluation of severe sepsis in France: age, severity, infection site, and place of acquisition (community, hospital, or intensive care unit) as determinants of workload and cost. J Crit Care 20:46–58
Bell RC, Coalson JJ, Smith JD, Johanson WG Jr (1983) Multiple organ system failure and infection in adult respiratory distress syndrome. Ann Intern Med 99:293–298
Leibovici L, Konisberger H, Pitlik SD, Samra Z, Drucker M (1992) Bacteremia and fungemia of unknown origin in adults. Clin Infect Dis 14:436–443
Valles J, Rello J, Ochagavia A, Garnacho J, Alcala MA (2003) Community-acquired bloodstream infection in critically ill adult patients: impact of shock and inappropriate antibiotic therapy on survival. Chest 123:1615–1624
Leibovici L, Shraga I, Drucker M, Konigsberger H, Samra Z, Pitlik SD (1998) The benefit of appropriate empirical antibiotic treatment in patients with bloodstream infection. J Intern Med 244:379–386
Leibovici L, Drucker M, Konigsberger H, Samra Z, Harrari S, Ashkenazi S, Pitlik SD (1997) Septic shock in bacteremic patients: risk factors, features and prognosis. Scand J Infect Dis 29:71–75
Bauer TT, Ewig S, Rodloff AC, Muller EE (2006) Acute respiratory distress syndrome and pneumonia: a comprehensive review of clinical data. Clin Infect Dis 43:748–756
Acknowledgments
This study was supported by grants ES00002, HL60710, and HL087934 from National Institutes of Health, USA. The authors would like to thank Thomas McCabe, Julia Shin, Hanae Fujii-Rios, Ian Taggart, and Kezia Ellison for patient recruitment; Andrea Shafer and Starr Sumpter for research support; Janna Frelich, Marcia Chertok, and Julie DelPrato for data management; and the patients and staff of ICUs at Massachusetts General Hospital.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Sheu, CC., Gong, M.N., Zhai, R. et al. The influence of infection sites on development and mortality of ARDS. Intensive Care Med 36, 963–970 (2010). https://doi.org/10.1007/s00134-010-1851-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-010-1851-3