
Abstract
Objective
Catheter colonization is commonly used as an end point in studies on central venous catheter (CVC) infections. This study aimed at comparing the rates of catheter colonization in patients according to the administration of antibiotics at removal.
Design
Prospective study over a 5-year period. All patients with a CVC removed without suspicion of CVC infection were included.
Setting
An adult medical/surgical intensive care unit at a university teaching hospital.
Patients
A total of 472 patients with CVC inserted for a mean CVC duration of 6.0 ± 3.7 days were included.
Methods
Antibiotics at removal was defined as antibiotics administered within 48 h before CVC removal, and CVC colonization as catheter tip culture yielding ≥ 103 colony-forming units per milliliter.
Interventions
None.
Measurements and results
Of 472 patients, 302 (64%) were receiving antibiotics at removal. The number of CVC colonizations per number of CVCs inserted was 4.7% (22 of 472) and the number of CVC colonizations per 1000 CVC days was 8.0. Administration of antibiotics at removal was associated with a lower risk of CVC colonization. Irrespective of CVC duration, CVC colonization rate differed between patients with or without antibiotics at removal (Kaplan–Meier test, p = 0.04).
Conclusions
The proportion of patients with antibiotics at time of removal should be taken into account when interpreting the results of surveys and trials using the quantitative CVC tip culture to define CVC colonization as an end point.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Numerous infection-control interventions have been developed to prevent CVC-related bloodstream infection; of these, CVC-related infection surveys and trials designed to measure the impact of hospital practice or new strategies are key elements in the development and evaluation of CVC-related infection policies.
Since CVC-related bloodstream infection is a rare event, most authors consider a quantitative CVC tip culture yielding ≥ 103 colony-forming units per milliliter as a suitable surrogate marker for CVC-related bacteremia [1, 2]; however, antibiotics administered at the time of microbiological sampling may inhibit the growth of bacteria potentially present in the samples. Whether antibiotics at CVC removal have a major impact on the results of CVC cultures is unknown. If they do, the findings of studies giving CVC culture results of patients irrespective of systemic antibiotic administration at the time of CVC removal are questionable.
The aim of the present work was to evaluate specifically the impact of antibiotics at CVC removal on the rate of CVC colonization.
Methods
Study population
This prospective study was performed in a nine-bed medical/surgical intensive care unit (ICU) at the university hospital of Clermont-Ferrand, France. From 1 September 2000 to 8 August 2005 all patients admitted to the ICU for more than 48 h and with a CVC in place during ICU stay were eligible. The patients were included in the study if they met the following criteria: CVC inserted and removed in the ICU; CVC duration ≥ 48 h, and CVC removed either because CVC was no longer needed or because of the death of the patient. To reduce the bias due to antibiotics administered for a suspected CVC infection on the results of CVC cultures, the patients with CVC removed while exhibiting local signs of CVC infection or suspicion of systemic CVC infection were not included. Only the first CVC inserted in the ICU was taken into account for inclusion in the study.
Data collection
For all eligible patients, demographics, the characteristics of catheterization, and the antibiotics within 48 h before insertion and before removal were collected.
Central venous catheterization
Polyurethane single- or multi-lumen CVCs with no antibiotic or antiseptic properties were inserted using strict sterile precautions according to a previously published standard protocol [3]. The CVCs were not tunneled and no guidewire assisted change of CVCs was used. In our unit, the CVCs were not changed after a fixed insertion time but removed when they were no longer needed, when the patient was suspected of systemic CVC infection, or because of death of the patient. The study and the consent policy were approved by the Ethics Committee of the hospital.
Microbiology
The CVCs were removed under aseptic conditions according to our standard protocol. The skin surrounding the insertion site was carefully disinfected with an alcoholic solution of 0.5% chlorhexidine before CVC removal. A 5-cm distal segment (tip) was collected in sterile containers for all catheters. All catheter tips were sent to the microbiology laboratory in a sterile tube for quantitative culture. The CVC tip was cultured as follows [4]: 1 ml of brain-heart broth was dripped on the tip and the tube was sonicated and vortexed; 0.1 ml of the suspension was then plated on blood agar. Standard microbiological methods were used to identify the colonizing organisms.
Definitions
Local CVC infection was defined by the presence of pus at the insertion site. The suspicion of systemic CVC infection was defined by one or more of the following criteria: temperature of < 36°C; temperature of ≥ 38.3°C with or without chill or sepsis or septic shock in a patient with no other obvious focus of infection. The CVC colonization was defined by a CVC tip culture yielding ≥ 103 colony-forming units per milliliter. The CVC-related bacteremia was defined as the isolation of the same phenotypic micro-organism from both peripheral blood culture and catheter-tip culture growing ≥ 103 cfu/ml when there was no other overt source of the bacteremia except the catheter. The comparability of microorganisms was based on speciation and antibiotic susceptibility profile. Antibiotics at removal refers to antibiotics administered within 48 h before CVC removal.
