
Abstract
Objective
To evaluate the implementation and process of withholding and withdrawing life-sustaining treatment in an intensive care unit.
Design and setting
Prospective observational study in the medical intensive care unit of a university hospital in Lebanon.
Patients
Forty-five consecutive adult patients admitted to the ICU for a 1-year period and for whom a decision to withholding and withdrawal of life-sustaining treatment was made.
Measurements and results
Patients were followed up until their death. Data regarding all aspects of the implementation and the process of withholding and withdrawal of life-sustaining treatment were recorded by a senior staff nurse. Withholding and withdrawing life-sustaining treatment was applied to 9.6% of all admitted patients to ICU. Therapies were withheld in 38% and were withdrawn in 7% of patients who died. Futility of care and poor quality of life were the two most important factors supporting these decisions. The nursing staff was not involved in 26% of the decisions to limit care. Families were not implicated in 21% of the cases. Decisions were not notified in the patients’ medical record in 23% of the cases. Sixty-three percent of patients did not have a sedative or an analgesic to treat discomfort during end-of-life care.
Conclusions
Life-sustaining treatment were frequently withheld or withdrawn from adult patients in the Lebanese ICU. Cultural differences and the lack of guidelines and official statements could explain the ethical limitations of the decision-making process recorded in this study.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The withholding and withdrawal of life-sustaining treatment refer to the process by which medical interventions are not given or are removed from patients with the expectation that they will die as a result. Withholding and withdrawal of life-sustaining treatment decisions independently predict hospital death [1] and are the most common causes of death in intensive care units (ICU), accounting for 60–80% of ICU deaths [2, 3, 4]. These decisions are, for patient’s physicians and relatives, difficult to take [5] and depend on ethical issues related to social, cultural, moral, and religious values [6, 7]. The high prevalence of withholding and withdrawal of life-sustaining treatment, coupled with the associated ethical issues and emotional burden for the families, emphasizes the need to continuously evaluate the implementation and process of withholding and withdrawal of life-sustaining treatment in our medical practice [8]. A large number of clinical studies have been published, especially from North American [2, 3, 4, 9, 10, 11, 12, 13, 14] and European countries [15, 16, 17, 18, 19, 20] describing and assessing withholding and withdrawal of life-sustaining treatment practices. However, there are very few such studies from Middle Eastern Arabic countries where ethical values, medical resources, and financial limitations are different from those in Western countries [21, 22, 23].
We undertook a prospective observational study on withholding and withdrawal of life-sustaining treatment practices in the ICU of a teaching hospital in Lebanon. Our objectives were to assess the frequency of such practices, the therapies withheld or withdrawn, the reasons supporting these decisions, and how withholding and withdrawal of life-sustaining treatment processes were conducted.
Materials and methods
We conducted a prospective study over 12 months in the intensive care unit of Hotel-Dieu Hospital in Beirut, Lebanon. Hotel-Dieu Hospital is a 300-bed tertiary care facility with an eight-bed medical intensive care unit for adult patients. The triage process for admission to this ICU includes patients referred from in-hospital medical services for unstable neurological, respiratory, or cardiocirculatory vital functions. The admission process excludes patients for whom a decision to forgo life-sustaining therapy has already been taken by the primary physician. During the past 3 years patients were admitted in our ICU for respiratory diseases (30%), neurological diseases (30%), cardiocirculatory diseases (20%), and hepatic, renal and malignant diseases (20%). Hemodialysis was needed in 20% of patients and mechanical ventilation in 40%, with a mean duration of ventilation of 6 days and a mean ICU stay of 11 days. The nurse/patient ratio in this ICU is one nurse for two patients. The ICU is the setting for an internship and resident training program. The Hotel-Dieu Hospital institutional review board approved the study design, stipulating that no collected information would identify any individual patient.
We included in our study all consecutive patients admitted to the ICU between March 2003 and March 2004 and for whom a decision to withholding and withdrawal of life-sustaining treatment was made. Patients with brain death were excluded because withdrawal of therapy from patients who are brain dead is a legal and well accepted practice in Lebanon. All included patients were followed up until death. Data were collected prospectively by a senior member of the nursing staff who was not involved in the decision of withholding and withdrawal of life-sustaining treatment but who had knowledge of all steps of patient’s management and interactions with families and surrogate. The collection of data for the study did not interfere with the discussion, the implementation, or process of withholding and withdrawal of life-sustaining treatment.
