
Abstract
Objective
To review how biotrauma leads to the development of multiple system organ failure (MSOF).
Design and setting
Published articles on experimental and clinical studies and review articles in the English language were collected and analyzed.
Results
The concept that ventilation strategies using “large” tidal volumes and zero PEEP of injured lungs can enhance injury by the release of inflammatory mediators into the lungs and circulation, a mechanism that has been called biotrauma, is supported by evidence from experimental models ranging from mechanically stressed cell systems, to isolated lungs, intact animals, and humans. Biotrauma may lead to MSOF via spillover of lung-borne inflammatory mediators into the systemic circulation. However, spillover of other agents such as bacteria and soluble proapoptotic factors may also contribute to the onset of MSOF. Other less well studied mechanisms such as peripheral immunosuppression and translocation of bacteria and/or products from the gut may play an important role. Finally, genetic variability is a crucial factor.
Conclusions
The development of MSOF is a multifactorial process. Our proposed mechanisms linking mechanical ventilation and MSOF suggest several novel therapeutic approaches. However, it will first be necessary to study the mechanisms described above to delineate more precisely the contribution of each proposed factor, their interrelationships, and their time course. We suggest that scientific advances in immunology may offer novel approaches for prevention of MSOF secondary to ventilator-induced lung injury.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Mechanical ventilation has been of enormous value in improving the survival of many patients. However, the use of this technique also has adverse effects since the ventilation procedure itself can cause direct damage to the lungs [1, 2, 3]. Initial experimental research on the induction and course of ventilator-induced lung injury (VILI) focused primarily on the contribution of mechanical factors such as pressure and volume [4, 5, 6, 7, 8, 9, 10]. Based on these studies innovative and protective lung strategies have been proposed to avoid VILI by limiting tidal volume and/or plateau pressure and by maintaining recruitment of alveolar regions with sufficient positive end-expiratory pressure (PEEP). Clinical trials subsequently made clear that ventilator management can alter mortality in patients with the acute respiratory distress syndrome (ARDS) [11, 12]. Despite these improvements a large number of ARDS patients still die of multiple system organ failure (MSOF).
Recent research has focused on how mechanical stresses caused by mechanical ventilation can affect cellular and molecular processes in the lung, a mechanism that has been called biotrauma [13]. It has become clear that mechanical ventilation triggers an inflammatory reaction in the lung and that the degree of inflammation depends on the mode of ventilation [14, 15, 16, 17] and ventilation strategy [18]. Furthermore, it has been suggested that this inflammatory reaction may not be limited to the lungs but may also initiate and propagate a systemic inflammatory response, possible contributing to the onset of MSOF [19, 20].
We review biotrauma and focus particularly on the way in which biotrauma can lead to the development of MSOF. Since we propose that the development of MSOF secondary to mechanical ventilation is not the result solely of biotrauma but is likely a multifactorial process, several other mechanisms are discussed as well.
Mechanical ventilation and MSOF
Biotrauma
The biotrauma hypothesis of VILI is relatively new and is the subject of some scientific debate [21, 22, 23]. Two independent pathways of the biotrauma hypothesis can be distinguished: (a) ventilation may cause release of mediators, and (b) these mediators have biological action [22]. Most research has focused on the first part of this hypothesis. It has become clear that ventilation strategies using “large” tidal volumes and zero PEEP of already injured lungs can promote the release of inflammatory mediators in the lungs. This is supported by evidence from experimental models ranging from mechanically stressed cell systems [24] to isolated lungs [18], intact animals [25, 26, 27, 28], and humans [12, 29], although detection of inflammatory mediators, in particular tumor necrosis factor (TNF) α concentrations is not universal [21, 30, 31]. Also, the injurious ventilation of healthy lungs (one-hit model) demonstrated early lung gene expression or release of various mediators [18, 32, 33]. Whether biotrauma holds true for normal, healthy lungs subjected to noninjurious or injurious ventilation in vivo is less clear [34, 35]. In contrast to the first part of the biotrauma hypothesis, the second pathway of the biotrauma hypothesis has only recently begun to be addressed and will certainly be a topic for future research.
It is important to realize that various mechanisms are responsible for the ventilation-induced release of mediators. There are four principal mechanisms, all of which appear to be clinically relevant: (a) stress failure of the plasma membrane (necrosis), (b) stress failure of endothelial and epithelial barriers (decompartmentalization), (c) overdistension without tissue destruction (mechanotransduction), and (d) effects on vasculature, independently of stretch and rupture [36]. These mechanisms should be taken into account in the interpretation of studies on molecular mechanisms of VILI [37, 38, 39]. The notion that mediator levels can increase in response to ventilation-induced cell necrosis and decompartmentalization [40, 41] does not exclude that under less injurious ventilation strategies [35], stretching of the lung can activate specific mechanotransduction pathways [22, 38]. For example, we have noted in 12 infants without prior lung injury that TNF-α and interleukin (IL) 6 concentrations in bronchoalveolar lavage were increased after 2 h of mechanical ventilation with a tidal volume of 10 ml/kg and a PEEP of 4 cmH2O, and this was associated with the absence of clinically obvious harmful effects of mechanical ventilation [35].
