
Abstract
Objective
To compare the efficacy of early administration of noninvasive continuous positive airway pressure (nCPAP) delivered by the helmet vs. face mask to treat hematological malignancy patients with fever, pulmonary infiltrates, and hypoxemic acute respiratory failure.
Design and setting
Prospective clinical study with historical matched controls in the hematology department of a university hospital.
Patients and interventions
Seventeen hematological malignancy patients with hypoxemic acute respiratory failure defined as: moderate to severe dyspnea, tachypnea (>30–35 breaths/min), use of accessory muscles and paradoxical abdominal motion, and PaO2/FIO2 ratio less than 200. Each patient was treated with nCPAP by helmet outside the ICU in the hematological ward. Arterial oxygen saturation, heart rate, respiratory rate, and blood pressure were monitored to identify early nCPAP failure. Seventeen historical-matched controls treated in the same department with face mask CPAP were selected as control population; matching criteria were age, sex, diagnosis, and PaO2/FIO2 ratio. Primary end-points were improvement in gas exchanges and the need for endotracheal intubation.
Results
Oxygenation improved in all patients after nCPAP. No patient failed helmet nCPAP because of intolerance while eigh patients in the mask group did so. nCPAP could be applied continuously for a longer period of time in the helmet group (28.44±0.20 vs. 7.5±0.45 h).
Conclusions
Early nCPAP with helmet improves oxygenation in selected immunosuppressed patients with hypoxemic acute respiratory failure. Tolerance of helmet nCPAP seems better than that of nCPAP delivered by mask.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Noninvasive continuous positive airway pressure (nCPAP) via facial mask has been used as an effective, early treatment for cooperative patients in whom respiratory failure develops, increasing functional residual capacity [1]. nCPAP can also be performed by means of the helmet, which seems to offer important advantages [2, 3] such as a good tolerability and a satisfactory interaction between patient and environment. The efficacy of the helmet used to ventilate patients with hypoxemic acute respiratory failure (ARF) by noninvasive pressure support ventilation has been demonstrated previously [2]. Ventilatory assistance can be administered in other settings than the ICU. CPAP delivered by a helmet was used as out-of hospital treatment for patients with pulmonary edema [3]. Several studies [4, 5, 6, 7] have shown that ventilator-associated pneumonia is an important cause of mortality in immunosuppressed patients with ARF, in whom avoiding intubation might be beneficial.
This study assessed the efficacy of nCPAP delivered in the hematological ward by a helmet in comparison to face mask nCPAP for treating early hypoxemic ARF in a group of patients with hematological malignancies.
Materials and methods
This prospective clinical study was carried out at the Department of Hematology, University Hospital of Ancona, Italy, between September 2001 and August 2002. Consecutive adult hematological malignancy patients with hypoxemic ARF were enrolled. The protocol was approved by our institutional ethics committee, and all patients gave their informed consent. Subjects’ baseline characteristics are summarized in Table 1.
Helmet group
This group included nine men and eight women with a mean age of 40±8 years. Criteria for eligibility were: the presence of dyspnea, tachypnea (>30–35 breaths/min), use of accessory muscles and paradoxical abdominal motion, PaO2/FIO2 ratio less than 200 while breathing oxygen through a Venturi mask, and pulmonary infiltrates on chest radiography. Exclusion criteria were: the presence of respiratory arrest, deterioration in neurological status, hemodynamic instability (hypotension with systolic blood pressure less than 80 mmHg, cardiac ischemia on electrocardiography or ventricular arrhytmias), chronic obstructive pulmonary disease, arterial carbon dioxide (PaCO2) higher than 55 mmHg with acidosis (pH <7.30), recent esophageal or gastric surgery, expectation of a poor oncological prognosis (defined as poor responders to hematological treatment and with expectation of death in short time for the severity of the underlying disease). Hematologists and intensivists collaborated closely to treat all patients with helmet (Castar-Starmed, Mirandola, Modena, Italy). After a period of training physicians were taught to evaluate the initial clinical signs of respiratory fatigue and radiological evidence of pulmonary infiltrates. Intensivists were alerted and arterial blood gas (ABG) level was determined at baseline. If the PaO2/FIO2 ratio was less than 200 mmHg while the patient was receiving oxygen through the Venturi mask (FIO2 0.5), heart rate, respiratory rate, arterial oxygen saturation, and blood pressure were monitored. High-flow CPAP (Vital Signs, Brighton, UK) was set at 8 cmH2O with FIO2 0.6 controlled by means of an oxymeter (Miniox II Oxygen Monitor, Catalyst Research Owings Mills, Md., USA). Subsequently ABG levels were determined 2, 4, 6, and 12 h after the start of nCPAP. Nurses were asked to maintain periods of nCPAP as long as possible, depending on the patient’s tolerance which was evaluated during the first 24 h as very good (3), good (2), medium (1), or bad (0). If the application of nCPAP was not successful, patients underwent intubation without delay, following predetermined criteria (PaO2 <65 mmHg with FIO2 >0.6), conditions requiring intubation to protect airways, copious secretions, hypercapnia with pH at 7.30 or less, hemodynamic instability, inability to correct dyspnea, and inability to tolerate device.