Collected data from each patient included sex and gender, Acute Physiology and Chronic Health Evaluation score at admission, terminal illnesses and organ system failures at the time of withholding and withdrawal of life-sustaining treatment, and the type of decision, whether it was withdrawal life-sustaining treatment or withholding life-sustaining treatment. The reasons supporting the decision of withholding and withdrawal of life-sustaining treatment were noted using prespecified items: age, futility of care because of a terminal illness, poor quality of life, physical or psychological uncontrollable pain, financial cost, and family request. Life-sustaining treatment modalities withheld or withdrawn were noted as: mechanical ventilation, endotracheal intubation, dialysis, vasopressors and inotrops, surgery, antimicrobial therapy, transfusion of blood products, enteral or parenteral nutrition, and intravenous fluids. The time from admission to ICU to taking the decision of withholding and withdrawal of life-sustaining treatment and the time from the beginning of withholding and withdrawal of life-sustaining treatment to patient’s death were both noted. Individuals who made the decision to withholding and withdrawal of life-sustaining treatment were identified, whether a physician alone, the medical staff, or the medical and the nursing staff together. Information and involvement of patients and families in the decision-making process were noted. The presence of a written account of the withholding and withdrawal of life-sustaining treatment decision in the patient’s medical record was also noted. Finally, the administration of sedatives and analgesic agents during the process of withholding and withdrawal of life-sustaining treatment were recorded.
Each patient included in the study received a three-page data-collection form. Aggregated data were reported as numbers and percentages of patients for categorical variables and as median and ranges for continuous variables. Statistical analysis was not used in this descriptive study.
Results
Over the 1-year period of the study a total of 446 patients were admitted to our ICU, 51 of whom died despite ongoing active treatment and 43 as a result of withholding and withdrawal of life-sustaining treatment (9.6% of all admitted patients and 45.7% of all dead patients). Patients who died as a result of withholding and withdrawal of life-sustaining treatment had a median age of 65 years (range 16–90), a sex ratio of two men to three women, and a median Acute Physiology and Chronic Health Evaluation II score of 25 (range 6–45) at admission. Life-sustaining treatment was withheld in 37 patients (86%) and was withdrawn in 6 (14%). The reasons for admission to the ICU among these patients were respiratory failure (35%), circulatory failure (25%), coma (20%), and sepsis (20%). The median length of stay in the ICU of these patients was 8 days (range 1–40).
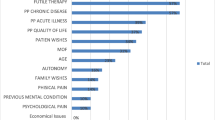
Terminal illnesses and organ system failures at the time of withholding and withdrawal of life-sustaining treatment are presented in Table 1, with multiple organ failure, sepsis, and cardiovascular failure being the most frequent. The reasons supporting the decision of withholding and withdrawal of life-sustaining treatment are presented in Table 2. Futility of care because of a terminal illness as well as poor quality of life were the two most important factors supporting the decision of withholding and withdrawal of life-sustaining treatment, while patient age, uncontrollable pain, financial cost, and family request were significantly less important factors.
Life-sustaining treatment modalities withheld or withdrawn are shown in Table 3. The most common modalities withheld or withdrawn were dialysis, vasopressors, and inotrops. Endotracheal intubation was withheld in two patients only (4.6%). The median time from admission to ICU to taking the decision of withholding and withdrawal of life-sustaining treatment was 5 days (range 1–30). The median time from the beginning of withholding and withdrawal of life-sustaining treatment to the time of patient’s death was 2 days (range 1–21). In two patients (4.6%) the withdrawal decision was later reconsidered by one of the closed family members, and medical treatment was resumed. After 1–2 days a new withdrawal of life-sustaining treatment was decided on in the two cases. Of the 43 patients whose medical life-sustaining treatment was withheld or withdrawn 40 (93%) died in the ICU and 3 (7%) died in the general ward after discharge from the ICU.
