
Abstract
Objective
To determine the relationship between measures of critical illness (sedative/analgesic administration, wakefulness and organ dysfunction), intensive care unit (ICU) recall and symptoms of posttraumatic stress disorder.
Design
Prospective, observational study with post-ICU follow-up.
Setting
Medical and surgical ICUs at a teaching hospital.
Patients
Two hundred seventy-seven subjects requiring > 36 h of mechanical ventilation were enrolled; 149 completed follow-up interviews 2 months later and 80 at 6 months.
Interventions
None.
Results
ICU recall was greater for events occurring at the end of critical illness; however, 18% of subjects had amnesia for the entire ICU course. Factual ICU recall was weakly associated with increased wakefulness during mechanical ventilation (r 2 = 0.03–0.11, p< 0.05). Posttraumatic stress disorder prevalence was 17% at 2 months and 15% at 6 months. The avoidance-numbing cluster had the highest specificity (91%) for a formal diagnosis and the re-experiencing cluster had the lowest (69%). Recall of a delirious memory during critical illness was associated with more severe posttraumatic stress symptoms, but there was no association between posttraumatic stress symptoms and factual recall of ICU events. Neither ICU recall nor posttraumatic stress symptoms were associated with the intensity of sedative administration during mechanical ventilation. Posttraumatic stress symptoms were lowest in patients either the most awake during mechanical ventilation or the least awake.
Conclusion
Wakefulness during mechanical ventilation has a greater influence on post-ICU recall and posttraumatic stress symptoms than sedative drug exposure or severity of illness. It is difficult to predict the future psychological consequences of an individual patient's critical illness.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Many patients surviving critical illness have decreased recall of factual events during mechanical ventilation yet report delusional memories. In 13 studies with 1882 patients, the frequency-weighted proportion of patients amnestic for the intensive care unit (ICU) was 29.6% (95% CI 27.5–31.7%) [1–13]. Memories of unreal situations were associated with worse post-ICU psychological adjustment than recall of factual memories [5]. In 10 studies comprising 1435 patients, the frequency-weighted proportion of patients with delirious memories was 26.7% (95% CI 24.4–29.1%) [3–5, 7–10, 12–14]. Few studies have identified factors that predict post-ICU amnesia or psychological symptoms such as posttraumatic stress symptoms [15–17].
Our study objectives were to (1) model the relationship between patient, medication or illness-related factors and post-ICU amnesia; (2) determine the relationship between ICU amnesia and posttraumatic stress symptoms; and (3) examine the domain structure of the posttraumatic stress disorder (PTSD) diagnosis for ICU patients. A version of this research was presented in an abstract [18].
Methods
We conducted a prospective study (approved by the Institutional Review Board for human subjects research) of adult patients mechanically ventilated for > 36 h in the medical and surgical intensive care units at the University of Minnesota Medical Center. Initial consent for enrollment was obtained by proxies (close family members in almost all cases) and a second consent to continue in the study was obtained from cognitively intact subjects before starting the follow-up interview. During the study period (2001–2003), the ICUs used sedation and analgesia guidelines including daily dose reduction for propofol [19]. However, there was not a protocol that recommended drug titration to a specific sedation level or mandated daily dose reduction for all sedatives. Nurses assessed patients' level of consciousness, spontaneous motor activity and overall sedation quality every 4 h using the Minnesota Sedation Assessment Tool (MSAT; see ESM) [20, 21].
Data were analyzed by 4-h time blocks during mechanical ventilation. Summed doses of midazolam, lorazepam, fentanyl, morphine, hydromorphone, and haloperidol dosages given during a 4-h time block were converted to mg/kg/4 h based on ICU admission weight. We considered 10 mg of intravenous morphine to be equivalent to 1.5 mg of hydromorphone and 0.1 mg of fentanyl [22]. Three milligrams of midazolam was equivalent to 1 mg of lorazepam [23]. Propofol and dexmedetomidine doses (μg/kg/min or μg/kg/h) were converted to μg/kg/4 h. There were 7750 4-h intervals for 149 subjects with follow-up data. Patients received at least one dose of a sedative medication in 6750 intervals (87%) and an arousal assessment was recorded during 5273 intervals (68%). 6/149 (4%) subjects received > 4 h of neuromuscular blockade during mechanical ventilation. Eleven other subjects received only a single dose for intubation or a procedure. Neuromuscular blockers prior to the ICU were not recorded.
