
Abstract
Objectives
To analyse 1-year mortality and functional disability outcomes and resource use in critical stroke patients admitted to ICU.
Design and setting
Multi-centre, prospective, observational study in 28 Spanish hospitals.
Patients
Patients admitted for acute stroke from March–August 1999.
Intervention
Collection of data on: severity by Apache III and Glasgow Coma Score; neurological lesion, hospital and 1-year mortality; functional disability at 1 year by Barthel Index and Glasgow Outcome Scale; ICU length of stay, life support techniques, and neurosurgical interventions.
Measurement and results
We studied 132 patients: 21% with subarachnoid haemorrhage (SAH), 58% intracerebral haemorrhage (ICH), 20% ischaemic stroke (ISC); Apache III 63±29 ICU stay 13±12 days; 74% required mechanical ventilation. Hospital and 1-year mortality was 33% (22%:ISC, 32%:SAH, 37%:ICH) and 53.8% (66%:ISC, 39%:SAH, 54%:ICH), respectively. Age, APACHE III, and diagnosis defined hospital mortality. Age, APACHE III, and Glasgow Coma Score defined 1-year mortality. Barthel Index score improved (P<0.001) between discharge and 1 year; 73% of patients presented severe disability at discharge vs. 26% at 1 year; 8% minimal/no disability at discharge vs. 43.3% at 1 year. Only 17% of subarachnoid haemorrhage patients presented severe disability at 1 year. Admission Apache III and hospital-discharge Barthel Index scores were related to functional outcome at 1 year.
Conclusions
Critical stroke patients are characterized by high severity of illness, elevated resource consumption, and poor outcomes that are mainly influenced by severity and age. Glasgow Coma Score-measured neurological severity is the main determinant of future functional capacity, which is greater at 1 year.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cerebrovascular disease (stroke) is an increasingly important social health issue. It has become the second leading cause of death worldwide [1, 2] and is the main cause of long-term disability in developed countries [3]. The different types of stroke [intracerebral haemorrhage (ICH), ischaemic (ISC), and subarachnoid haemorrhage (SAH)] have distinct pathophysiologic mechanisms and currently receive specific treatments in their acute phase, including recently developed endovascular and thrombolytic approaches to patients with SAH and ISC, respectively [4, 5].
Although a large number of stroke victims arrive at Emergency , relatively few of these patients are admitted to intensive care (ICU) [6]. ICU admission is more frequent in centres with neurosurgical facilities, and more ICH and SAH than ISC patients are admitted, probably related to the low level of consciousness initially presented by the former groups. ICU admission selection seems more related to the age of the patient than to criteria of viability or efficacy, with a preferential selection of younger patients [7].
The EVASCAN multi-centre project on continuous quality improvement of stroke management in ICUs and Emergency Departments of Southern Spain conducted a prospective study on the characteristics of patients admitted to ICUs for stroke and on the management and consumption of critical care resources for these patients [6]. The study outcomes were the mortality and disability level (functional independence) during the hospital stay and 1 year after ICU discharge.
Material and methods
Participating hospitals and ICUs
Twenty-eight hospitals participated in the study, forming 80.6% of the hospitals in Andalusia (a region in Southern Spain of 7.2 million inhabitants): four referral centres (Spanish level III), each with neurosurgery and interventionist neuroradiology departments and >750 beds; eight level II hospitals (three with neurosurgery departments) with a mean of 350 beds; and 16 district hospitals (level I) with < 300 beds.
Patients
Patients were consecutively recruited for the study through three cross-sectional samplings of 24-h duration conducted on the 5th, 15th, and 25th of each month from 5 March 1999–25 August 1999 (6 months). The samplings included all patients with stroke admitted to or already in the ICU during these times in the ICUs studied. The criteria for ICU admission were low level of consciousness, need for life support measures and/or specific neurosurgical procedures, and the possibility of recovery, as assessed by the physician responsible for the patient's care. We also recorded the total number of patients admitted to the hospitals and emergency departments on the sampling days.