The decision to withhold and withdraw life-sustaining treatment was made by a single physician in 3 cases (7%), by medical staff without nursing staff in 8 (18.5%), and by medical and nursing staff in 32 (74.5%). Information and involvement of patients and families in the decision-making process are presented in Table 4. Only one patient (2.3%) was judged by his physicians to be competent to participate in treatment decisions. In nine cases (21%) the family was not involved, and the decision to withhold or withdraw life-sustaining treatment rested on the critical care medical staff and the primary physician. The hospital ethics committee was consulted about one case.
A written account of the withholding and withdrawal of life-sustaining treatment decision was present in the medical record of 33 patients (77%). This written account was always made by the attending critical care physician. Sedatives and analgesic agents were administered during the process of withholding or withdrawal of life-sustaining treatment to 16 patients only (37%). Reasons for restricting the use of sedatives and narcotic agents were given as absence of pain, decreased awakening, and severe hemodynamic or respiratory instability.
Discussion
This was the first prospective observational study assessing the implementation and the process of withholding and withdrawal of life-sustaining treatment in a Middle Eastern Arabic country. Lebanon is an Arab country where Muslim and Christian beliefs as well as oriental and occidental trends of life coexist, and where relations among family members are close, and social traditions are rather conservative. Clinical studies on practices with regard to withholding and withdrawal of life-sustaining treatment in Middle Eastern countries have been reported from Israel [24] and Turkey [25]. However, these two countries have different social lives, traditions, languages, and religious beliefs than Arabic societies. One study from Saudi Arabia focused only on the accuracy of decision to withdraw therapy in critically ill patients and did not evaluate other aspects of the decision [22]. Another study from Lebanon assessed the attitudes of Lebanese judges regarding end of life issues but did not evaluate clinical practices regarding withholding and withdrawal of life-sustaining treatment [21]. A prospective study from Oman was performed in a neonatal ICU and did not evaluate withholding and withdrawal of life-sustaining treatment in adults [23].
In our study 9% of admitted patients and 45% of dead patients in ICU had a decision of withholding and withdrawal of life-sustaining treatment. Similar figures have been reported from Israel and Latin countries in Europe [17, 19, 24]. However, the incidence of withholding and withdrawal of life-sustaining treatment reported in northern European and North American literature is much higher and reaches 70–90% in patients who die in the ICU [2, 4, 9, 10, 16]. The relatively low incidence of withholding and withdrawal of life-sustaining treatment decisions in Lebanon could be related to the absence of consensus statements and guidelines from scientific societies and to the lack of information on attitudes toward end-of life-sustaining treatment in the Lebanese media. Another important finding of our study is that withdrawing life-sustaining treatment is given to only 7% of patients who die in the ICU. Eidelman et al. [24] reported that withholding life-sustaining treatment is common in an Israeli ICU whereas withdrawal of therapies is limited to brain-dead patients. Iyilikçi et al. [25] reported that Turkish physicians prefer limiting treatment rather than discontinuing therapy in critically ill patients. Physicians from the Middle East seem to consider that withholding and withdrawal of life-sustaining treatment are not ethically equivalent and are reluctant to withdraw therapies in critically ill patients. This attitude differs from that reported in most European and North American studies, in which decisions to withhold treatment are not distinguished from withdrawal decisions [3, 9, 10, 16, 17, 18]. This difference regarding withholding and withdrawing therapies in different countries may be related to religious beliefs and moral convictions.
The reasons for the withdrawal and withholding decisions in our study did not differ from those reported in most other studies [2, 3, 9, 16, 17, 20]. Futility of care and poor quality of life were the most common reasons given in more than 90% of withholding and withdrawing life-sustaining treatment decisions, whereas advanced age, uncontrollable pain, economic cost, and family request were given in only 14% of decisions. This finding suggests that a balance between the aggressiveness of ICU care and poor medical prognosis or poor quality of life is an ethical concept well accepted by Lebanese physicians. On the other hand, advanced age and financial cost were not found to be important factors in deciding withholding and withdrawal of life-sustaining tratment, even though Lebanese health-care system is economically very limited. Uncontrollable pain was infrequently considered as a reason for withholding and withdrawal of life-sustaining treatment in our study. Similarly, Wood and Martin [3] considered suffering to be minimally to moderately important to the interviewed intensivists.