Statistical analysis
The aim of the study was not to assess the diagnostic accuracy of the quantitative CVC tip culture as a surrogate of CVC-related infection. The primary end point for the study was risk for CVC colonization according to antibiotics at removal. The CVC colonization rate was expressed using cumulative incidence (number of CVC colonizations per number of CVC inserted) and incidence density (number of CVC colonizations per 1000 CVC days). The variables associated with CVC colonization in univariate analysis were determined using chi-square test or Fischer's exact test when necessary for categorical variables and by Mann–Whitney test for continuous variables. Multivariate logistic regression analysis was performed, with colonization being the dependent variable and the variables found in the univariate analysis for CVC colonization with a p-value lower than 0.05 being the independent variables. The Kaplan–Meier test was used to compare the risk for CVC colonization according to catheter duration with regard to antibiotics at removal. Two-tailed p-values of less than 0.05 were considered to indicate statistical significance. Analyses were performed using SAS (SAS Institute, Cary, N.C.).
Results
The study included 472 patients, 279 men and 193 women (Table 1). The mean number of antibiotics administered at removal was 1.85 ± 0.98. Antibiotics were infused through the CVC in 245 of the 302 patients who were receiving them at removal. In 143 of 302 patients with antibiotics at removal, the antibiotics were administered throughout the catheterization period.
The cumulative incidence of CVC colonization was 4.7% (22 of 472) and the incidence density was 8.0 per 1000 days of CVC use. In univariate analysis, antibiotics at removal was the only variable associated with CVC colonization at a p-value < 0.05 (Table 2), and therefore no multivariate model was performed. Among the patients with antibiotics at removal there was no difference in the incidence rate of CVC colonization between those whose antibiotics at removal were administered throughout the catheterization period and the others (5 of 159 vs. 3 of 143, p = 0.72). Figure 1 shows an actuarial survival curve for CVC colonization. The Kaplan–Meier test demonstrated that the difference in the risk of CVC colonization with regard to antibiotics at removal was observed regardless of the catheter duration (p = 0.037). Similar results were observed in the subgroup of 356 patients who had their CVC removed because it was no longer needed (p = 0.033). During the study period, 170 eligible patients were not included because of CVC removal for a suspicion of CVC infection. When the data of these patients were combined with the data of the 472 included patients, similar results were observed. Antibiotics at removal was the independent risk factor associated with CVC colonization: OR = 0.49; 95% CI = 0.24 – 0.98 (p = 0.04; data not shown).

Proportion of central venous catheters (CVC) free of colonization
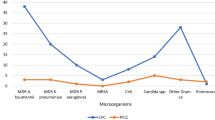
A total of 24 etiologic organisms were isolated in the 22 CVC colonizations. They were mainly Gram-positive cocci with a predominance of coagulase-negative staphylococci (Table 3). In patients on antibiotics at removal, the etiologic organisms of CVC colonization were resistant to the antibiotics in 5 of 8 cases.
In 1 patient with CVC removed because of death while exhibiting no sign of infection, both peripheral blood cultures and CVC tip culture yielded methicillin-resistant Staphylococcus aureus. Since there was only one CVC-related bacteremia, we cannot draw any meaningful conclusion concerning the impact of antibiotics at removal on CVC-related bacteremia.
Discussion
The CVC colonization is widely used as a primary end point in numerous studies on CVC infections [5–8]. The potential impact of antibiotics at removal on the rate of colonization of CVCs has not been fully assessed in clinical studies [9–15]. Our work is the first to specifically focus on this topic. Our results show that when CVCs are removed without suspicion of CVC infection, antibiotics at time of CVC removal interfere with the evaluation of CVC colonization, when CVC colonization is defined by a quantitative catheter-tip culture threshold > 103 ufc/ml. Our findings are not able to show whether antibiotics at removal have an impact on CVC colonization when CVC colonization is defined by the roll-tip culture. Our study cannot determine whether CVC culture yielding < 103 colony-forming units per milliliter corresponded to true-negative tests, i.e. the CVC were actually not colonized, or whether antibiotic use led to negative tests even in the presence of CVC colonization. Such a study would require another definition of CVC colonization that does not take into account the results of CVC cultures. The mechanisms by which antibiotics inhibit bacterial growth are speculative and the methods we used are unable to clarify this point.
To circumvent the bias due to the relationship between antibiotic administration for a suspicion of CVC infection and the subsequent results of CVC cultures, the patients with suspected CVC infection were excluded from the study. This renders questionable the translation of the results to this subpopulation; however, similar results were observed in the secondary analysis combining both patients with CVC removed with and without a suspicion of CVC infection suggesting that our results are extrapolated to all CVC removed when the quantitative culture is used to define CVC colonization.