We created and validated a sedation intensity score (SIS) to address the problem of aggregating sedative exposure across drug classes [21]. We first calculated the weight-adjusted dose of each medication administered during a time block. The dose was then categorized as 1–4 based on the quartile within the distribution of that drug for one time block in the sample (n = 277). For instance, if 0.1 mg/kg of lorazepam and 0.2 mg/kg of morphine were given during a 4-h interval and 0.1 mg/kg fell into the second quartile of the distribution of all 4-h lorazepam doses in the entire cohort and 0.2 mg/kg of morphine was in the third quartile, then the SIS for that time block was 2 + 3 = 5. A subject's mean SIS score (quotient of sum of subject's SIS values and number of 4-h intervals on mechanical ventilation) represents the average sedative exposure per hour relative to all other subjects.
Eighty-seven percent of the 2-month interviews were conducted in the home or facility where the subject was residing. All 6-month interviews were by telephone.
The study's “memory” tests focused on episodic or explicit memories which are subject to patients' ability to consciously recollect internal or external experiences. The initial 11 items of the questionnaire (item phrasing in Table 1) had a six-level Likert-type response format of “disagree very much” to “agree very much.” Questions 1–5 asked about events likely to occur in almost all patients (e.g., presence of endotracheal tube, suctioning, transfer out of ICU) so that a “disagree” response suggests amnesia for episodic memory. We summed responses from questions 1–5 to create the “ICU amnesia score”, a scale ranging from 5 (“disagree very much” on all items suggesting complete amnesia) to 30 (“agree very much” on all items suggesting complete recall).
Posttraumatic stress disorder (PTSD) symptoms and diagnoses were made with the Posttraumatic Stress Diagnostic Scale [24]. This scale closely follows the Diagnostic and Statistical Manual of Mental Disorders, version 4 [25] criteria for PTSD, which require ≥1 positive response in the five-item “re-experiencing” B domain; ≥3 positive responses in the seven-item “avoidance-emotional numbing” C domain; and ≥2 positive responses in the five-item “arousal” D domain. Domain-specific and global PTSD symptom severity scores were calculated by multiplying the number of positive symptoms by frequency severity (1 = once a week or less; 2 = two to four times per week; and 3 = five or more times per week) and summing within each domain (or over all three domains for a global score). Because a PTSD symptom severity score can be calculated for all subjects even if they do not have a PTSD diagnosis, to avoid misunderstanding, we renamed the global severity score the “PTSD-like severity score.”
Statistical methods
Group means were tested for differences by t-tests or ANOVA or nonparametric tests, depending on the distribution. If global F tests were significant (α< 0.05), post-hoc comparisons were tested with the Tukey HSD statistic.
Results
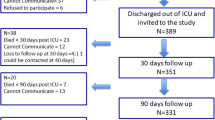
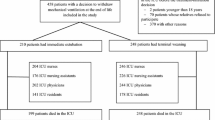
Figure 1 shows the enrollment and follow-up rates. Subjects had a broad range of indications for mechanical ventilation, with a median duration of mechanical ventilation of 6.8 days and a 32% 2-month case-fatality rate (Table 2). Compared to all enrollees (n = 277), those surviving and able to complete the PTSD assessment at 2-month follow-up (n = 149) were: (1) more likely to be treated in the SICU and have post-operative respiratory failure; (2) had shorter duration of mechanical ventilation; and (3) had better mental status prior to intubation.

Flow of subjects through the study
Recall of the ICU experience
The median ICU amnesia score was 14 (IQR 8, 20) and 18% of patients had a minimum score of 5, suggesting complete amnesia for the time in the ICU. The validity of the ICU amnesia score was supported by a moderate correlation (r = –0.69, p< 0.001) between the ICU amnesia score and a separate single ICU recall item (item 1 in Table 1). Also, in asking patients which part of their ICU time they recalled most clearly, the group choosing “can't recall anything” (n = 37) had significantly lower mean ICU amnesia scores than those choosing a specific period (n = 109) [7.5 (SD 3.7) vs. 16.8 (SD 6.2), p< 0.001].