The possible pivotal role for biotrauma in the development of MSOF was based on the suggestion that this inflammatory reaction is not limited to the lungs but via spillover of mediators in the circulation may also initiate and propagate a systemic inflammatory response [19, 20]. Indirect evidence from experimental models ranging from an isolated perfused and ventilated mouse lung [42], intact animals with preinjured lungs [25, 26], and humans with acute lung injury or ARDS [12, 29, 43] supports this hypothesis. Whether injurious ventilation of healthy lungs is also associated with increased serum concentrations of inflammatory mediators is less clear [34, 44].
Direct demonstration of this phenomenon is difficult in vivo since lung-derived inflammatory mediators cannot easily be biolabeled to facilitate the detection of the cellular sources of cytokine release and cytokine trafficking. There is some evidence that pulmonary cytokines do in fact spill over; using an ex vivo single pass perfusion model, Uhlig and colleagues [45] demonstrated release of cytokines from the lung. Also, in a model of decompartmentalization increased pulmonary and systemic concentrations of TNF-α were measured [40, 41]. It is important to realize that these increased concentrations are due to both tissue destruction and mechanotransduction [36]. In addition, concentration differences across the lung (difference between arterial and mixed venous) for inflammatory mediators have been detected in patients with ARDS [46].
Although there is evidence that lung-borne inflammatory mediators spill over into the circulation, there is no confirmed relationship with the development of MSOF [47, 48, 49]. However, results of the ARDS Network study showed that day 3 plasma IL-6 concentrations were significantly lower in ARDS patients ventilated with a tidal volume of 6 ml/kg (predicted body weight) than those ventilated with a tidal volume of 12 ml/kg [12]. This may reflect a reduced systemic inflammatory response secondary to the lung protective strategy, which could have contributed to the increased organ failure free days and the lower mortality in the group treated with lower tidal volumes [12]. In addition, a post-hoc analysis of the relationship between organ failures and cytokine concentrations revealed that an increase in IL-6 plasma concentrations is correlated with the development of MSOF [50]. It remains unclear how pro- and anti-inflammatory mediators exert their detrimental effect on distal organs. Also, the biological action of these mediators is unclear, especially when both pro- and anti-inflammatory mediators are released into the circulation [43, 49].
With respect to biological activity it is important to realize that not only inflammatory mediators but also extracellular HSP-70 (eHSP-70) may be translocated from the lung into the circulation. Ventilation increases the expression of intracellular HSP-70, which also implies that HSP-70 is secreted rapidly during and after the ventilation procedure [28, 51]. The presence of eHSP-70 in the plasma may activate innate immune responses, with production of inflammatory mediators. eHSP-70 is a ligand for the lipopolysaccharide (LPS) receptor or the Toll-like receptor (TLR) 4 on monocytes and macrophages, thereby eliciting a host of inflammatory mediators [52, 53].
In summary, we believe that biotrauma plays an important role in the development of MSOF secondary to mechanical ventilation. There are still important issues, in particular with respect to the biological activity of these mediators, that need to be addressed. In addition, development of MSOF secondary to mechanical ventilation is likely not due solely to biotrauma but likely is a multifactorial process. We therefore discuss several other mechanisms that may be involved, a number of which are hypothetical.