We are aware that the present study has limitations. Firstly, the patients were not randomized to have antibiotics at removal, but conducting such an ideal study would not have been clinically feasible. Secondly, the inclusion in the study of the patients with CVC removal because of death could represent another potential bias in the interpretation of the results, since it would have been difficult to firmly rule out that CVC removal in this setting was unrelated to a suspicion of CVC infection; however, after excluding the CVCs removed because of death of the patients, we found similar results concerning the negative impact of antibiotics at removal on the occurrence of CVC colonization. Thirdly, we did not systematically record the indication for antibiotic treatment and the date of antibiotic introduction. Interestingly, among the patients receiving antibiotics at CVC removal, the frequency of CVC colonization was not different between the 145 whose antibiotics at removal had been administered throughout the catheterization period and the 159 whose antibiotics at removal had been introduced during catheterization. Fourthly, we took into account in the analysis only the antibiotics administered within 48 h before CVC removal. We cannot exclude that in some cases antibiotics previously administered but with a very long plasmatic half-life may have been present in the patient and therefore had an impact on the results of the quantitative CVC tip cultures.
Conclusion
In studies using the CVC quantitative culture tip to define CVC colonization, antibiotics at removal should be taken into account either when comparing the results of CVC colonization as benchmarks for quality management or as a surrogate of CVC infection for the evaluation of new preventive strategies in the field of CVC infection.
References
Rijnders BJ, Van Wijngaerden E, Peetermans WE (2002) Catheter-tip colonization as a surrogate end point in clinical studies on catheter-related bloodstream infection: How strong is the evidence? Clin Infect Dis 35:1053–1058
Safdar N, Fine JP, Maki DG (2005) Meta-analysis: methods for diagnosing intravascular device-related bloodstream infection. Ann Intern Med 142:451–466
Souweine B, Traore O, Aublet-Cuvelier B, Badrikian L, Bret L, Laveran H, Deteix P (1999) Dialysis and central venous catheter infections in critically ill patients: results of a prospective study. Crit Care Med 27:2394–2398
Brun-Buisson C, Abrouk F, Legrand P, Huet Y, Larabi S, Rapin M (1987) Diagnosis of central venous catheter-related sepsis. Critical level of quantitative tip cultures. Arch Intern Med 147:873–877
Raad I, Darouiche R, Dupuis J, Abi-Said D, Gabrielli A, Hachem R, Wall M, Harris R, Jones J, Buzaid A, Robertson C, Shenaq S, Curling P, Burke T, Ericsson C (1997) Central venous catheters coated with minocycline and rifampin for the prevention of catheter-related colonization and bloodstream infections. A randomized, double-blind trial. The Texas Medical Center Catheter Study Group. Ann Intern Med 127:267–274
Darouiche RO, Raad II, Heard SO, Thornby JI, Wenker OC, Gabrielli A, Berg J, Khardori N, Hanna H, Hachem R, Harris RL, Mayhall G (1999) A comparison of two antimicrobial-impregnated central venous catheters. Catheter Study Group. N Engl J Med 340:1–8
Veenstra DL, Saint S, Saha S, Lumley T, Sullivan SD (1999) Efficacy of antiseptic-impregnated central venous catheters in preventing catheter-related bloodstream infection: a meta-analysis. J Am Med Assoc 281:261–267
Maki DG, Stolz SM, Wheeler S, Mermel LA (1997) Prevention of central venous catheter-related bloodstream infection by use of an antiseptic-impregnated catheter. A randomized, controlled trial. Ann Intern Med 27:257–266
McGee DC, Gould MK (2003) Preventing complications of central venous catheterisation. N Engl J Med 348:1123–1133
Mermel LA (2000) Prevention of intravascular catheter-related infections. Ann Intern Med 132:391–402
Ranucci M, Isgro G, Giomarelli PP, Pavesi M, Luzzani A, Cattabriga I, Carli M, Giomi P, Compostella A, Digito A, Mangani V, Silvestri V, Mondelli E, Catheter Related Infection Trial (CRIT) Group (2003) Impact of oligon central venous catheters on catheter colonization and catheter-related bloodstream infection. Crit Care Med 31:52–59
Giles Y, Aksoy M, Tezelman S (2002) What really affects the incidence of central venous catheter-related infections for short-term catheterization? Acta Chir Belg 102:256–258
Brun-Buisson C, Doyon F, Sollet JP, Cochard JF, Cohen Y, Nitenberg G (2004) Prevention of intravascular catheter-related infection with newer chlorhexidine-silver sulfadiazine-coated catheters: a randomized controlled trial. Intensive Care Med 30:837–843
Moretti EW, Ofstead CL, Kristy RM, Wetzler HP (2005) Impact of central venous catheter type and methods on catheter-related colonization and bacteraemia. J Hosp Infect 61:139–145
Osma S, Kahveci SF, Kaya FN, Akalin H, Ozakin C, Yilmaz E, Kutlay O (2006) Efficacy of antiseptic-impregnated catheters on catheter colonization and catheter-related bloodstream infections in patients in an intensive care unit. J Hosp Infect 62:156–162
Acknowledgements
The authors thank J. Watts for his help in preparing the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Souweine, B., Heng, A.E., Aumeran, C. et al. Do antibiotics administered at the time of central venous catheter removal interfere with the evaluation of colonization?. Intensive Care Med 34, 286–291 (2008). https://doi.org/10.1007/s00134-007-0849-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-007-0849-y