
Abstract
Aims
To identify the variables affecting vancomycin pharmacokinetics in medical ICU patients and to evaluate the potential efficacy of dosage schedules by PK/PD analysis.
Design
A retrospective pharmacokinetic analysis of serum levels obtained in routine vancomycin monitoring was performed.
Setting
A 12-bed general ICU of a university teaching hospital.
Patients
Forty-six vancomycin-treated ICU patients fitting the following criteria: over 18 years old; more than three concentration data per patient; absence of renal replacement support, cardiac surgery and neoplastic disorders.
Interventions
Clinical information was collected from the patients' medical records. Details of vancomycin therapy, dosage and blood sampling times were obtained from pharmacokinetic reports. Population analysis were made by the standard two-stage approach.
Measurements and main results
Vancomycin clearance and distribution volume were estimated individually assuming a one-compartment pharmacokinetic model. PK/PD analysis was performed by Monte Carlo simulation. In the ICU patients, higher Vd (nearly twice the quoted value of 0.72 l/kg) and different vancomycin clearance–creatinine clearance relationship were found. Renal function, the APACHE score, age and serum albumin accounted for more than 65% of drug clearance variability. Vancomycin standard dosages led to a 33% risk of not achieving the recommended AUC24h/MIC breakpoint for Staphylococcus aureus.
Conclusions
The population kinetics and PK/PD analyses based on Monte Carlo simulation procedures offer an excellent tool for selecting the therapeutic option with the highest probability of clinical success in ICU patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Patients admitted to intensive care units (ICU) show high rates of infections, and dosage adjustment strategies have emerged as a critical factor in the control of infectious diseases within this clinical setting.
Staphylococcus aureus is the most common pathogen in the ICU, and according to surveillance studies all staphylococcal isolates remain susceptible to vancomycin [1, 2, 3]. Thus, this glycopeptide is still frequently used in ICU patients. Nevertheless, only limited data are available concerning the kinetic profiles and dosage requirements of this drug in this particular population group. Due to the pharmacokinetic modifications related to clinically ill status [4], higher doses seem to be necessary even when the pathogens have MIC values typical of susceptible microorganisms [5]. This clinical scenario is currently found in Spain, where glycopeptide-intermediate Staphylococcus aureus (GISA) strains are not yet documented.
The population approach aims at characterising the pharmacokinetic profile in a target patient group and includes interindividual and residual variability as well as the covariates affecting this. Subpopulations with special features can be identified, and relevant information aimed at tailoring dosage needs for each particular patient according to the clinical variables identified as the determinants of drug kinetics can be obtained. A previous study performed in ICU patients [6] revealed broad variability, together with a significant change in both clearance and the distribution volume during the course of vancomycin treatment; this highlighted the need for population modelling in this kind of patients. Nevertheless, such studies are scarce, except in patients receiving extracorporeal membrane oxygenation support [7] or renal replacement therapy [8].
The increasing development of antimicrobial resistance is one of the main causes of the failure of treatments in infectious diseases. In order to avoid or minimise this problem, particularly in ICUs, several strategies have been implemented, and in this sense, the application of pharmacokinetic/pharmacodynamic (PK/PD) criteria [9] is crucial for such a goal to be achieved. Such criteria allow clinicians to predict the potential efficacy of antimicrobial treatments based on patient characteristics and the aetiology of the infection, providing an excellent tool for choice of the best available therapy. In the case of glycopeptides, there is little information concerning this issue, although recently some interesting PK/PD information has been reported for vancomycin [10], supporting the idea that the ratio of the area under the serum concentration-time curve (AUC) and the minimum inhibitory concentration (MIC) is the parameter best correlated to efficacy in vancomycin therapy. Thus, the AUC/MIC ratio is currently accepted as the most relevant surrogate marker for this glycopeptide, and a value of 400 has been proposed as the recommended breakpoint for this parameter as referred to 24 h (AUC24h/MIC).
The dual aim of the present study was first to identify the variables that affect vancomycin profiles in a representative sample of medical ICU patients using sparse serum data collected during routine clinical care, and then to evaluate the dosage schedules to be applied in this group with respect to the probability of achieving the above-mentioned breakpoint for the AUC24h/MIC ratio.