Historically matched control group
Seventeen patients were selected as a matched control group from a total of 343 patients admitted to the Department of Hematology in the 19 preceding months with diagnosis of ARF (11 men, 6 women; mean age 45±9 years). They received face-mask CPAP and the same medical treatment in the hematological ward as patients with helmet. Controls had the same enrollment criteria as described for the helmet group. The physician who made the selection was unaware of the study results. For each patient treated with helmet nCPAP, one matching control was selected following predetermined criteria: age within 10 years of that of the treated patients; PaO2/FIO2 ratio while breathing oxygen through a Venturi mask within 10 points of the value for the treated patients; sex; and diagnosis of hemopathy. In matching each patient we gave priority to the type of hematological disease and its stage and to the patient’s age, sex, and PaO2/FIO2 ratio because the outcome of these patients and the decision to undertake intubation depended on the initial severity of illness. All patients were treated with face mask nCPAP (Gibeck, Upplands, Sweden). High-flow CPAP was set at 8 cmH2O with FIO2 0.6, using the same CPAP system and oxymeter of the helmet group. Subsequently ABG levels were determined.
End-points and definitions
Primary end-points were improvement in gas exchanges and need for intubation. Secondary end-points included duration of ventilatory assistance and complications related to technique and mortality. Improvement in gas exchange was defined as ability to increase the PaO2/FIO2 ratio to more than 200 or as an increase in this ratio more than 100 above baseline. Sustained improvement was defined as the ability to maintain the improved PaO2/FIO2 ratio until nCPAP was discontinued. Criteria for diagnosis of bacterial pneumonia and adult respiratory distress syndrome followed consensus guidelines [8, 9].
Statistical analysis
Results are expressed as mean ±SD. The two-way analysis of variance test was used to compare the PaO2/FIO2 values measured at baseline and 2, 4, 6, and 12 after the start of treatment. Differences with p of 0.05 or less were considered significant. Patients characteristics were compared using Student’s unpaired t test for continuous data and Fisher’s exact test for categorical data. Death rate was assessed by Kaplan-Meier analysis and Mantel-Cox log-rank test. MedCalc version 7.1.0.0 (MedCalc Software, Belgium) was used for all analyses.
Results
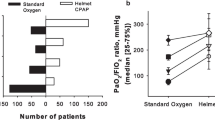
The two groups had a similar improvement in PaO2/FIO2 ratio (Table 2) within the first 2 h. Sustained improvement in PaO2/FIO2 ratio was observed in all 17 patients in the helmet group and in 13 patients (76%) in the mask group (p<0.1). In the helmet group the values of the PaO2/FIO2 ratio at 4, 6, and 12 h were significantly higher than baseline (p<0.05) while in the mask group the ratio was significantly higher than baseline at 4 and 6 h (p<0.05) but not at 12 h (p=0.07). No patient required intubation in the helmet group, compared to seven (41%) in the mask group (p<0.01). In the helmet group the mean duration of continuous application of nCPAP without disconnection and the total duration of nCPAP were longer than in the mask group (28.44±0.2 vs. 7.5±0.45 h, p<0.0001) and 34.13±0.19 vs. 28.15±0.35 h, p<0.0001) respectively). nCPAP was better tolerated in the helmet group than in the mask group, where tolerance was evaluated by nurses as bad in 8 cases (47%, p<0.01). No patient in the helmet group had complications related to nCPAP, while two patients (12%) in the mask group had skin necrosis (p=0.48), and two (12%) had eye irritation (p=0.48).