The clinical diagnostic criteria proposed in the NINDS study were used [8]. The patients were diagnosed with ISC, ICH, or SAH according to admission computed tomography (CT) scan findings of hypodense lesions, cerebral haematoma, or blood in the subarachnoid space, respectively. Patients with acute traumatic cerebral injuries or with other types of brain injury were excluded from the study. In Spain, ICUs are of a closed format type and specialist physicians are responsible for the patients, in consultation with neurologists and neurosurgeons (with 24-h presence in hospitals with these departments). After their discharge, all survivors attended regular rehabilitation sessions at the hospitals.
Measurement instruments
Severity assessment
The severity of illness was evaluated by the APACHE III score [9] measured during the first 24 h of admission to the ICU. The level of consciousness was assessed with the Glasgow Coma Scale (GCS) [10].
Functional outcome
Disability level at ICU discharge and 12 months later was assessed with two reliable methods widely used in neurological patients and adapted for application to stroke patients. The Barthel index [11] measures the ability to perform the daily life activities of eating, bathing, walking, and using the toilet; patients who can perform all activities with complete independence receive a score of 100. The Glasgow Outcome Scale (GOS) [12] provides a global assessment of function: a score of 1 indicates a good recovery; 2, moderate disability; 3, severe disability; 4, vegetative state; and 5, death. The range of outcomes was described by classifying the patients as having minimal or no disability (Barthel index score, >90; Glasgow Outcome Score, 1), moderate disability (Barthel index, 55–90; Glasgow Outcome Score 2), or severe disability (Barthel index, <55; Glasgow Outcome Score, 3 or 4), following NINDS criteria [8]. The outcome measures were assessed by a single physician (I.G.) with specialist training and experience in the collection of quality of life and outcome data.
Life support measures and resource consumption
Data were gathered on: need for and time on mechanical ventilation; administration of hypotensive and vasoactive drug infusions or antiarrhythmic, sedative, and relaxant drug infusions; and use of ventricular catheter, intracranial pressure monitoring, angiographic/intravascular procedures, neurosurgery, and tracheotomy. The ICU length of stay was also recorded. Treatment was uniform between centres and was based on guidelines of the Spanish and Andalusian Intensive Care Societies. Similar protocols were used in all centres for intubation, mechanical ventilation, and intracranial pressure monitoring. The treatment protocol for patients with ISC only specifies medical treatment of elevated intracranial pressure; neither decompressive hemicraniectomy, hypothermia, nor thrombolysis is applied in these cases. In patients with SAH, intraventricular catheters were used to monitor the intracranial pressure.
Independent and dependent variables
We considered age, severity of illness (APACHE III score in first 24 h and GCS), and stroke type (ISC, ICH or SAH) as independent variables in the study. Dependent variables were the mortality and the functional outcome (as a quality of life indicator) at hospital discharge and after 12 months.
Reproducibility of the results and quality control of the data
Every ICU studied designated a physician to be responsible for data collection and to undergo training for this purpose. Explanatory leaflets and data collection sheets were produced. Doubts or queries on data collection were immediately answered by the data collection central unit (at Virgen de las Nieves University Hospital, Granada, Spain). This unit was responsible for checking the data from the ICUs and ensuring correct completion of documentation.
All data were introduced by a single investigator into a database created with Microsoft Access. Quality control measures included a procedure to prevent the entry of data incompatible with possible value ranges as well as the use of two different databases that were subsequently compared.
All follow-up data were gathered telephonically by a single physician at the central unit who had participated in numerous surveys of this type [6] and was trained in the administration of disability and quality-of-life questionnaires.
Life-sustaining care was withdrawn following the same protocol and according to identical brain death criteria in all the hospitals in the study. Besides cases of brain death, life support is also discontinued at the request of the family when there is no hope of recovery.
Statistical analysis
Continuous variables were expressed as means±standard deviation and categorical variables were expressed as actual numbers and percentages. The Student's t-test for quantitative variables was used for the comparison of the means of two categories and the analysis of variance for the comparison of more than two. The Newman-Keul's test was then performed if there were statistically significant differences. Categorical variables were analysed with the Chi-square test. Comparison of paired samples was used to study the evolution of quantitative variables over time.