We observed several ethical limitations in the withholding and withdrawal of life-sustaining treatment processes in our ICU. First, more than 50% of the decisions were taken 5–30 days after admission to ICU and only 2 days before death. Similar figures have been reported in several other studies [9, 20, 25, 26], raising the question of whether the shift to palliative strategies takes place inappropriately late in the course of illness. In Lebanon the delay in taking a withholding or withdrawal of life-sustaining treatment decision is frequently related to families who insist on giving full medical support to the patients and require several meeting with the medical team before reaching a consensus. Second, a substantial portion (26%) of decisions to limit care are taken without involving the nursing staff. Nurses have a close relationship with critically ill patients and many studies [17, 20, 27] recommended their participation in ethical discussions and decisions. Third, 23% of decisions were not noted in the patient medical record. This may reflect the reluctance of some physicians to record their decisions because of the Lebanese legal context. Lebanon does not currently have clearcut legal guidelines related to end-of-life care. There are no legal precedents to define whether a physician has the authority to withhold or to withdraw life-sustaining treatment in critically ill patients. Similarly, Vincent [18] found in his European study that because of legal concerns physicians in Italy, Spain, and Greece are willing to give verbal orders to restrict care but not to write these orders down. A fourth worrying finding in this study is that 63% of patients do not have a sedative or an analgesic to treat discomfort during the process of withholding and withdrawal of life-sustaining treatment. Lebanese physicians seem reluctant to use sedatives and analgesics after limitation of therapies because of the risk of precipitating death and of so-called active euthanasia. The SUPPORT [28] study showed that 50% of seriously ill patients are in moderate to severe discomfort and pain during the last 3 days of life. This raises the possibility that unskilled cessation of life-sustaining treatment may lead to unnecessary suffering in the final hours of life. Even more, no evidence has been found that the use of narcotics or benzodiazepines hastens death after the withdrawal of life-sustaining treatment in critically ill patients [11, 13]. The implementation of standardized procedures in Lebanese ICU may help physicians to increase medication delivery and to improve the quality of dying.
An ethical process entails information and consent of patients, families, or both. In our study only one patient was judged competent to be consulted, and relatives were not included in the withholding or withdrawal of life-sustaining treatment decision in 21% of cases. The grounds for deciding to avoid involving family members are difficulty in establishing a trustful relationship and in reaching a rational consensus between numerous surrogates. There are in Lebanon no guidelines governing the relationship between physician, patient, and family. This relationship is often limited to a traditional paternalism based on the principle of benevolence. Similarly, studies from Mediterranean and European countries report that a high portion of decisions to limit therapy are not discussed with families. A study by Ferrand et al. [17] in France found that families were informed in only 59% of the cases. In a study in Swedish ICUs one-half the decisions of withholding and withdrawal life-sustaining treatment were made without a documented discussion with the patient or the family [16]. Sonnenblick et al. [29] reported that in an Israeli hospital families were involved in only 29% of the decision-making cases for terminally ill patients. Conversely, in most reports from North America families are more systematically informed of the withholding or withdrawing decisions [2, 9, 26]. In a review article on withholding and withdrawal of life-sustaining treatment Way et al. [30] found that close collaboration with patients’ families is mandatory and may shorten the dying process.
Our method to evaluate withholding and withdrawal of life-sustaining treatment in Lebanon had some limitations that may have influenced the interpretation of our results. First, it was a prospective observational study, and the attitude of physicians in ICU may have been biased by their knowledge that they were observed. However, it was our impression, from our daily practice, that the results of this study reflected the attitude of the intensivists in our hospital. Second, it was a single-center study that lasted only 12 months, with a limited number of charts to analyze. This pilot study will be followed by a prospective multicenter study including several Lebanese intensive care units. Data collected from this study will reflect more accurately the practice of all Lebanese intensivists regarding withholding and withdrawal of life-sustaining treatment. Previous studies demonstrated high variability in end-of-life care between various groups of physicians in the same country [10, 12, 26]. Third, we did not collect data about the patients who died in ICU despite ongoing active treatment. Several studies have compared demographic characteristics, medical history, therapeutic modalities, ICU stay, and surrogates attitudes between patients dying after withholding and withdrawal of life-sustaining treatment and patients dying despite ongoing life-sustaining treatment [3, 9, 17, 19]. Such a study could have helped us to better understand practice patterns of withholding and withdrawal of life-sustaining treatment in Lebanon. Fourth, this study did not investigate all aspects of withholding and withdrawal of life-sustaining treatment practices in our critically ill patients. Further studies should focus on specific issues such as the impact of oriental social values and religious Muslim or Christian beliefs on the involvement of family members and on refusal of withdrawal life-sustaining treatment.