Translocation of bacteria or products from the lung
Similar to the spillover of inflammatory mediators into the circulation, overinflation during mechanical ventilation may also promote the translocation of bacteria or their products from the lung into the bloodstream, thereby contributing to the development of MSOF [19, 20]. In a dog model Nahum et al. [54] demonstrated that a ventilatory strategy that markedly overdistended the lungs while allowing repetitive opening and closure of alveoli facilitated translocation to the bloodstream of bacteria that had previously been instilled intratracheally. Similar results were obtained in rats [55]. Using a rat model in which Klebsiella pneumoniae were instilled into the lungs Verbrugge et al. [55] demonstrated that mechanical ventilation with a high peak inspiratory pressure (30 cmH2O) and zero PEEP induced bacteremia after a ventilation period of 180 min. This effect was diminished by using a ventilatory strategy in which PEEP was applied. The authors suggested that the results were likely attributable to ventilation-induced damage of the alveolocapillary barrier which resulted in lowering the threshold for bacterial translocation. Ventilatory strategy can also affect lung-to-systemic translocation of endotoxin. Murphy et al. [56] found that a nonprotective ventilatory strategy (tidal volume 12 ml/kg, PEEP zero) significantly increased the translocation of endotracheally instilled endotoxin in saline lung lavaged rabbits. In addition, plasma endotoxin levels were significantly greater in eventual nonsurvivors than survivors, suggesting a pathophysiological link between ventilatory strategy and outcome. Lin et al. [57] subjected rats to 1 h of protective ventilation or injurious ventilation prior to endotracheal installation of Pseudomonas aeruginosa; animals were then followed for 48 h. In the injurious group the 48-h mortality trended to higher levels (40% vs. 28%), whereas in the surviving animals an impaired host defense reflected by a cytokine response was observed. In addition, there were greater bacterial counts in the lung and serum of animals treated with the injurious ventilatory strategy. These data suggest that mechanical ventilation may alter host defense so as to predispose to pneumonia and bacteremia. Although the respiratory tract of patients with an endotracheal tube is often colonized with potential pathogenic micro-organisms, it is important to note that not every colonization results in pneumonia or translocation of bacteria.
Circulating proapoptotic soluble factors
Another important factor that may be locally produced in the lung due to overdistension and subsequently be released into the circulation is soluble Fas ligand. Fas ligand accumulates in soluble form at sites of tissue inflammation and has the potential to initiate apoptosis of leukocytes, epithelial cells, and other parenchymal cells. Dysregulation of apoptotic pathways can contribute to the epithelial injury that is characteristic of acute lung injury in humans [58]. The effects of Fas ligand are modulated by a number of factors, many of which are found in the lungs of patients with acute lung injury; these include surfactant protein A, angiotensin II, transforming growth factor (TGF) β1, and a specific Fas ligand decoy receptor (DcR3).
Recent research has demonstrated that an injurious ventilation strategy can lead to end-organ epithelial cell apoptosis, and that circulating soluble factors produced by this ventilatory strategy may be involved in this process. Using an invivo animal model of aspiration, Imai et al. [59] demonstrated that an injurious ventilatory strategy increases epithelial cellapoptosis in the kidney and the small intestine in vivo and leads to increased levels ofbiochemical markers, indicating renal dysfunction. Using an in vitro model the authors then used plasma from the ventilatedanimals and induced apoptosis in LLC-RK1 renal tubular cells;they also demonstrated that a fusion protein that blocks soluble Fas ligand(a circulating proapoptotic factor) attenuated apoptosis induction.Finally, using samples from ARDS patients involved in a clinical trial of a lung protective strategythe authors found a significant correlation between changesin soluble Fas ligand and changes in creatinine. Although very suggestive, it remains unclear whether the soluble Fas ligand is indeed produced in the lung as a consequence of an injurious ventilatory strategy and via spillover released in the systemic circulation.
Suppression of the peripheral immune response
The mechanisms described above all have in common that the involved agents, such as inflammatory mediators, bacteria and/or bacterial products, soluble proapoptotic factors, are (most likely) produced locally in the lung and released into the circulation. However, other less well studied mechanisms may also play an important role. In this respect we discuss the role of peripheral immunosuppressant and translocation of bacteria and/or products from the gut, respectively.
Suppression of the peripheral immune response may be another contributing factor in the development of MSOF. Munford and Pugin [60] recently proposed that the body’s normal responses to stress are such as to minimize systemic inflammation. They hypothesized that local inflammation is normally accompanied by systemic anti-inflammation. The body’s systemic anti-inflammatory responses to stress are not just compensatory; they dominate outside the affected local site. Coordinating local inflammation with systemic anti-inflammation enables the body to concentrate activated phagocytes and other effectors at an injured local site while preventing potentially damaging inflammation in uninvolved sites [60, 61]. However, these normally protective systemic responses may sometimes become immunosuppressive.
In 12 infants with healthy lungs we noted an increase in TNF-α and IL-6 concentrations in BAL fluid after 2 h of mechanical ventilation with a tidal volume of 10 ml/kg and a PEEP of 4 cmH2O [35]. However, the capacity of the patients’ peripheral blood lymphocytes to produce interferon γ was decreased and, after ex vivo stimulation with LPS, monocytes released less IL-6 and TNF-α. Additionally, the activity of peripheral blood natural killer cells was decreased. We confirmed this phenomenon of peripheral immunosuppression in healthy rats that had been ventilated for 4 h with several ventilatory strategies [62]. Although peripheral immunosuppression associated with mechanical ventilation might be a beneficial mechanism for regulating the intensity of pulmonary inflammation, it could at the same time be detrimental. Peripheral immunosuppression may contribute to increased vulnerability to bacteremia. Therefore it will be of utmost importance to elucidate the role and the mechanism of peripheral immunosuppression as a consequence of local inflammation in the lung.