The independent variables that had significant association with mortality and disability level (quality of life) at discharge and at 1 year were assessed with univariate analysis. The impact of the significant variables on the mortality, functional status, and level of disability was established using multivariate analysis with multiple logistic and linear regression. Because the diagnosis variable had three categories (ISC, ICH, and SAH), it was transformed into two dummy variables for the analysis: "Diagnosis 1" variable represented a value of 0 in ICH and ISC and of 1 in SAH; and "Diagnosis 2" a value of 1 in ICH and of 0 in ISC and SAH. These dummy variables were also used in a multivariate analysis with logistic regression to relate the 1-year mortality to the Glasgow Coma Score variable.
All statistical tests were two-tailed and statistical significance was accepted at P<0.05. The statistical analysis was performed using the SPSS 9.0 statistical software package.
Results
Characteristics of the ICU population from March 1999–August 1999
A total of 2,926 patients were admitted to the 28 ICUs in the study, but only 16 ICUs (57%: level III, 43%; level II) admitted any patients with stroke, a total of 132 patients, representing 5.9% of the entire population of the participating ICUs during the study period.
Epidemiological data
The mean age of the 132 patients was 55.7±15.8 years and 61% were males. There was a significantly lower incidence of ISC and SAH vs. ICH (Table 1).
Severity of illness
The mean first-24 h Apache III score was 63.2±29.2. The APACHE III-measured severity of patients with ISC was significantly worse than that of ICH patients and, especially, SAH patients. The mean Glasgow Coma Score at ICU admission was 8.2±4, with no differences according to stroke type.
Neurological characteristics
All ISC patients suffered MCA territory ischaemia (2/3 or complete) with the exception of four cases of vertebro-basilar territory ischaemia. ICH was supratentorial in 69/77 cases. All SAH patients presented a Hunt and Hess score >2.
Life support measures and resource consumption
Mechanical ventilation was applied to 74% of the patients for a mean of 9.2±3 days, and 24% required tracheotomy (Table 2). MV was ordered for low level of consciousness in the large majority of cases (82%) and post-operatively in the remainder. No stroke patient was ventilated outside the ICU in any of the hospitals studied. Hypotensive drugs were administered to 57%, vasoactive drugs to 31%, and intravenous sedation to 73% of the patients. Ventricular drainage was performed in 31%, intracranial pressure monitoring in 25%, interventionist angiography/angiology diagnostic methods in 30%, and neurosurgical treatment in 22% of the patients. The mean ICU stay was 13±12.5 days.
Mortality
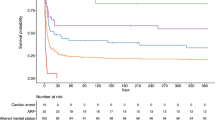
Global hospital mortality was 33% and mortality at 1 year after ICU discharge was 53% (P = 0.04). Patients with ISC had the lowest hospital mortality rate (22% vs. 32% for SAH and 37% for ICH) but the highest mortality rate after 1 year (66% vs. 39% for SAH and 54% for ICH) Mortality at 12 months was similar to that at ICU discharge in SAH patients (39% vs. 32%, n.s.) but higher in ISC (66%, vs. 22% P<0.001) and ICH (54% vs. 37%, P<0.001) patients. Univariate analysis showed that at ICU discharge and after 1 year, survivors and non-survivors differed in their age, first-24 h APACHE III score, and admission Glasgow Coma Score (Table 3). Multivariate study with logistic regression revealed that the patient age, APACHE III score, and dummy-type diagnostic variable defined the hospital mortality. For the same age and APACHE III score, SAH showed a mortality 5.74-fold that of ISC and ICH a mortality 4.1-fold that of ISC. Another multivariate analysis with logistic regression showed that the mortality at 1 year depended on age, APACHE III score at ICU admission, and Glasgow Coma Score (transformed into two dummy variables) (Table 4).