Materials and methods
Study design
This retrospective, non-comparative pharmacokinetic study was conducted at a 662-bed teaching hospital belonging to the University of Salamanca (Spain) in collaboration with the pharmacy department of the same university.
Informed patient consent was unnecessary because the study involved collection of routine clinical data. However, approval was obtained from the institutional review board of the hospital.
Selection of patients
Initially, all vancomycin-treated patients admitted to the 12-bed general ICU of the above hospital from 1992 to 1998 were selected. The following exclusion criteria were then applied: patient under 18 years old; fewer than three vancomycin concentration-time data available; implementation of renal replacement therapy support, prior cardiac surgery, and the existence of neoplastic disorders.
Data collection
The patient information retrieved addressed clinical diagnosis at discharge; age; gender; height; total bodyweight; mechanical ventilation status; nutritional support; albumin and creatinine serum levels; creatinine clearance (CLcr); and concurrent administration of albumin, aminoglycosides, diuretics and catecholamines. Exitus and the Acute Physiology and Chronic Health Evaluation System (APACHE II) score were also collected from the patients' medical records. The APACHE II score was obtained within 24 h after ICU admission; the other variables were recorded at the start of vancomycin treatment as well as on the days of serum sampling to determine vancomycin level. Data pertaining to vancomycin therapy were obtained from pharmacokinetic reports that included the precise timing of drug dosing and blood sampling. For each patient, body surface area and body mass index were estimated according to standard formulas, and body weight on the day of vancomycin initiation was taken into account. Additionally, CLcr values estimated according to the Cockroft and Gault [11], Jelliffe [12] and Levey [13] formulas were recorded for each patient.
Serum sampling and analytical assay
In recent years, hospital guidelines for vancomycin sampling times have been modified. Thus, they have changed from obtaining peak data (3 h after post-infusion) together with trough samples (15–30 min prior to the next dose) to the current strategy that is mainly based on the latter (trough) levels, peak sampling being implemented only occasionally. A total of 233 vancomycin serum levels were recorded, mostly (80%) corresponding to trough values. Serum vancomycin concentrations were measured with a fluorescence polarisation immunoassay (AxSYM, Abbott Laboratories, Abbott Park, IL, USA) with a quantification limit of 2.00 μg/ml and an inter-day variation coefficient of < 7% for all standards. The external quality control used was Unity (Bio-Rad Laboratories).
Pharmacokinetic analysis
Pharmacokinetic analysis was performed assuming the one-compartment model [14], total vancomycin clearance (CL), and the apparent volume of distribution (Vd) being the estimated pharmacokinetic parameters. Population analysis was carried out with the standard two-stage approach. In the first stage, individual parameters were determined by non-linear regression using pharmacokinetic software (PKS, Abbottbase Pharmacokinetic System, version 1.10; Abbott Diagnosis Division, Irving, TX, USA). In the second stage, statistical analysis was applied to the parameters obtained in the first stage.
The area under the curve of vancomycin serum concentrations versus time from 0 to 24 h (AUC24h) was calculated as the daily dose/clearance ratio (D24h/CL). Note that the units of AUC and CL are mg/l*h and l/h/kg, respectively.
Monte Carlo simulations (evaluation of dosage schedules)
The probability of achieving the recommended value of the AUC24h/MIC ratio was estimated by the Monte Carlo simulation technique [15, 16, 17] from the AUC values calculated for each patient included in the study, as described above. Except for GISA strains [18], the MIC values reported for different pathogens by the EUCAST database (www.eucast.org) were used. A log-normal distribution was assumed for the AUC data according to statistical criteria. In the case of the MIC, a discrete distribution based on reported data was considered. Simulations for standard (2000 mg/day) as well as higher doses (up to 5000 mg/day) were performed in order to predict the interest of increasing the daily doses in this population group. Monte Carlo simulation was performed at 104 replicates using the SimulAr program [19].
Statistical analysis
For statistical analysis the SPSS software, version 12.0 (SPSS, Chicago, IL, USA), was used. The results are reported as means and medians, together with their dispersion coefficients. The correlation between pharmacokinetic parameters and continuous variables was established using the Pearson coefficient for normally distributed variables, and using the Spearman coefficient otherwise. Statistical significance was established at the p < 0.05 level.