The prevalence of individual ICU recall events or symptoms is shown in Table 1 and shows less recall of early ICU events than of later events. When asked to choose a time they recalled “most clearly”, only 4% chose “the beginning” and 71% chose “the end.” Similar findings in the opposite direction were found for the time recalled “least clearly”. About half the subjects reported memories of terror, hallucinations or unreal situations during their ICU stay.
Predictors of ICU amnesia
We found no relationship between the ICU amnesia score and three hypothesized predictors: SIS, duration of mechanical ventilation, or cumulative severity of illness by MODS. However, Fig. 2 shows a positive relationship between patient wakefulness during mechanical ventilation and the ICU amnesia score. This relationship was consistent across four separate analyses that had different thresholds for defining wakefulness. Although the correlation between the proportions of time spent at each level of wakefulness and the ICU amnesia score was statistically significant, the r 2-values were low (0.03–0.11), suggesting that other factors strongly affect ICU recall. For instance, subjects who were alert and awake prior to mechanical ventilation had a mean amnesia score of 15.3 (SD 6.9, n = 114); inattentive or confused, 12.1 (SD 6.7, n = 17); unresponsive or non-verbal, 12.5 (SD 7.0, n = 8) and unknown, 9.1 (SD 5.8, n = 8); global F = 3.1, p = 0.03.

Relationship between observed wakefulness during mechanical ventilation and ICU amnesia score. The ordinate is ICU amnesia score (5–30), with higher scores representing greater recall of factual ICU memories. The abscissa is quartiles of wakefulness, with quartile 4 representing cases with the greatest proportion of “awake” intervals during mechanical ventilation. Each plot uses a different Minnesota Sedation Assessment Tool Arousal threshold for defining the “awake” proportion: For each case we counted the number of 4-h time blocks which reached the threshold value divided by the total number of time blocks during mechanical ventilation. The mean ICU amnesia scores within each quartile group are compared with one-way ANOVA. A single asterisk indicates pair-wise comparisons are statistically different at a p-value of 0.01 to 0.05 and a double asterisk indicates a p-value of < 0.01. The upper-left plot defines “awake” as an arousal score of 3 or greater (global F = 8.2, p < 0.001. Pearson correlation before grouping by quartile was r = 0.34, p < 0.001). The upper-right plot raises the “awake” threshold to arousal score of 4 or greater (global F = 6.3, p < 0.001. Pearson correlation before grouping by quartile was r = 0.32, p < 0.001). The lower-left plot raises the arousal score to 5 or greater (global F = 1.7, p = 0.17. Pearson correlation, r = 0.18, p = 0.04). The lower-right plot defines “awake” as a score of 6 (global F = 3.8, p = 0.01. Pearson correlation, r = 0.25, p = 0.003). Horizontal bars are means, and ends of each vertical line are 95% confidence intervals
Diagnosis of posttraumatic stress disorder and specific symptom domains
Some 16.8% (25/149) of subjects at 2 months and 15% (12/80) at 6 months had a research diagnosis of PTSD (i.e., positive criteria for B, C and D domains). Women had more than twice the odds of having a PTSD diagnosis (OR 2.2, 95% CI 0.9–5.2), but this difference did not reach statistical significance.
More subjects met frequency criteria for individual symptom clusters than met diagnostic criteria for PTSD (see Table 3). The prevalence of subjects positive for the “re-experiencing” domain was greater than the other two domains, but the prevalence declined at 6 months, whereas symptoms in the “avoidance-numbing” and “arousal” domains were more persistent.
The “avoidance-numbing” cluster had the highest specificity (91.1%, 95% CI 86.1–96.6 %) for the PTSD diagnosis at 2 months. This means that 91% of all the subjects positive for the “C” domain met severity criteria for all three symptom domains. The “arousal” cluster had a lower specificity (78.2%, 95% CI 71.0–85.4%) and the “re-experiencing” cluster had the lowest specificity (68.6%, 95% CI 60.4–76.7%).