Disability level
Functional outcome at ICU discharge was poor, both overall (73% of patients had severe disability, 18% moderate disability and only 8% minimal/no disability) and for each stroke type (Table 5). However, only 57% of SAH patients presented severe disability, compared with 85% of ISH and 74% of ICH patients. Moderate disability was presented by 26% of SAH, 10% of ISC, and 19% of ICH patients; and minimal/no disability by 15% of SAH, 5% of ISC, and 6% of ICH patients.
At 1 year after discharge, 64.7% of SAH patients had minimal/no disability, compared with only 25% of ISC and 37% of ICH patients, whereas only 17% of SAH patients presented severe disability, compared with 50% of ISC and 25% of ICH patients.
Surviving patients had a Barthel Index score of 29.4±35.6 at hospital discharge and of 73±34.4 at 1 year. The hospital-discharge Barthel Index score of the group that survived to 1 year was 35.7±35.9, with a statistically significant correlation between the discharge and 1-year follow-up scores (r = 0.579, P<0.001), demonstrating a significant (P<0.001) improvement in the BI-measured functional status of these patients.
Multivariate analysis with logistic regression showed that the variables associated with the BI-measured functional outcome at 1 year were the APACHE III-measured severity of illness at ICU admission and the Barthel Index score at hospital discharge. Other variables, such as age and type of stroke (ISC, ICH or SAH) contributed no additional information (Table 5). Two patients were lost to the follow-up study at 12 months.
Discussion
We prospectively studied a representative cohort of ICU-admitted patients with stroke during a 6-month period in a region of southern Spain of over 7 million inhabitants. Stroke patients represented less than 6% of the total admissions to the ICUs in the study and only half of these ICUs, in higher-level hospitals (Spanish levels II and III), admitted any patient with stroke during this time. These stroke patients were characterized by a high consumption of resources and an intensive use of life support measures, especially mechanical ventilation. Their mortality rate after 1 year was very high, at over 50%. Among survivors, there was a recovery in functional outcome and ability to perform basic daily activities between hospital discharge and 1-year follow-up.
Very few patients with acute stroke are admitted to ICU compared with other types of patient, despite the high incidence of this disease in hospital emergency areas [7]. These patients constituted 3.9% of the US APACHE III database of critical patients [9] and a large British study using APACHE II found similar rates [13]. According to the Spanish APACHE III-based study (PAEEC) of 86 ICUs, which disclosed a higher severity among Spanish ICU patients, stroke represented 3.3% of ICU admissions [6]. In the present study, 5 years later, the proportion of these patients remains low, at 5.9% of ICU admissions in Southern Spain. The fact that only half of the ICUs admitted any stroke patient reflects the practice of transferring stroke patients, especially haemorrhagic stroke patients (SAH and ICH), to referral centres from the emergency areas of other hospitals.
The present ICU stroke population showed elevated resource consumption with intense therapeutic activity, including specific diagnostic and monitoring procedures and a heavy use of life support techniques, notably mechanical ventilation (74.2%). The need for mechanical ventilation is a recognized severity marker in ICU stroke patients, and it is associated with a very high mortality (60%–100%) that varies according to the motive for respiratory support [14]. A recent European prospective study of 52 patients with ischaemic stroke on mechanical ventilation described a mortality of around 80% at 3 months [15].
The high hospital mortality of stroke patients has been widely reported. The British study cited above described 55% hospital mortality among ICU-admitted stroke patients [13], similar to the non-adjusted hospital mortality rate reported by the Spanish PAEEC study [6]. Our findings for SAH patients, the paradigm of ICU stroke admission, are also consistent with previous reports [16, 17]. The present study highlights the need for further investigation of the poor clinical outcomes of patients with acute stroke. There have been recent therapeutic advances, including early non-invasive obliteration of cerebral aneurysm in SAH patients and the use of thrombolytic therapy in ISC patients [18], who were traditionally treated outside the ICU, especially in Europe. However, there remains great scope for improvements.