At this stage we only can speculate on the causes of the suppressed peripheral immune function. One of the possible mechanisms is that cytokines produced locally in the lung cause leukocyte redistribution from the systemic circulation to the alveolar space [15], giving rise to a disturbance in the balance of T effector cells such as Th1/Th2 cells and/or regulatory T cells or TGF-β secreting Th3 cells [63, 64]. The altered Th1/Th2/Th3 balance in the periphery favoring Th2/3 cytokine production may represent a systemic adaptation to the proinflammatory milieu in the lung [63, 64]. However, when the proinflammatory status in the lungs is severe or persists, the peripheral systemic anti-inflammatory response may become counterproductive by supporting the course of MSOF.
Another important mechanism may be the role of the adrenergic nervous system. The physical stress of ventilation may lead to a sharp increase in catecholamine secretion, such as dopamine, adrenaline, and noradrenaline. Noradrenaline and especially adrenaline exert their effect via binding to β2-adrenergic receptors on leukocytes and other cell types. Triggering of β2-adrenergic receptors leads to the intracellular production of cAMP, which in turn leads to downregulation of the production of proinflammatory cytokines and enhances the production of anti-inflammatory cytokines such as IL-10 and TGF-β [65]. Therefore we propose that activation of β2-adrenergic receptors on cells of the peripheral immune system, especially in those organs which are densely innervated by noradrenergic fibers such as the spleen, suppresses the peripheral immune response. It is not known whether these putative mechanisms also play a role in VILI.
Translocation of bacteria and/or products from the gut
The gut may also play an important role in the translocation of bacteria or their products into the circulation. Guery et al. [66] evaluated remote consequences on the gut of lung triggered inflammatory response; neutralizing anti TNF antibody was administered to assess the role of TNF in the lung and the effect on changes in gut permeability. Rats were ventilated with larger (30 ml/kg) vs. smaller (10 ml/kg) tidal volumes. High tidal volume ventilation resulted in an increase in lung edema and gut permeability; antagonism of TNF with neutralizing antibodies abrogated the increase in gut permeability as well as lung edema. The importance of the gut as a regulator of systemic immune responses has become clearer in recent years. Moreover, it has been shown that alterations in gut bacterial flora, and consequently the level of bacterial components such as LPS, are important for initiation of the regulatory suppressive response exerted by immune cells of the gut. On the basis of results describing suppression of proinflammatory diseases by intestinal T cells we propose that either directly or by altering the gut bacterial flora mechanical ventilation is also accompanied by activation of regulatory T cells (CD4+CD25+), which may cause immunosuppression. The latter concept is supported by an experimental study from our laboratory in rats which demonstrated that modifying the bacterial gut flora by oral vancomycin treatment induces a peripheral systemic anti-inflammatory effect that is powerful enough to completely suppress acute inflammatory processes such as adjuvant arthritis [67]. Apparently increasing the level of luminal Escherichia coli or LPS induces the activation of regulatory T cells (CD4+CD25+), which can efficiently suppressing inflammation. This interrelationship between gut and translocation of bacteria may further be exacerbated by increased small intestinal epithelial apoptosis due to mechanical ventilation [59] which may predispose to translocation of bacteria from the gut into the systemic circulation. Finally, the observed peripheral immunosuppression may also affect the gut immune system directly and thereby contribute to the translocation of bacteria. The rate of translocation of intestinal bacteria can be altered with agents, for example, mechanical ventilation, that modulate immune function [68].
Individual genetic variability
Individual variations in response to mechanical ventilation and development of MSOF is likely to be another crucial factor. Recently Schmitt et al. [69] demonstrated polymorphisms in the TLR, the receptor that binds the lipid-A part of the LPS molecule, which determines responsiveness to LPS. Since mechanical ventilation may promote the translocation of LPS from the lung and/or gut to the systemic circulation, these TLR-4 polymorphisms may be of great importance in determining the susceptibility of any given patient to the inflammatory effects of injurious ventilation. Interesting in this respect is a recent study by Held et al. [70]. They observed in isolated perfused mice lungs that both LPS and overventilation (peak inspiratory pressure of 25 cmH2O) caused translocation of nuclear factor κB (NF-κB), which was abolished by pretreatment with the steroid dexamethasone. However, in LPS-resistant C3H/HeJ mice only overventilation, and not LPS, caused translocation of NF-κB and release of chemokines. These results suggest that although the signal transduction mechanisms responsible for biotrauma act at least partly via NF-κB (similar to LPS signaling), the upstream mechanisms appears to be different and independent of TLR-4.