Results
The main characteristics of the patient population selected (n = 46) are summarised in Table 1. The most prevalent clinical diagnosis was sepsis (n = 25). The origins of primary sepsis were as follows: abdominal (12), respiratory (7), peritonitis (3), catheter (2), abscess (2), endocarditis (1) and urinary (1). Septic shock was recorded in 16 of the patients with sepsis. The remaining patients had severe trauma (15) or a post-surgery status (6).
The mean (standard deviation) and median initial daily dose in these patients were 21.5 (8.3) mg/kg/day and 22.7 mg/kg/day, respectively, administered in intermittent i.v. infusion over 0.5–1 h. It should be noted that 50% of the patients initially received the conventional dosage regimen of 1,000 mg/12 h. Table 2 shows the pharmacokinetic parameters obtained for the overall population together with those corresponding to the different sub-population groups that emerged after excluding the patients who exhibited a given condition.
Since creatinine clearance is known to be the main covariate affecting vancomycin clearance, the influence of several different methods used to estimate this renal function index was tested. Table 3 shows the results of the regression analysis performed to establish the relationship between vancomycin clearance and creatinine clearance for both the estimated data and the individually measured values. Accordingly, the Levey formula is the one recommended to determine creatinine clearance.
The influence of the covariates on pharmacokinetic parameters of vancomycin was analysed with multiple regression techniques and the following equations were selected as the statistically significant predictors of drug clearance in our patient population:
Equation 1 (r 2 = 0.64; p < 0.01):
CL(ml/min/kg) = 0.660 – 0.016*age(years) – 0.006*ApII + 0.380*Ab + 0.562*CLcri (ml/min/kg)
Equation 2 (r 2 = 0.68; p < 0.01):
CL(ml/min/kg) = 0.872–0.015*age(years) – 0.007*ApII + 0.234*Ab + 0.346 CLcrLevey(ml/min/kg)
where ApII is APACHE II score, Ab is serum albumin (g/dl), Clcri is measured creatinine clearance and CLcrLevey is creatinine clearance as estimated by the Levey formula.
For comparative purposes, Table 4 shows reported values of vancomycin one-compartment parameters corresponding to non-critically ill patients [20, 21, 22, 23, 24, 25] versus the values obtained in the present study.
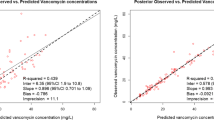
Table 5 and Figure 1 illustrate the results of the Monte Carlo simulations.

Influence of S. aureus vancomycin susceptibility and daily doses on the probability of attaining AUC24h/CMI values ≥ 400
Discussion
We found that renal function, APACHE II score, age and serum albumin accounted for more than 65% of the vancomycin clearance variability in ICU patients. This population also showed Vd nearly twice as high as the quoted value of 0.72 l/kg. According to PK/PD analysis vancomycin standard dosages led to a 33% risk of not achieving the recommended AUC24h/MIC breakpoint for S. aureus.
This study has integrated variability on both drug pharmacokinetics and pathogen susceptibility to evaluate vancomycin dosage in ICU patients. Adequate antibiotic therapy including optimal dosage has a significant impact on clinical outcome in patients with life-threatening infections such as those occurring in ICUs. Clinical failure and the emergence of resistance in this scenario have been related to inadequate dosage schedules. However, no useful guidelines for vancomycin dosage individualisation are available for ICU patients. The effect of patient pathophysiological status on drug disposition and the pronounced heterogeneity of critically ill populations should be taken into account with a view to improving the precision and appropriateness of dosage selection in this target population. The available data evaluating vancomycin pharmacokinetics in ICU patients are scarce, and studies aimed at applying the PK/PD approach to this specific population have not yet been attempted. The present study addresses the above issues and aims at finding clinically useful information that will allow the prediction and estimation of the correct dose for each particular ICU patient on vancomycin therapy.