In conclusion, life-sustaining treatment therapies were found to be withheld or withdrawn frequently from critically ill adult patients in a Lebanese ICU. Some of the characteristics and the processes of withholding and withdrawal of life-sustaining treatment do not fully correspond to current European and North American guidelines. The Fifth International Consensus Conference on Critical Care in 2003 recommended a shared approach involving the caregiver team and the patient families to guarantee respect for patient autonomy, a pain free death, and the prohibition of treatments specifically designed to hasten death [31]. Cultural differences and the lack of guidelines and official statements from Lebanese legal and scientific bodies could explain the ethical limitations of the decision-making process recorded in this study. Larger studies focused on physicians’ attitudes and on the perception of patients and families regarding end of life care are necessary in Lebanon and in other countries of the Middle East. Such studies will help to clarify withholding and withdrawal of life-sustaining treatment practices and to elaborate legal and scientific guidelines in this region of the world. Recent international recommendations can be taken as a baseline reference and adapted to our local cultural context.
References
Azoulay E, Pochard F, Garrouste-Orgeas M, Moreau D, Montesino L, Adrie C, De Lassence A, Cohen Y, Timsit JF, on the behalf of the outcomerea group (2003) Decisions to forgo life-sustaining therapy in ICU patients independently predict hospital death. Intensive Care Med 29:1895–1901
Prendergast TJ, Luce JM (1997) Increasing incidence of withholding and withdrawal of life sustaining treatment from the critically ill. Am J Respir Crit Care Med 155:15–20
Wood GG, Martin E (1995) Withholding and withdrawing life-sustaining therapy in a Canadian intensive care unit. Can J Anaesth 42:186–191
Faber-Langendoen K, Bartels DM (1992) Process of forgoing life-sustaining treatment in a university hospital: an empirical study. Crit Care Med 20:570–577
Pochard F, Azoulay E, Chevret S, Lemaire F, Hubert P, Canoui P, Grassin M, Zittoun R, Le Gall JR, Dhainaut JF, Schlemmer B, for the French FAMIREA group (2001) Symptoms of anxiety and depression in family members of intensive care unit patients: ethical hypothesis regarding decision-making capacity. Crit Care Med 29:1893–1897
Vincent JL (2001) Cultural differences in end-of-life care. Crit Care Med 29 [Suppl]:N52–N55
Bone RC, Rackow EC, Weg JG (1990) Ethical and moral guidelines for the initiation, continuation, and withdrawal of intensive care. Chest 97:949–957
Levy MM (2001) Evaluating our end-of-life practice. Crit Care 5:182–183
Keenan SP, Busche KD, Chen LM, McCarthy L, Inman KJ, Sibbald WJ (1997) A retrospective review of a large cohort of patients undergoing the process of withholding or withdrawal of life sustaining. Crit Care Med 25:1324–1331
Prendergast TJ, Claessens MT, Luce JM (1998) A national survey of end-of-life care for critically iII patients. Am J Respir Crit Care Med 158:1163–1167
Treece PD, Engelberg RA, Crowley L, Chan JD, Rubenfeld GD, Steinberg KP, Curtis JR (2004) Evaluation of a standardized order form for the withdrawal of life sustaining treatment in the intensive care unit. Crit Care Med 32:1141–1148
McLean RF, Tarshis J, Mazer D, Szalai JP (2000) Death in two Canadian intensive care units: institutional difference and changes over time. Crit Care Med 28:100–103
Chan JD, Treece PD, Engelberg RA, Crowley L, Rubenfeld GD, Steinberg KP, Curtis JR (2004) Narcotic and benzodiazepine use after withdrawal of life sustaining. Association with time to death? Chest 126:286–293