We found that the hospital mortality was related to the age, APACHE III score, and type of stroke. Thus, the hospital mortality was higher among patients with SAH and ICH than among those with ISC for the same APACHE III-measured severity and age. At 1 year, the diagnostic variable was replaced in the multivariate model by the GCS, despite the inclusion of the Glasgow Coma Score within the APACHE IIII formula. There was a considerable increase in the proportion of ISC patients dying in the first year after hospital discharge, with a smaller increase among ICH patients and virtually no increase among those with SAH. Other authors, reporting on non-ICU settings, attributed this high 1-year mortality among ISC patients largely to cardiovascular and coronary comorbidities [19]. Our study suggests that the 1-year mortality is related to the degree of neurological impairment and the hospital mortality is mainly influenced by the type of stroke.
Mortality in stroke has been related to multiple clinical and radiological parameters. In ISC, half of the mortality has been attributed to infectious and medical complications and half to neurological complications [20]; the short-term prognosis has been related to age, signs of neurological involvement, and basic analytical parameters on admission [21]. The long-term (3–8 years) prognosis has been related to a history of cardiovascular disease, the level of activity at hospital discharge [22], and other family, social, or ethnic factors [23]. In an attempt to simplify the prediction of hospital outcomes, retrospective studies demonstrated the validity of the previous APACHE II system and its Glasgow Coma Score variable, in equal measure, for predicting mortality in ischaemic stroke [24]. This was confirmed by a recent prospective study [25]. In ICH, survival prediction has classically been linked to the severity of the episode (measured by Glasgow Coma Score and blood pressure) and, to a lesser degree, to the haemorrhage size [26, 27]. In SAH, the mortality has been related to the initial severity (Hunt and Hess scale), the CT findings (Fisher's scale) [28], and the APACHE II-measured severity on admission [29].
Many of the above prognostic items, although not independently studied in the present work, are gathered in the APACHE III system, validated for Spanish critical patients by our group [6]. APACHE III introduced important novelties: the Glasgow Coma Score measurement of coma depth (used in both versions) is given special weighting, so that a higher APACHE III score is recorded for the deeper coma states compared with APACHE II, to which the Glasgow Coma Score score is linearly related. In our study, the APACHE III score was the main predictor of hospital mortality and also formed part of the 1-year mortality model. Another finding of interest was that age emerged as an independent variable in the logistical regression model for the hospital mortality, despite its inclusion in APACHE III with special weighting. This suggests that the evolution of elderly patients with stroke may be worse than that of elderly patients with other critical diseases. The influence of age on the 1-year mortality was even greater: not only did age enter the logistic regression model for 1-year mortality prediction but the Odds Ratio increased from 1.048 to 1.088 with a very moderate increment in the APACHE III ratio from 1.022 to 1.03. The Glasgow Coma Score entered the 1-year mortality model (despite its inclusion in APACHE III) but did not enter the hospital mortality model, which implies that the depth of coma, a measure of the neurological impact of the disease, has greater influence on the 1-year mortality than the hospital mortality. Thus, patients with major neurological impairment who survive to hospital discharge will have a high mortality, considerably higher than those with lesser neurological impairment. This underlines our conclusion that 1-year mortality depends more on the neurological severity than on the type of stroke.
The quality of life after ICU discharge provides one of the best means to evaluate the performance of ICUs, as previously argued by our group [30, 31]. We used the Barthel Index and the GOS, widely used to assess outcomes in this type of patient [8]. Among survivors, there was a recovery in the functional outcome and ability to perform basic daily activities between hospital discharge and 1-year follow-up. This was not solely due to the post-discharge mortality of patients with worse disability level, as shown by the survivor follow-up data. The 1-year functional outcomes were poor and moderate for ISC and ICH patients, respectively, whereas SAH survivors were self-sufficient and their scores were practically normal. However, multivariate analysis revealed that the clinical functional outcome at 1 year, measured by ability to perform basic activities, was mainly related to the APACHE III-measured severity of illness at admission and to the functional status at hospital discharge. The present findings are consistent with earlier reports that the factors that influence mortality outcomes also predict the functional outcome of these patients, i.e., severity of stroke, age and comorbidities [32]. A recent study of ICU-admitted stroke patients found a very elevated mortality (52% at 3 months) and poor BI-measured functional outcome, which were related to haemorrhagic stroke, fixed dilated pupils, and a GCS<10 [33]
Neurological patients currently admitted to ICU are characterized by an elevated consumption of resources and a high hospital and 1-year mortality. Survivors have a high level of disability that improves over the year after hospital discharge and appears to be related to the degree of neurological involvement. The mortality and functional outcome after 1 year can be predicted by the severity of illness at admission.