In light of these clinical aims, a simple pharmacokinetic model that permits both the implementation of the two-stage approach and the use of limited serum data per patient was selected for our population analysis. A broad clinical diagnosis was also allowed so that the population would be typical of what may be encountered in this clinical setting. As reported for other antibiotics, interindividual variation in vancomycin pharmacokinetics is considerable in the case of ICU patients, and the increased Vd value generally ascribed to the sepsis-induced “third space” [26] is noticeable. Both observations could also be partly explained in terms of the methodology used in the present work, i.e. the two-stage and one-compartment model. Pharmacokinetic modifications in our ICU patients are evident, however, when comparing these findings with the values reported using similar approaches in “conventional” patients (Table 4). Any covariate, apart from body weight – which was used as normalisation factor – could explain the large interindividual differences observed in Vd, whereas CLcr, measured individually in the patients or estimated using Levey's formula, accounts for more than 50% of the variability in clearance. Moreover, the vancomycin clearance-CLcr relationship obtained in our ICU population differed from those used for dosage individualisation [27]. This confirms the need to design useful guidelines for vancomycin dosage individualisation in ICU patients such as those reported in the present work. In addition to its CLcr dependence, vancomycin clearance has been related to pathological (APACHE II) and clinical (age and albumin) characteristics, both explaining an additional 16% of variability in the parameter. Albumin influence on vancomycin clearance does not seem to have a plausible physiological basis. However, this may be due to albumin being a surrogate of illness severity or other non-recorded covariates. This would compromise the predictive ability of our model for other ICU populations. Confirmation of this hypothesis by prospective assays would be interesting.
Equations 1 and 2 permit not only the individual prediction and estimation of vancomycin clearance but also provide a simple method of dosage optimisation: the appropriate daily dose can be easily calculated as the product of the target AUC24h and the patient-predicted drug clearance. This predictive model remains valid throughout the treatment providing changes in included covariates are recorded and used in the corresponding equation, allowing dose adjustment according to patient evolution.
The Monte Carlo simulation techniques have recently been incorporated in the antimicrobial therapy field as a methodological strategy to take into account the pharmacokinetic and pharmacodynamic variability in PK/PD analysis. Their main interest lies in the possibility of using population pharmacokinetics to predict the potential efficacy of different dosage schedules in patients belonging to different population groups, when therapeutic drug monitoring is not possible, as long as the population model is available. The reliability of this approach, however, is directly related to the adequacy of the population model, and it will not perform better than, or replace, predictions from real data coming from measured serum concentrations.
In the present study this technique was applied for the first time to vancomycin. The results of Monte Carlo simulation revealed that doses of 3,000 mg or even 4,000 mg daily may be necessary to reach the highest probability of efficacy when susceptible S. aureus strains are involved in the infectious process. Similar results were found for other Staphylococcus isolates (Table 5). The advantages of the proposed procedure over the more popular so-called single-point analysis [28], which is based on use of the mean pharmacokinetic and pharmacodynamic parameters, lie in the possibility of estimating the level of uncertainty of predictions, since PK/PD variability is considered for risk analysis. Monte Carlo simulation provides information on what is probable, while single-point analysis merely shows what is possible. The differences between the two – probable and possible – become more relevant as the pharmacokinetic and pharmacodynamic variabilities increase, as occurs in ICU patients. For example, let us consider one of our prototype patients (59.5 years old, serum albumin level 2.3 g/dl, CLcr 65.5 ml/min, weight 71.5 kg and APACHE II score 18.9), for whom the estimated drug clearance according to Eq. 1 would be 0.984 ml/min/kg corresponding to 0.059 l/h/kg. A dose of 23.6 mg/kg/day would be estimated as the optimum to reach a target AUC24h/MIC of 400 if a MIC of 1 mg/l is assumed. Nevertheless, the Monte Carlo simulation affords a probability of clinical success of only 70% for such a dose, highlighting the relevance of PK/PD variability in risk analysis.
Regarding GISA strains, doses as high as 5,000 mg/day lead to a maximum probability of clinical outcome of only 80% for a value of 400 as the breakpoint (Fig. 1). From these findings, a vancomycin dosage of 2,000 mg/day should be questioned as a standard schedule in ICU patients, and the need for higher doses tailored according to population kinetics and pathogen susceptibility seems evident. The results also point to the suitability of considering antimicrobial agents other than vancomycin when GISA strains are involved, as suggested by other authors [29].