Proposed mechanisms for mechanical ventilation and MSOF
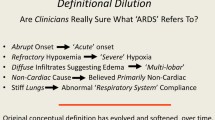
Mechanical ventilation may trigger a complex but potentially well balanced sequelae of pro- and anti-inflammatory mediators which may lead to enhanced lung healing and quicker restoration of homeostasis [71]. This inflammatory reaction is accompanied by a stress response which is reflected by increased catecholamine secretion causing suppression of peripheral immune function. The anti-inflammatory forces also limit and quell the inflammatory process throughout the body. If the anti-inflammatory mechanisms are sufficient, the potential harmful effects (in terms of an exuberant inflammatory response) are mitigated. However, when a persistent injurious ventilatory strategy is applied or preexisting lung injury exists, the immune response is more skewed to proinflammation and peripheral immunosuppression [49, 61]. This series of events may precede a multifactorial process (which is summarized in Fig. 1) that eventually result in the development of MSOF.

Proposed mechanisms for biotrauma, ventilator-induced lung injury and multiple system organ failure (MSOF) in preinjured lungs and/or injurious mechanical ventilation. When a persistent injurious ventilatory strategy is applied or preexisting lung injury exists, a dysbalance between pro- and anti-inflammation may occur, and the immune response is more skewed to proinflammation and peripheral immunosuppression. Due to an increased permeability over the alveolar membrane loss of compartmentalization occurs. Spillover of predominantly proinflammatory mediators, proapoptotic soluble factors, and extracellular heat shock protein 70 (eHSP-70) amplify the proinflammatory peripheral environment. Since the adrenergic stress response is more pronounced, as is the immune suppression via regulatory T cells, the initial protective prevention of systemic inflammation overshootes and becomes immunosuppressive. Increased immunosuppression may also occur by the increased suppressive effect of regulatory T cells due to a change in the gut microbial flora. MSOF is also accompanied by bacterial translocation from the lung and gut into the systemic circulation. Together the onset of systemic inflammation may eventually lead to MSOF. Finally, we must keep in mind that the individual susceptibility of the patient as defined by his or her genetic background, including TLR-4 polymorphisms, determines the extent to which this inflammatory reaction finally develops
Conclusion
The development of MSOF secondary to mechanical ventilation is a multifactorial process. Our proposed mechanisms linking mechanical ventilation and MSOF suggest several novel therapeutic approaches. Possible methods to abrogate injury include anti-inflammatory therapies, proinflammatory therapies, and antiapoptotic therapies. Further research is required addressing the mechanisms described above to delineate more precisely the contribution of each proposed factor, their interrelationships, and their time course. We suggest that scientific advances in immunology will offer novel approaches for the prevention of MSOF secondary to VILI.
References
Pinhu L, Whitehead T, Evans T, Griffiths M (2003) Ventilator-associated lung injury. Lancet 361:332–340
Ricard JD, Dreyfuss D, Saumon G (2003) Ventilator-induced lung injury. Eur Respir J 22:2s–9s
Gattinoni L, Carlesso E, Cadringher P, Valenza F, Vagginelli F, Chiumello D (2003) Physical and biological triggers of ventilator-induced lung injury and its prevention. Eur Respir J 22:15s-25 s
Parker JC, Townsley MI, Rippe B (1984) Increased microvascular permeability in dog lungs due to high peak airway pressure. J Appl Physiol 57:1809–1816
Dreyfuss D, Soler P, Basset G, Saumon G (1988) High inflation pressure pulmonary edema: respective effects of high airway pressure, high tidal volume, and positive end-expiratory pressure. Am Rev Respir Dis 137:1159–1164
Dreyfuss D, Saumon D (1993) Role of tidal volume, FRC, and end-inspiratory volume in the development of pulmonary edema following mechanical ventilation. Am Rev Respir Dis 148:1194–1203