References
Murray CJL, Lopez AD (1997) Mortality by cause for eight regions of the world: Global burden of Disease Study. Lancet 349:1269–1276
Eastern Stroke and coronary heart disease collaborative research Group (1998) Blood pressure, cholesterol, and stroke in eastern Asia Lancet 352:1801–1807
Helgason CM, Wolf PA (1997) American Heart Association Prevention Conference IV: prevention and rehabilitation of stroke: executive summary. Circulation 96:701–707
Thorvaldsen P, Kuulasmaa K, Rajakangas AM, Rastenyte D, Sarti C, Wilhemsen L (1997) Stroke trends in the WHO MONICA project. Stroke 28:500–506
Brott T, Bogousslavsky J (2000) Treatment of acute stroke ischemic stroke. N Engl J Med 343:710–722
Navarrete-Navarro P, García-Alcántara A, Murillo-Cabezas F, G. Vazquez-Mata, Fernández S., Jimenez JM, Galindo I, Rivera R., Dominguez JM, Pino E, Nacle B, Muñoz A (2000) Acute Stroke and Emergency and Critical Care Departments in Andalusia. The EVASCAN project experience. Med Intensiva 24:257–266
Rivera Fernández R, Vázquez Mata G, Bravo M, Aguayo E, Zimmerman J, Wagner D, Knaus W (1998) The Apache III prognostic system: customized mortality predictions for Spanish ICU patients. Intensive Care Med 24:574–581
The National Institute of Neurological Disorder and rt-PA Stroke Study Group (1995) Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 333:1581–1587
Knaus WA, Wagner DP, Draper EA, Zimmerman J, JE Begner, Bastos PA, Sirio CA, Murphy DJ, Lotring T, Damiano A, Harrell FE (1991) The Apache III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest 100:1619–1636
Teasdale G, Jennet B (1974) Assessment of coma and impaired consciousness : a practical scale. Lancet 2:81–84
Mahoney FI, Barthel DW (1965) Functional evaluation: the Barthel index. Md Med J 14:61–65
Teasdale G, Knill-Jones R, van der Sande J (1978) Observer variability in assessing impaired consciousness and coma. J Neurol Neurosurg Psychiatry 41:603–610
Goldhill DR, Sumner A (1998) Outcome of Intensive care patients in a group of British intensive care units. Crit Care Med 26:1337–1345
Steiner T, Mendoza G, De Georgia M, Schellinger P, Holle R, Hacke W (1997) Prognosis of stroke patients requiring mechanical ventilation in a neurological critical care unit. Stroke 28:711–715
Berrouschot J, Rossler A, Koster J, Scheineder D (2000) Mechanical ventilation in patients with hemispheric ischemic stroke. Crit Care Med 28:2956–2961
Gruber A, Reinprecht A, Illievich UM, Fitzgerald R, Dietrich W, Czech T, Richling B (1999) Extracerebral organ dysfunction and neurologic outcome after aneurysmal subarachnoid hemorrhage. Crit Care Med 27:505–514
Solenski NJ, Haley CE, Kassel NF, Kongable G, Germanson T, Truskowski L, Torner JC (1995) Medical complications of aneurysmal subarachnoid hemorrhage: a report of the multicenter, cooperative aneurysm study. Crit Care Med 23:1007–1017
Kiatkowski TG, Libman RB, Frankel M, Tilley BC, Morgenstern LB, Mei L, Broderick J, Lewandowski CA, Marler JR, Levine SR, Brott T, for the National Institute of Neurological Disorders and Stroke. Recombinant Tissue Plasminogen Activator Stroke Study Group (1999) Effects of tissue plasminogen activator for acute ischemic stroke at one year. N Engl J Med 340:1781–1787