Hall RI, Rocker GM, Murray D (2004) Simple changes can improve conduct of end-of-life care in the intensive care unit. Can J Anaesth 51:631–636
Giannini A, Pessina A, Tacchi EM (2003) End-of-life decisions in intensive care units: attitudes of physicians in an Italian urban setting. Intensive Care Med 29:1902–1910
Nolin T, Andersson R (2003) Withdrawal of medical treatment in the ICU. A cohort study of 318 cases during 1994–2000. Acta Anaesthesiol Scand 47:501–507
Ferrand E, Robert R, Ingrand P, Lemaire F, for the French LATAREA group (2001) Withholding and withdrawal of life sustaining treatment in intensive-care units in France: a prospective survey. Lancet 357:9–14
Vincent JL (1999) Forgoing life sustaining treatment in western European intensive care units: the results of an ethical questionnaire. Crit Care Med 27:1626–1633
Esteban A, Gordo F, Solsona JF, Alia I, Caballero J, Bouza C, Alcala-Zamora J, Cook DJ, Sanchez JM, Abizanda R, Miro G, Fernandez Del Cabo MJ, De Miguel E, Santos JA, Balerdi B (2001) Withdrawing and withholding life sustaining treatment in the intensive care unit: a Spanish prospective multi-centre observational study. Intensive Care Med 27:1744–1749
Turner JS, Michell WL, Morgan CJ, Benatar SR (1996) Limitation of life sustaining: frequency and practice in a London and a Cape Town intensive care unit. Intensive Care Med 22:1020–1025
Adib SM, Kawas SH, Hajjar TA (2003) End-of-life issues as perceived by Lebanese judges. Developing World Bioethics 3:10–26
Chang RW, Lee B, Jacobs S, Lee B (1989) Accuracy of decisions to withdraw therapy in critically ill patients: clinical judgment versus a computer model. Crit Care Med 17:1091–1997
Costa DE, Ghazal H, Al Khusaiby S (2002) Do not resuscitate orders and ethical decisions in a neonatal intensive care unit in a Muslim community. Arch Dis Child Fetal Neonatal Ed 86:F115–F119
Eidelman LA, Jakobson DJ, Pizov R, Geber D, Leibovitz L, Sprung CL (1998) Foregoing life-sustaining treatment in an Israeli ICU. Intensive Care Med 24:162–166
Iyilikçi L, Erbayraktar S, Gökmen N, Ellidokuz H, Kara HC, Günerli A (2004) Practices of anaesthesiologists with regard to withholding and withdrawal of life sustaining treatment from the critically ill in Turkey. Acta Anaesthesiol Scand 48:457–462
Maksoud L, Jahnigen DW, Skibinski CI (1993) Not resuscitate orders and the cost of Death. Arch Intern Med 153:1249–1253
Lofmark R, Nilstun T (1997) Deciding not to resuscitate. Responsibilities of physicians and nurses: a proposal. Scand J Caring Sci 11:207–211
Support Principal Investigators (1995) A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (Support). JAMA 274:1591–1598
Sonnenblick M, Gratch L, Raveh D, Steinberg A, Yinnon AM (2003) Epidemiology of decision on life-sustaining treatment in the general internal medicine division. Harefuah 142:650–653
Way J, Back AL, Curtis JR (2002) Withdrawing life sustaining treatment and resolution of conflict with families. BMJ 325:1342–1345
Carlet J, Thijs LG, Antonelli M, Cassell J, Cox P, Hill N, Hinds C, Pimentel JM, Reinhart K, Thompson BT (2004) Challenges in end-of-life care in the ICU. Statement of the 5th International Consensus Conference in Critical Care: Brussels, Belgium, April 2003. Intensive Care Med 30:770–84
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yazigi, A., Riachi, M. & Dabbar, G. Withholding and withdrawal of life-sustaining treatment in a Lebanese intensive care unit: a prospective observational study. Intensive Care Med 31, 562–567 (2005). https://doi.org/10.1007/s00134-005-2578-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-005-2578-4