The 2-month PTSD-like severity score in the group with delirious memories was greater than subjects with no delirious memories [mean score 7.5 (SD 8.1) vs. 4.7 (SD 5.7), p = 0.018] but the proportion that had a formal PTSD diagnosis was not statistically different: 19.3% vs. 13.8%. We found no relationship between the extent of episodic memory (ICU amnesia score) and either the PTSD-like severity score or having recall of a delirious memory.
The presence of delirious memories was associated with higher (worse) scores in the “re-experiencing” [1.5 (SD 2.3) vs. 0.4 (SD 0.75), p = 0.001] and “avoidance-numbing” domains [3.3 (SD 3.9) vs. 2.1 (SD 3.2) p = 0.05] but not in the “arousal” domain [2.8 (SD 3.2) vs. 2.2 (SD 2.7), p = 0.23] than in subjects without a delirious memory. None of these relationships remained at 6 months.
Consequences of sedative exposure and wakefulness during mechanical ventilation
The sedation intensity score (sedative exposure averaged over the interval of mechanical ventilation) was not associated with three hypothesized post-ICU outcomes: PTSD diagnosis, PTSD domain scores or PTSD-like severity score. There was a linear positive relationship between SIS and having delirious memories: 42% of subjects in the lowest quartile of SIS (i.e., lowest sedative exposure) had a delirious memory compared to 66%, 58% and 71% in quartiles 2, 3 and 4, respectively (test for linear trend, p = 0.05).
The association between wakefulness during mechanical ventilation and post-ICU PTSD-like severity score was non-linear (Fig. 3). Increasing wakefulness was associated with increasing PTSD-like symptom scores until the highest quartile of wakefulness, in which the mean score fell to below that in the first quartile. The same pattern was also observed if the data were analyzed by individual domain scores (data not shown).

Relationship between observed wakefulness during mechanical ventilation and PTSD-like severity score. The ordinate is the PTSD-like severity score, with higher scores representing more frequent re-experiencing, avoidance and arousal symptoms. The abscissa is quartiles of wakefulness, with quartile 4 representing cases with the greatest proportion of “awake” intervals during mechanical ventilation. Each plot uses a different Minnesota Sedation Assessment Tool Arousal threshold for defining the “awake” proportion: For each case we counted the number of 4-h time blocks which reached the threshold value divided by the total number of time blocks during mechanical ventilation. The mean PTSD-like severity scores within each quartile group are compared with one-way ANOVA. A single asterisk indicates pair-wise comparisons are statistically different at a p-value of 0.01–0.05 and a double asterisk indicates a p-value of < 0.01. The upper-left plot defines “awake” as an MSAT assessment with an arousal score of 3 or greater (global F = 6.3, p < 0.001). The upper-right plot raises the “awake” threshold to arousal score of 4 or greater (global F = 2.3, p = 0.09). The lower-left plot raises the arousal score to 5 or greater (global F = 3.9, p = 0.01). The lower-right plot defines “awake” as a score of 6 (global F = 1.9, p = 0.13). Linear correlation analysis was not performed because of the appearance of non-linearity. Horizontal bars are means, and ends of each vertical line are 95% confidence intervals
Discussion
Our main findings on ICU recall were that: (1) greater wakefulness during mechanical ventilation was associated with increased factual recall for the ICU experience, although the relationship was not strong; (2) episodic recall was greater for events that occurred near the end of an episode of respiratory failure; (3) complete amnesia for the ICU experience occurred in 18%.
We propose three explanations for the lack of association between sedative exposure and recall. First, we used an aggregate measure of sedative exposure averaged over the course of mechanical ventilation. However, we have previously reported that sedation intensity increases soon after intubation, peaks around the mid-point of the intubation interval and then slowly declines [21]. Therefore, it is possible that peaks and troughs in sedation administration that could affect recall were averaged out over the course of critical illness. Second, patients with metabolic encephalopathy may have amnesia in the absence of sedatives. Third, sedatives and their metabolites may persist for many hours, and changes in serum levels of benzodiazepines may influence explicit memory more than level of consciousness [26]. Our data suggest that the behavioral state of the patient (e.g., overall objective level of consciousness) is more predictive of factual ICU recall than the amount of sedatives they received. However, the relationship is not strong, suggesting that ICU clinicians cannot reliably predict the amount and content of an individual patient's post-ICU recall.