Hernandez LA, Peevey KJ, Moise AA, Parker JC (1989) Chest wall restriction limits high airway pressure-induced lung injury in young rabbits. J Appl Physiol 66:2364–2368
Dreyfuss D, Saumon G (1998) Ventilator-induced lung injury: lessons from experimental studies. Am J Respir Crit Care Med 157:294–323
Slutsky AS (1999) Lung injury caused by mechanical ventilation. Chest 116:9S-15S
Parker JC, Hernandez LA, Peevy KJ (1993) Mechanisms of ventilator-induced lung injury. Crit Care Med 21:131–143
Amato MBP, Barbas CSV, Medeiros DM, Magaldi RB, Schettino GPP, Lorenzi-Filho G, Kairalla RA, Deheinzelin D, Munoz C, Oliveira R, Takagaki TY, Carvalho CR (1998) Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med 338:347–354
Acute Respiratory Distress Syndrome Network (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury the acute respiratory distress syndrome. N Engl J Med 342:1301–1308
Tremblay LN, Slutsky AS (1998) Ventilator-induced injury: from barotrauma to biotrauma. Proc Assoc Am Physicians 110:482–488
Matsuoka T, Kawano T, Miyasaka K (1994) Role of high-frequency ventilation in surfactant-depleted lung injury as measured by granulocytes. J Appl Physiol 76:539–544
Sugiura M, McCulloch PR, Wren S, Dawson RH, Froese AB (1994) Ventilator pattern influences neutrophil influx and activation in atelectasis-prone rabbit lung. J Appl Physiol 77:1355–1365
Takata M, Abe J, Tanaka H, Kitano Y, Doi S, Kohsaka T, Miyasaka K (1997) Intraalveolar expression of tumor necrosis factor-alpha gene during conventional and high-frequency ventilation. Am J Respir Crit Care Med 156:272–279
Imai Y, Kawano T, Miyasaka K, Takata M, Imai T, Okuyama K (1994) Inflammatory chemical mediators during conventional ventilation and during high frequency oscillatory ventilation. Am J Respir Crit Care Med 150:1550–1554
Tremblay L, Valenza F, Ribeiro SP, Li J, Slutsky AS (1997) Injurious ventilatory strategies increase cytokines and c-fos m-RNA expression in an isolated rat lung model. J Clin Invest 99:944–952
Slutsky AS, Tremblay LN (1998) Multiple system organ failure: is mechanical ventilation a contributing factor? Am J Respir Crit Care Med 157:1721–1725
Dreyfuss D, Saumon G (1998) From ventilator-induced lung injury to multiple organ dysfunction. Intensive Care Med 24:102–104
Dreyfuss D, Ricard JD, Saumon G (2003) On the physiologic and clinical relevance of lung-borne cytokines during ventilator-induced lung injury. Am J Respir Crit Care Med 167:1467–1471
Uhlig S, Ranieri M, Slutsky AS (2004) Biotrauma hypothesis of ventilator-induced lung injury. Am J Respir Crit Care Med 169:314–315
Dreyfuss D, Ricard JD, Saumon G. (2004) Comment: biotrauma hypothesis of ventilator-induced lung injury. Am J Respir Crit Care Med 169:315
Vlahakis NE, Schroedr MA, Limper AH, Hubmayr RD (1999) Stretch induces cytokine release by alveolar epithelial cells in vitro. Am J Physiol 227:L167–L173
Chiumello D, Pristine G, Slutsky AS (1999) Mechanical ventilation affects local and systemic cytokines in an animal model of acute respiratory distress syndrome. Am J Respir Crit Care Med 160:109–116
Herrera MT, Toledo C, Valladares F, Muros M, Diaz-Flores L, Flores C, Villar J (2003) Positive end-expiratory pressure modulates local and systemic inflammatory responses in a sepsis-induced lung injury model. Intensive Care Med 29:1345–1353
Haitsma JJ, Uhlig S, Goggel R, Verbrugge SJ, Lachmann U, Lachmann B (2000) Ventilator-induced lung injury leads to loss of alveolar and systemic compartmentalization of tumor necrosis factor-alpha. Intensive Care Med 26:1515–1522
Vreugdenhil HAE, Haitsma JJ, Jansen NJ, Zijlstra J, Plötz FB, Van Dijk JE, Lachmann B, van Vught AJ, Heijnen CJ (2003) Ventilator-induced heat shock protein 70 and cytokine mRNA expression in a model of lipopolysaccharide-induced lung inflammation. Intensive Care Med 29:915–922
Ranieri VM, Suter PM, Tortorella C, De Tullio R, Dayer JM, Brienza A, Bruno F, Slutsky AS (1999) Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome: a randomized controlled trial. JAMA 282:54–61
Ricard JD, Dreyfuss D, Saumon G (2001) Production of inflammatory cytokines in ventilator-induced lung injury: a reappraisal. Am J Respir Crit Care Med 163:1176–1180