In summary, the application of our results to clinical practice would consist of the following:
-
1.
Use of Eq. 1 or Eq. 2 to estimate the patient's vancomycin clearance (ml/min/kg) followed by the unit conversion to l/h/kg.
-
2.
Estimation of daily dose from the product of the latter and the desired (target) AUC24h or AUC24h/MIC, if available.
-
3.
Use of Fig. 1 to obtain directly the recommended dose for any probability of attaining the AUC24h/MIC of ≥ 400 (for susceptible S. aureus and GISA) or to evaluate any dosing regimen used in this population group.
We believe that the model can be applied provided the patient and pathogen populations fit those considered in our study. If this is not the case, the same methodological procedure could be followed but the actual pharmacokinetics (relationship between drug clearance and patient variables) and pharmacodynamic modelling (MIC distribution) would have to be used. Note that neither infusion duration nor AUC24h/MIC breakpoint affects the usefulness of the model.
Despite the shortcomings of this study, due to its retrospective nature and the lack of patient outcome evaluation, our findings emphasise the risk of vancomycin underdosing in ICU patients, possibly leading to an unfavourable clinical outcome in therapy with this drug.
Other factors besides the (AUC)24h/MIC ratio have been reported as variables affecting the clinical outcome for ICU patients treated with vancomycin [29]. Nevertheless, optimisation of the above PK/PD index should be the goal when attempting to optimise vancomycin dosage schedules, since this shows the highest statistical correlation with response and, more importantly, it is the only circumstance that can be modified and consequently optimised by dosage adjustment. The patient's physiopathological condition and pathogen susceptibility cannot be avoided or modified but merely considered when antimicrobial treatment is initiated. Application of population kinetics together with PK/PD analysis based on Monte Carlo simulation, as performed in this study, offers an excellent tool to select the therapeutic option with the highest probability of clinical success not only in ICU patients but also in any other population. The reliability of this approach reinforces the interest of population pharmacokinetics as a tool for the optimisation of drug therapy. Prospective validation of the proposed model would be desirable.
References
Johnson AP, Henwood C, Mushtaq S, James D, Warner M, Livermore DM, The ICU Study Group (2003) Susceptibility of Gram-positive bacteria from ICU patients in UK hospitals to antimicrobial agents. J Hosp Infect 54:179–187 DOI 10.1016/S0195-6701(03)00145-2
Streit JM, Jones RN, Sader HS, Fritsche TR (2004) Assessment of pathogen occurrences and resistance profiles among infected patients in the intensive care unit: report from the SENTRY Antimicrobial Surveillance Program (North America, 2001). Int J Antimicrob Agents 24:111–118 DOI 10.1016/j.ijantimicag.2003.12.019
Jones ME, Draghi DC, Thornsberry C, Karlowsky JA, Sahm DF, Wenzel RP (2004) Emerging resistance among bacterial pathogens in the intensive care unit – a European and North American surveillance study (2000–2002). Ann Clin Microb Antimicrob 3:14 DOI 10.1186/1476-0711-3-14
Power BM, Forbes AM, van Heerden VP, Ilett KF (1998) Pharmacokinetics of drug used in critically ill adults. Clin Pharmacokinet 34:25–56
Pea F, Porreca L, Baraldo M, Furlanut M (2000) High vancomycin dosage regimens required by intensive care unit patients cotreated with drugs to improve haemodynamics following cardiac surgical procedures. J Antimicrob Chemother 45:329–335
Polard E, Le Bouquin V, Le Corre P, Kérebel C, Trout H, Feuillu A, Le Verge R, Mallédant Y (1999) Non steady state and steady state PKS Bayesian forecasting and vancomycin pharmacokinetics in ICU adult patients. Ther Drug Monit 21:395–403