Our main findings on post-ICU PTSD symptoms were as follows: (1) The prevalence of a formal PTSD diagnosis was similar at 2 and 6 months although the 15–17% rate does not represent the same individuals. (2) PTSD prevalence was higher and more likely to persist if PTSD was defined by a global score that disregarded whether symptoms were distributed across three PTSD domains. This suggests caution in interpreting prevalence studies of “medical” PTSD because results may be strongly influenced by case definition [27]. (3) Similar to community studies of PTSD, we found that women were more likely than men to develop PTSD [28].
The relationship between events during mechanical ventilation and PTSD was complex: Although the mean level of sedative exposure was associated with an increased risk of having a delirious memory; the intensity of sedative exposure, by itself, was not predictive of PTSD or PTSD-like symptom severity. Patients that were either the most awake or the most unresponsive during mechanical ventilation experienced the least amount of PTSD-like symptoms.
Results from this study are most readily comparable to eight prior studies [2, 5, 6, 8, 10, 14–16] although comparisons are limited by varied definitions of delirium, recall, PTSD and study design. Rotondi et al. [8] reported that amnestic subjects had greater day 1 APACHE III scores, whereas we did not find that severity of illness was associated with amnesia when we used a MODS score summed over the entire ICU stay. As in our study, Capuzzo et al. concluded that sedation did not affect recall of factual memories during ICU care [2]. We did not confirm Capuzzo's subsequent report that impairment in episodic memory was associated with delusional memories [14]. Kress et al. showed that patients treated with daily sedation interruption had lower Revised Impact of Events scores and PTSD prevalence than control patients even though the prevalence of ICU amnesia was equivalent (∼31%) [6]. The study by Samuelson et al. had a prevalence of complete amnesia (18%) comparable to our study and we confirmed their observation that greater patient wakefulness was associated with increased ICU recall [16]. Girard demonstrated that duration of delirium (prospectively measured during mechanical ventilation) was not associated with PTSD symptom severity at 6-month follow-up although the aggregate amount of lorazepam administered was weakly associated with subjects' PTSD symptoms [17].
Our results are in partial agreement with Jones et al. [5] in that patients with delirious memories had more PTSD-like symptoms, but we did not confirm that factual recall had a protective effect against developing PTSD. Patients examined by Schelling et al. (a median of 4 years after ICU care) [10] had a PTSD rate slightly higher than ours (28%), and those authors concluded that greater recall of “adverse experiences” during mechanical ventilation led to higher PTSD symptom scores years later [10]. Similar results were reported by Deja et al. [29].
Schelling and Jones' results lead to opposing theoretical approaches to sedation as an intervention to improve post-ICU psychological outcome. Schelling's findings suggest that higher doses of sedatives would more reliably create amnesia for “adverse experiences” and thereby decrease PTSD. Jones' data suggest that sedation can lead to delirious memories and blunt factual recall, which, albeit unpleasant, is protective against persistent PTSD-like symptoms. Our data support both interpretations: we found that having delirious memories was associated with more PTSD-like symptoms but patients that were the most awake during mechanical ventilation also had the lowest levels of PTSD-like symptoms. Whether the lower prevalence of PTSD symptoms is a direct consequence of alertness or indicates milder illness or brain dysfunction cannot be established with this study design. Similarly, it has never been proven that delirium, as measured by an objective instrument during ICU care, is associated with patients' post-ICU report of delirious memories. There are many valid reasons for administering sedatives to patients with respiratory failure, and adverse events may occur if patients are not sedated adequately [30].
An issue that has been under-appreciated in medical PTSD studies is that a formal diagnosis requires sufficient symptoms in three clusters. Breslau et al. showed in a community-based sample that symptoms in the “avoidance-numbing” cluster were more predictive of a “pervasive disturbance” than symptoms in the B and D domains [31]. Our results, derived from a completely different type of stressor, also show that the C cluster had the highest specificity for a formal PTSD diagnosis. While this may be partially explained by the higher number of symptoms needed to achieve a “positive” result for the C domain, our results also suggest that the oft-mentioned “ICU flashback” symptom is only a weak predictor of a “full-blown” PTSD diagnosis.