Verbrugge SJ, Uhlig S, Neggers SJ, Martin C, Held HD, Haitsma JJ, Lachmann B (1999) Different ventilation strategies affect lung function but do not increase tumor necrosis factor-alpha and prostacyclin production in lavaged rat lungs in vivo. Anesthesiology 91:1834–1843
Wilson MR, Choudhury S, Goddard ME, O’Dea KP, Nicholson AG, Takata M (2003) High tidal volume upregulates intrapulmonary cytokines in an in vivo mouse model of ventilator-induced lung injury. J Appl Physiol 95:1385–1393
Copland IB, Kavanagh BP, Engelberts D, McKerlie C, Belik J, Post M (2003) Early changes in lung gene expression due to high tidal volume. Am J Respir Crit Care Med 168:1051–1059
Wrigge H, Uhlig U, Zinserling J, Behrends-Callsen E, Ottersbach G, Fischer M, Uhlig S, Putensen C (2004) The effects of different ventilatory settings on pulmonary and systemic inflammatory responses during major surgery. Anesth Analg 98:775–781
Plötz FB, Vreugdenhil HAE, Slutsky AS, Zijlstra J, Heijnen CJ, van Vught AJ (2002) Mechanical ventilation alters the immune response in ventilated children without lung pathology. Intensive Care Med 28:486–492
Uhlig S (2002) Ventilation-induced lung injury and mechanotransduction: stretching it too far? Am J Physiol Lung Cell Mol Physiol 282:L892–L896
Steinberg JM, Schiller HJ, Halter JM, Gatto LA, Lee HM, Pavone LA, Nieman GF (2004) Alveolar instability causes early ventilator-induced lung injury independent of neutrophils. Am J Respir Crit Care Med 169:57–63
Santos CC dos, Slutsky AS (2000) Mechanotransduction, ventilator-induced lung injury and multiple organ dysfunction syndrome. Intensive Care Med 26:638–642
Tremblay LN, Miatto D, Hamid Q, Govindarajan A, Slutsky AS (2002) Injurious ventilation induces widespread pulmonary epithelial expression of tumor necrosis factor-α and interleukin-6 messenger RNA. Crit Care Med 30:1693–1700
Haitsma JJ, Uhlig S, Goggel R, Verbrugge SJ, Lachmann U, Lachmann B (2000) Ventilator-induced lung injury leads to loss of alveolar and systemic compartmentalization of tumor necrosis factor-alpha. Intensive Care Med 26:1515–1522
Haitsma JJ, Uhlig S, Lachmann U, Verbrugge SJ, Poelma DL, Lachmann B (2002) Exogenous surfactant reduces ventilator-induced decompartmentalization of tumor necrosis factor alpha in absence of positive end-expiratory pressure. Intensive Care Med 28:1131–1137
Bethmann AN von, Brasch F, Nusing R, Vogt K, Volk HD, Muller KM, Wendel A, Uhlig S (1998) Hyperventilation induces release of cytokines from perfused mouse lung. Am J Respir Crit Care Med 157:263–272
Stuber F, Wrigge H, Schroeder S, Wetegrove S, Zinserling J, Hoeft A, Putensen C (2002) Kinetic and reversibility of mechanical ventilation-associated pulmonary and systemic inflammatory response in patients with acute lung injury. Intensive Care Med 28:834–841
Wrigge H, Zinserling J, Stuber F, von Spiegel T, Hering R, Wetegrove S, Hoeft A, Putensen C (2000) Effects of mechanical ventilation on release of cytokines into systemic circulation in patients with normal pulmonary function. Anesthesiology 93:1413–1417
Stamme C, Brasch F, von Bethmann A, Uhlig S (2002) Effect of surfactant on ventilation-induced mediator release in isolated perfused mouse lungs. Pulm Pharmacol Ther 15:455–461
Douzinas EE, Tsidemiadou PD, Pitaridis MT, Andrianakis I, Bobota-Chloraki A, Katsouyanni K, Sfyras D, Malagari K, Roussos C (1997) The regional production of cytokines and lactate in sepsis-related multiple organ failure. Am J Respir Crit Care Med 155:53–59
Plötz FB, Vreugdenhil HAE, van Vught AJ Heijnen CJ (2003) Mechanical ventilation and multiple organ failure. Lancet 361:1654
Plötz FB (2001) Ventilator-induced lung injury. Intensive Care Med 27:452
Pugin J (2002) Is the ventilator responsible for lung and systemic inflammation? Intensive Care Med 28:817–819
Ranieri VM, Giunta F, Suter PM, Slutsky AS (2000) Mechanical ventilation as a mediator of multisystem organ failure in acute respiratory distress syndrome. JAMA 284:43–44
Ribeiro SP, Rhee K, Tremblay L, Veldhuizen R, Lewis JF, Slutsky AS (2001) Heat stress attenuates ventilator-induced lung dysfunction in an ex vivo rat lung model. Am J Respir Crit Care Med 163:1451–1456