Mulla H, Pooboni S (2005) Population pharmacokinetics of vancomycin in patients receiving extracorporeal membrane oxygenation. Br J Clin Pharmacol 60:265–275 DOI 10.1111/j.1365-2125.2005.02432.x
DelDot ME, Lipman J, Tett SE (2004) Vancomycin pharmacokinetics in critically ill patients receiving continuous venovenous haemodiafiltration. Br J Clin Pharmacol 58:259–268 DOI 10.1111/j1365-2125.2004.02143.x
Sánchez Navarro A, Sánchez Recio MM (1999) Basis of anti-infective therapy: pharmacokinetic–pharmacodynamic criteria and methodology for dual dosage individualisation. Clin Pharmacokinet 37:289–304
Moise-Broder PA, Forrest A, Birmingham C, Schentag JJ (2004) Pharmacodynamics of vancomycin and other antimicrobials in patients with Staphylococcus aureus lower respiratory tract infections. Clin Pharmacokinet 43:925–942
Cockroft DW, Gault MH (1976) Prediction of creatinine clearance from serum creatinine. Nephron 16:31–41
Jelliffe RW (1973) Creatinine clearance: beside estimate. Ann Inter Med 79:604–605
Levey AS, Bosch JP, Breger Lewis J, Greene T, Rogers N, Roth D (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med 130:461–470
Matzke GR (1992) Vancomycin. In: Evans WE, Schentag JJ, Jusko WJ (eds) Applied pharmacokinetics. Principles of therapeutic drug monitoring. Applied Therapeutics, Vancouver, pp 1–31
Bonate PL (2001) A brief introduction to Monte Carlo simulation. Clin Pharmacokinet 40:15–22
Mouton JW, Schmitt-Hoffman A, Shapiro S, Nashed N, Punt NC (2004) Use of Monte Carlo simulations to select therapeutic doses and provisional breakpoints of BAL9141. Antimicrob Agents Chemother 48:1713–1718
Sánchez Navarro A (2005) Optimización de la terapia antibacteriana mediante análisis farmacocinético/farmacodinámico: predicción de la eficacia con técnicas de simulación de Montecarlo. Rev Esp Quimioterap 18:230–235
Kantzanou K, Tassios PT, Tseleni-Kotsovili A, Legakis NJ, Vatopoulos AC (1999) Reduced susceptibility to vancomycin of nosocomial isolates of methicillin-resistant Staphylococcus aureus. J Antimicrob Chemother 43:729–731
Matzke GR, Mc Gory RW, Halstenson CE, Keane WF (1984) Pharmacokinetics of vancomycin in patients with various degrees of renal function. Antimicrob Agents Chemother 25:433–437
Rybak MJ, Boike SC (1986) Monitoring vancomycin therapy. DICP 20:757–761
Birt JK, Chandler MHH (1990) Using clinical data to determine vancomycin dosing parameters. Ther Drug Monit 12:206–209
Ducharme MP, Slaughter RL, Edwards DJ (1994) Vancomycin pharmacokinetics in a patient population: effect of age, gender and body weight. Ther Drug Monit 16:513–518
Kitzes-Cohen R, Farin D, Piva G, Ivry S, Scharony R, Amar R, Uretzky G (2000) Pharmacokinetics of vancomycin administered as prophylaxis before cardiac surgery. Ther Drug Monit 22:661–667
Rushing TA, Ambrose PJ (2001) Clinical application and evaluation of vancomycin dosing in adults. J Pharm Technol 17:33–38
De Paepe P, Belpaire FM, Buylaert A (2002) Pharmacokinetic and pharmacodynamic considerations when treating patiens with sepsis and septic shock. Clin Pharmacokinet 41:1135–1151
Zellner D, Zellner GE, Keller F (1998) Dependence of vancomycin clearance on renal function via regression and bootstrap methods. J Clin Pharm Ther 23:107–113
Ambrose PG, Quintiliani R (2000) Limitations of single point pharmacodynamic analysis. Pediatr Infect Dis J 19:769
Schentag JJ (2001) Antimicrobial management strategies for Gram-positive bacterial resistance in the intensive care unit. Crit Care Med 29(suppl 4):S100–S107
Acknowledgements
The authors thank the staff of the Intensive Care Medicine Department of the University Hospital of Salamanca for use of their facilities and collaboration.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Rights and permissions
About this article
Cite this article
del Mar Fernández de Gatta Garcia, M., Revilla, N., Calvo, M.V. et al. Pharmacokinetic/pharmacodynamic analysis of vancomycin in ICU patients. Intensive Care Med 33, 279–285 (2007). https://doi.org/10.1007/s00134-006-0470-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-006-0470-5