As evidenced by Kaplan-Meier analysis, mortality differed significantly between the two groups (p<0.05); four patients in the helmet group (23%) and eight (47%) in the mask group died in the Hematology Department. This represented an apparent reduction of 49% in the risk of death (Fig. 1). Seven of the eight patients in the mask group who died were intubated for significant worsening of gas exchange and transferred to ICU, where they developed serious complications leading to death. Only one patient of the mask group died in the Hematology Department after refusing intubation. In contrast, the four deaths in the helmet group occurred in the Hematology Department after multiple organ failure and gas exchange deterioration. All of these four patients had refused endotracheal intubation. One patient in the helmet group (6%) and four in the mask group (24%) died due to septic shock; two deaths occurred as a consequence of the hematological disease (one in the helmet group and one in the mask group, 6% each), three patients in the mask group (18%) died due to intractable hypoxia and cardiac arrest, and two patients in the helmet group (12%) died after the development of cardiogenic shock.

Death rate assessed by Kaplan-Meier analysis. Four patients in the helmet group (23%) vs. eight (47%) in the face mask group died in the Hematology Department, representing an apparent risk of death reduction of 49%. Hospital mortality in the helmet group was significantly lower than that in the face mask group (Mantel-Cox log-rank test, p<0.05)
Discussion
We used helmet nCPAP to treat 17 selected hematological malignancy patients at an early stage of hypoxemic ARF in the Hematology Department, reducing intubation and avoiding ICU admission, often related to an increased risk of infectious complications. In our study nCPAP was successfully applied in all patients, but helmet nCPAP was better tolerated than mask nCPAP, avoiding skin breakdown and allowing a longer period of continuous treatment with fewer endotracheal intubations. These advantages may explain at least in part the lower mortality observed in the helmet group. However, we are aware that the choice of matched historical controls represents a major limitation of this pilot study, not allowing a definitive conclusion on mortality. Interdisciplinary collaboration between hematologists and intensivists appears crucial for achieving an early implementation of noninvasive mechanical ventilation and improving the quality of care. Future randomized studies are needed to confirm our results.
References
Kats JA, Mark JD (1985) Inspiratory work with and without continuous airway pressure in patient with acute respiratory failure. Anesthesiology 63:598–607
Antonelli M, Conti G, Pelosi P, Gregoretti C, Pennisi MA, Costa R, Severgnini P, Chiaranda M, Proietti R (2002) New treatment of acute hypoxemic respiratory failure: noninvasive pressure support ventilation delivered by helmet—A pilot controlled trial. Crit Care Med 30:602–608
Foti G, Cazzaniga M, Villa F (1999) Out of hospital treatment of acute pulmonary edema (PE) by non-invasive continuous positive airway pressure (CPAP): feasibility and efficacy. Intensive Care Med S112:A431
Hilbet G, Gruson D, Vargas F, Valentino R, Gbikpi-Benissan G, Dupon M, Reiffers J, Cardinaud JP (2001) Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure. N Engl J Med 344:481–487
Conti G, Marino P, Cogliati A, Dell’Utri D, Lappa A, Rosa G, Gasparetto A (1998) Noninvasive ventilation for the treatment of acute respiratory failure in patients with hematologic malignancies: a pilot study. Intensive Care Med 24:1283–1288
Antonelli M, Conti G, Bufi M, Costa MG, Lappa A, Rocco M, Gasparetto A, Meduri GU (2000) Noninvasive ventilation for treatment of acute respiratory failure in patients undergoing solid organ transplantation: a randomized trial. JAMA 283:235–241
Hilbert G, Gruson D, Vargas F, Valentino R, Chene G, Boiron JM, Pigneux A, Reiffers J, Gbikpi-Benissan G, Cardinaud JP (2000) Noninvasive continuous positive airway pressure in neutropenic patients with acute respiratory failure requiring intensive care unit admission. Crit Care Med 28:3185–3190
Meduri Gu, Chastre J (1992) The standardization of bronchoscopic technique for ventilator-associated pneumonia. Chest 102:557–564
Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, Legall JR, Morris A, Spragg R (1994) The American-European Consensus Conference on ARDS. Am J Respir Crit Care Med 149:818–824
Antonelli M, Pennisi MA, Conti G, Bello G, Maggiore SM, Michetti V, Cavaliere F, Proietti R (2003) Fiberoptic bronchoscopy during noninvasive positive pressure ventilation delivered by helmet. Intensive Care Med 29:126–129
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Principi, T., Pantanetti, S., Catani, F. et al. Noninvasive continuous positive airway pressure delivered by helmet in hematological malignancy patients with hypoxemic acute respiratory failure. Intensive Care Med 30, 147–150 (2004). https://doi.org/10.1007/s00134-003-2056-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-003-2056-9