We acknowledge several study design limitations. Subjects were not randomly assigned to different sedative regimens or level of wakefulness, so a cause-and-effect relationship between ICU conditions and post-ICU outcomes cannot be established. We had limited data on subjects' pre-ICU psychiatric symptoms, did not measure delirium during mechanical ventilation and did not assess the extent to which patients were functionally impaired by PTSD symptoms. In contradistinction to studies of memory function in patients given a few hours of general anesthesia, we did not expose subjects to standardized stimuli and then test for conscious and non-conscious learning [32, 33]. The 6-month follow-up assessment had significant attrition and therefore our conclusions about symptom persistence are more subject to bias.
Conclusion
Post-ICU amnesia and PTSD symptoms are likely caused by a complex interaction of pre-existing psychological and cognitive function, gender, level of consciousness before and during critical illness, type of sedative drug exposure and severity and class of organ failure. Because many of these factors are not routinely measured in general practice, it is unlikely that a clinician can predict the recall content and psychological consequences of critical illness for a specific patient. Future research in PTSD associated with ICU care could benefit by evaluating the preventive and therapeutic interventions already tested in non-medical PTSD populations.
References
Bergbom-Engberg I, Haljamae H (1989) Assessment of patients' experience of discomforts during respirator therapy. Crit Care Med 17:1068–1072
Capuzzo M, Pinamonti A, Cingolani E, Grassi L, Bianconi M, Contu P, Gritti G, Alvisi R (2001) Analgesia, sedation, and memory of intensive care. J Critical Care 16:83–89
Granja C, Lopes A, Moriera S, Dias C, Costa-Pereira A, Carneiro A (2005) Patients' recollections of experiences in the intensive care unit may affect their quality of life. Critical Care 9:R96–R109
Hallenberg B, Bergbom-Engberg I, Haljamae H (1990) Patients' experiences of postoperative respirator treatment – influence of anaesthetic and pain treatment regimens. Acta Anaesthesiol Scand 34:557–562
Jones C, Griffiths R, Humphris G, Skirrow P (2001) Memory, delusions and the development of acute posttraumatic stress disorder-related symptoms after intensive care. Crit Care Med 29:573–580
Kress J, Gehlbach B, Lacy M, Pliskin N, Pohlman A, Hall J (2003) Long-term psychological effects of daily sedative interruption on critically ill patients. Am J Respir Crit Care Med 168:1457–1461
Magarey J (1997) Sedation of adult critically ill ventilated patients in intensive care units: a national survey. Australian Crit Care 10:90–93
Rotondi A, Chelluri L, Sirio C, Mendelsohn A, Schulz R, Belle S, Im K, Donahoe M, Pinsky M (2002) Patients' recollections of stressful experiences while receiving prolonged mechanical ventilation in an intensive care unit. Crit Care Med 30:746–752
Rundshagen I, Schnabel K, Wegner C, Schulte am Esch J (2002) Incidence of recall, nightmares, and hallucinations during analgosedation in intensive care. Int Care Med 28:38–43
Schelling G, Stoll C, Haller M, Briegel J, Manert W, Hummel T, Lenhart A, Heyduck M, Polasek J, Meier M, Preuss U, Bullinger M, Schuffel W, Peter K (1998) Health-related quality of life and posttraumatic stress disorder in survivors of the acute respiratory distress syndrome. Crit Care Med 26:651–659
Simpson TF, Armstrong S, Mitchell P (1989) American Association of Critical-Care Nurses Demonstration Project: Patients' recollection of critical care. Heart Lung 18:325–332
Green A (1996) An exploratory study of patients' memory recall of their stay in an adult intensive therapy unit. Intensive Crit Care Nursing 12:131–137
Kvale R, Ulvik A, Flaatten H (2003) Follow-up after intensive care: a single center study. Intensive Care Med 29:2149–2156
Capuzzo M, Valpondi V, Cingolani E, De Luca S, Gianstefani G, Grassi L, Alvisi R (2004) Application of the Italian version of the Intensive Care Unit Memory tool in the clinical setting. Critical Care 8:R48–55