Vabulas RM, Wagner H, Schild H (2002) Heat shock proteins as ligands of toll-like receptors. Curr Top Microbiol Immunol 270:169–184
Dybdahl B, Wahba A, Lien E, Flo TH, Waage A, Qureshi N, Sellevold OF, Espevik T, Sundan A (2002) Inflammatory response after open heart surgery: release of heat-shock protein 70 and signaling through toll-like receptor-4. Circulation 105:685–690
Nahum A, Hoyt J, Schmitz L, Moody J, Shapiro R, Marini JJ (1997) Effect of mechanical ventilation strategy on dissemination of intratracheally instilled Escheria coli in dogs. Crit Care Med 25:1733–1743
Verbrugge SJC, Sorm V, van ‘t Veen A, Mouton JW, Gommers D, Lachmann B (1998) Lung overinflation without positive end-expiratory pressure promotes bacteremia after experimental Klebsiella pneumoniae inoculation. Intensive Care Med 24:172–177
Murphy DB, Cregg N, Tremblay L, Engelberts D, Laffey JG, Slutsky AS, Romaschin A, Kavanagh BP (2000) Adverse ventilatory strategy causes pulmonary-to-systemic translocation of endotoxin. Am J Respir Crit Care Med 162:27–33
Lin CY, Zhang H, Cheng KC, Slutsky AS (2003) Mechanical ventilation may increase susceptibility to the development of bacteremia. Crit Care Med 31:1429–1434
Martin TR, Nakamura M, Matute-Bello G (2003) The role of apoptosis in acute lung injury. Crit Care Med 31:S184–S188
Imai Y, Parodo J, Kajikawa O, de Perrot M, Fischer S, Edwards V, Cutz E, Liu M, Keshavjee S, Martin TR, Marshall JC, Ranieri VM, Slutsky AS (2003) Injurious mechanical ventilation and end-organ epithelial cell apoptosis and organ dysfunction in an experimental model of acute respiratory distress syndrome. JAMA 289:2104–2112
Munford RS, Pugin J (2001) Normal responses to injury prevent systemic inflammation and can be immunosuppressive. Am J Respir Crit Care Med 163:316–321
Suter PM (2002) MV causes lung inflammation and systemic immune depression: a balance of fire and ice. Intensive Care Med 28:383–385
Vreugdenhil HAE, Heijnen CJ, Plötz FB, Zijlstra J, Jansen NJG, Haitsma JJ, Lachmann B, van Vught AJ (2004) Mechanical ventilation affects peripheral immune functioning in the healthy rat. Eur Respir J 23:122–128
Weiner HL (2001) Induction and mechanism of action of transforming growth factor-beta-secreting Th3 regulatory cells. Immunol Rev 182:207–211
Cobelens PM, Kavelaars A, Vroon A, Ringeling M, van der Zee R, van Eden W, Heijnen CJ (2002) The beta 2-adrenergic agonist salbutamol potentiates oral induction of tolerance, suppressing adjuvant arthritis and antigen-specific immunity. J Immunol 169:5028–5035
Kavelaars A, Pol M van de, Zijlstra J, Heijnen CJ (1997) Beta-2-adrenergic activation enhances interleukin-8 production by human monocytes. J Neuroimmunol 177:211–216
Guery B, Welsh DA, Viget NB, Robriquet L, Fialdes P, Mason CM, Beaucaire G, Bagby GJ, Neviere R (2003) Ventilation-induced lung injury is associated with an increase in gut permeability. Shock 19:559–563
Nieuwenhuis EE, Visser MR, Kavelaars A, Cobelens PM, Fleer A, Harmsen W, Verhoef J, Akkermans LM, Heijnen CJ (2000) Oral antibiotics as a novel therapy for arthritis: evidence for a beneficial effect of intestinal Escherichia coli. Arthritis Rheum 43:2583–2589
Wells CL, Maddaus MA, Simmons RL (1988) Proposed mechanisms for the translocation of intestinal bacteria. Rev Infect Dis 110:958–979
Schmitt C, Humeny A, Becker CM, Brune K, Pahl A (2002) Polymorphisms of TLR4: rapid genotyping and reduced response to lipopolysaccharide of TLR4 mutant alleles. Clin Chem 48:161–167
Held H, Boettcher S, Hamann L, Uhlig S (2001) Ventilation-induced chemokine and cytokine release is associated with activation of NF-κB and is blocked by steroids. Am J Respir Crit Care Med 163:711–716
Plötz FB, Vught AJ van, Heijnen CJ (1999) Ventilator-induced lung inflammation: is it always harmful? Intensive Care Med 125:236
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Plötz, F.B., Slutsky, A.S., van Vught, A.J. et al. Ventilator-induced lung injury and multiple system organ failure: a critical review of facts and hypotheses. Intensive Care Med 30, 1865–1872 (2004). https://doi.org/10.1007/s00134-004-2363-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-004-2363-9