White HD, Simes RJ, Anderson NE, Hankey GJ, Watson JD, Hunt D, Colquhoun D, Glasziou P, MacMahon S, Kirby A, West MJ, Tonkin AM (2000) Pravastatin therapy and the risk of stroke. N Engl J Med 343:317–326
Johnston KC, Li JY, Lyden PD, Hanson SK, Feasby TE, RJ, Faught RE, Haley EC. for the RANTTAS Investigators (1998) Medical and neurological complications of ischemic stroke. Experience from the RANTTAS trial. Stroke 29:447–453
Czlonkowska A, Ryglewicz D, Lechowsicz W (1997) Basic analytical parameters as the predictive factors for 30-day case fatality rate in stroke. Acta Neurol Scand 95:121–124
Chambers BR, Norris JW, Shurvell BL, Hachinski VC (1987) Prognosis of acute stroke. Neurology;37:221–225
Bonita R, Ford MA, Stewart AW (1988) Predicting survival after stroke: a three-year follow-up. Stroke 19:669–673
Weingarten S, Bolus R, Riedinger MS, Maldonado L, Stein S, Ellrodt G (1990) The principle of parsimony: Glasgow coma scale predicts mortality as well as the Apache II score for stroke patients. Stroke 21:1280 -1282
Rordof G, Koroshetz W, Efird JT, Cramer SC (2000) Predictors of mortality in stroke patients admitted to an intensive care unit. Crit Care Med 18:1301–1305
Portenoy RK, Lipton RB, Berger AR, Lesser ML, Lantos G (1987) Intracerebral haemorrhage: a model for the prediction of outcome. J Neurol Neurosurg Psychiatry 50:976–979
Tuhrim S, Dambrosia JM, Price TR, Mohr JP, Wolf PA, Heyman A, Kase CS (1988) Prediction of intracerebral hemorrhage survival. Ann Neurol 24:258–263
Elliott JP, Le Roux PD, Ransom G, Newell DW, Grady MS, Winn HR (1996) Predicting length of hospital stay and cost by aneurysm grade on admission. J Neurosurg 85:388–391
Stachniak JB, Layon AJ, Day AL, Gallagher TJ (1996) Craniotomy for intracranial aneurysm and SAH. Is course cost or outcome affected by age. Stroke 27:276–281
Vazquez-Mata G, Rivera-Fernández R, Gonzalez A, Delgado M, Torres JM, Raya A, Aguayo E (1992) Factors related to quality of life 12 months after discharge from an Intensive Care Unit. Crit Care Med 20:1257–1262
Rivera-Fernández R, Sanchez JJ, Abizanda R,Vazquez-Mata G (2001) Quality of life before intensive care admission and its influence on resource utilization and mortality rate. Crit Care Med 29:1701–1709
Cifu SX, Stewart DG (1999) Factors affecting functional outcome after stroke: a critical review of rehabilitation interventions. Arch Phys Med Rehabil: 80 [Suppl 1]: S35-S39
Fanshawe M, Venkatesh B, Boots RJ (2002) Outcome of stroke patients admitted to intensive care: experience from an Australian teaching hospital. Anaesth Intensive Care 30:628–632
Author information
Authors and Affiliations
Corresponding author
Additional information
An editorial regarding this article can be found in the same issue (http://dx.doi.org/10.1007/s00134-003-1840-x)
Rights and permissions
About this article
Cite this article
Navarrete-Navarro, P., Rivera-Fernández, R., López-Mutuberría, M.T. et al. Outcome prediction in terms of functional disability and mortality at 1 year among ICU-admitted severe stroke patients: a prospective epidemiological study in the south of the European Union (Evascan Project, Andalusia, Spain). Intensive Care Med 29, 1237–1244 (2003). https://doi.org/10.1007/s00134-003-1755-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-003-1755-6