Richter J, Waydhas C, Pajonk F (2006) Incidence of posttraumatic stress disorder after prolonged surgical intensive care unit treatment. Psychosomatics 47:223–230
Samuelson K, Lundberg D, Fridlund B (2006) Memory in relation to depth of sedation in adult mechanically ventilated intensive care patients. Intensive Care Med 32:660–667
Girard T, Shintani A, Jackson J, Gordon S, Pun B, Henderson M, Dittus R, Bernard G, Ely E (2007) Risk factors for posttraumatic stress disorder symptoms following critical illness requiring mechanical ventilation: a prospective cohort study. Critical Care 11:R28
Weinert C, Sprenkle M (2007) Post-ICU consequences of patient wakefulness and sedative exposure during mechanical ventilation. Am J Resp Crit Care Med 175:A21
Jacobi J, Fraser GL, Coursin DB, Riker RR, Fontaine D, Wittbrodt ET, Chalfin DB, Masica MF, Bjerke HS, Coplin WM, Crippen DW, Fuchs BD, Kelleher RM, Marik PE, Nasraway SA Jr, Murray MJ, Peruzzi WT, Lumb PD, Task Force of the American College of Critical Care Medicine (ACCM) of the Society of Critical Care Medicine (SCCM), American Society of Health-System Pharmacists (ASHP), American College of Chest Physicians (2002) Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med 30:119–141
Weinert C, McFarland L (2004) The state of intubated ICU patients: Development of a two-dimensional sedation rating scale for critically ill adults. Chest 126:1883–1890
Weinert C, Calvin A (2007) Epidemiology of sedation for mechanically ventilated patients. Crit Care Med 35:393–401
American Pain Society (1999) Principles of analgesic use in the treatment of acute pain and cancer pain, 4th edn. American Pain Society, Glenview, IL
Ely E, Truman B, Shintani A, Thomason J, Wheeler P, Gordon S, Francis J, Speroff T, Gautam S, Margoli (2003) Monitoring sedation status over time in ICU patients. JAMA 289:2983–2991
Foa E, Riggs D, Dancu C, Rothbaum B (1993) Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J Traumatic Stress 6:459–473
American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders: DSM-IV, 4th edn. American Psychiatric Press, Washington, DC
Verwey B, Muntendam A, Ensing K, Essink G, Pasker-de Jong P, Willekens F, Zitman F (2005) Clinically relevant anterograde amnesia and its relationship with blood levels of benzodiazepines in suicide attempters who took an overdose. Prog Neuropsychopharm Biol Psychiatry 29:47–53
Jackson J, Hart R, Gordon S, Hopkins R, Girard T, Ely E (2007) Post-traumatic stress disorder and post-traumatic stress symptoms following critical illness in medical ICU patients: assessing the magnitude of the problem. Critical Care 11:R27
Nemeroff C, Bremner J, Foa E, Mayberg H, North C, Stein M (2006) Posttraumatic stress disorder: a state-of-the-science review. J Psychiatr Res 40:1–21
Deja M, Denke C, Weber-Carstens S, Schroder J, Pille C, Hokema F, Falke K, Kaisers U (2006) Social support during intensive care unit stay might improve mental impairment and consequently health-related quality of life in survivors of severe acute respiratory distress syndrome. Critical Care 10:R147
Moons P, Sels K, De Becker W, De Geest S, Ferdinande P (2004) Development of a risk assessment tool for deliberate self-extubation in intensive care patients. Intensive Care Med 30:1348–1355
Breslau N, Reboussin B, Anthony J, Storr C (2005) The structure of posttraumatic stress disorder: latent class analysis in 2 community samples. Arch Gen Psychiatry 62:1434–1351
Hirshman E, Passannante A, Henzler A (1999) The effect of midazolam on implicit memory tests. Brain Cognition 41:351–364
Munte S, Kobbe I, Demertzis A, Lullwitz E, Munte T, Piepenbrock S, Leuwer M (1999) Increased reading speed for stories presented during general anesthesia. Anesthesiology 90:662–669
Author information
Authors and Affiliations
Corresponding author
Additional information
Work supported by a grant from the National Institutes of Health to C. R. W.
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Weinert, C.R., Sprenkle, M. Post-ICU consequences of patient wakefulness and sedative exposure during mechanical ventilation. Intensive Care Med 34, 82–90 (2008). https://doi.org/10.1007/s00134-007-0829-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-007-0829-2