
Abstract
Objective
Systemic leukocyte activation is claimed to trigger inflammatory response and remote organ dysfunction in acute pancreatitis. Chemokines are inflammatory mediators with potent leukocyte-activating properties and have been shown to be involved in the pathophysiological process of experimental acute pancreatitis. However, as little is known about their role in human disease we investigated local and systemic concentrations of different CC-chemokine members in patients with acute pancreatitis.
Patients and methods
We included 68 patients with acute pancreatitis in the present study. Local complications in terms of necrosis were present in 37 (54%) patients of whom 21 (57%) developed pancreatic infections. Monocyte chemoattractant protein-1 (MCP-1), macrophage inflammatory protein-1α (MIP-1α) and macrophage inflammatory protein-1β (MIP-1β) concentrations were measured daily over 2 weeks after study inclusion by ELISA in sera and lesser sac aspirates.
Results
MCP-1 serum concentrations showed a dramatic increase in patients who developed local complications and/or remote organ failure. Herein, a close correlation was found between the severity of remote organ failure and the degree of MCP-1 elevation. Multiple regression analysis identified pancreatic infections as well as renal and cardiocirculatory failure as independent variables associated with enhanced systemic MCP-1 release. MIP-1α levels remained unaffected by local complications and showed a significant increase only; if multiple organ dysfunction syndrome (MODS) developed or patients subsequently died. In contrast, MIP-1β concentrations correlated with neither the presence nor the severity of any complication. Compared with systemic concentrations, local lesser sac aspirates revealed significantly higher levels of MCP-1, whereas MIP-1α and MIP-1β were not different.
Conclusions
Complicated acute pancreatitis is associated with significantly elevated local and systemic concentrations of the CC-chemokine MCP-1. Our results suggest that, among the CC-chemokine members investigated, MCP-1 might play a pivotal role in the pathological mechanism of complicated acute pancreatitis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute pancreatitis is characterized by wide clinical variation ranging from a mild self-limiting to a severe life-threatening disease carrying high mortality rates. It is well established that the development of pancreatic necrosis is the main prognostic factor in acute pancreatitis. The presence of intra- and extra-pancreatic necrosis strongly influences the risk of infected necrosis [1, 2, 3] and remote organ failure [2, 3, 4], which is further associated with a significant increase in mortality rate [1, 3, 5]. A large number of experimental studies have shown that the subsequent infiltration of different leukocyte subsets into the damaged gland are the major source of the release of various toxic mediators such as proteolytic enzymes [6], oxygen free radicals [7, 8] and cytokines [9, 10], which enhance pancreatic tissue destruction and promote remote organ failure.
Chemokines are a family of small (8–10 kDa), inducible, secreted cytokines with chemotactic and activating effects on different leukocyte subsets; thus they provide a key stimulus for directing leukocytes to the areas of injury [11]. Chemokines can be subdivided on a structural basis into the CXC-subfamily in which the first two of four conserved cysteine residues are separated by another amino acid and the CC-subfamily, in which the first two cysteine residues are adjacent. The structural classification of the chemokines also determines their biological activity: while a subgroup of the CXC-chemokines, such as interleukin-8, are potent neutrophil chemoattractants and activators, the CC-chemokines, comprising monocyte chemoattractant protein (MCP)-1, -2, -3, macrophage inflammatory protein (MIP)-1α and -1β, RANTES and eotaxin predominantly affect monocytes [10, 11]. Chemokines bind to specific receptors which can be broadly divided into those that bind a single chemokine or those that bind a number of chemokines of either CXC- or CC-type [12]. With respect to the CC-chemokines, the CC-CKR-2 receptor is exclusively located on monocytes and specific for MCP-1, whereas the CC-CKR-1, -3, -4, and -5 receptors are to be found on monocytes, eosinophil and basophil granulocytes as well as on T-cells, and variably bind to MCP-1, MIP-1α or MIP-1β [12, 13].
Recent experimental data suggest that chemokines may be important inflammatory mediators within the early pathophysiological process of acute pancreatitis, promoting distant organ failure. In various experimental models an early upregulation of CXC-chemokines, such as mob-1 / IP10 [14] or cytokine-induced neutrophil chemoattractant (CINC) [15], as well as CC-chemokines, such as MCP-1 [14, 15, 16] and RANTES, has been observed [16]. Moreover, pancreatitis-associated pulmonary damage is significantly attenuated following the application of neutralizing antibodies against CINC [17] or in mice deficient in the CC-CKR-1 gene [18].
With respect to the clinical setting, elevated plasma levels of the CXC-chemokines ENA-78 and GRO-α revealed a close correlation with disease severity in human acute pancreatitis [19], however, little is known about the course and dynamics of CC-chemokines in this context. To address this issue we assessed local and systemic concentrations of the CC-chemokines MCP-1, MIP-1α and MIP-1β in a morphologically and clinically well-defined patient series with acute pancreatitis.
Materials and methods
Patients
Sixty-eight patients with acute pancreatitis entered the present study at the Department of General Surgery, University hospital at Ulm during the time from November, 1994, to June, 1999. Inclusion criteria were typical upper abdominal pain and at least three-fold elevated serum amylase and/or lipase levels. The median time interval between onset of symptoms and admission to hospital was 25 (range 0–141) h, patients were recruited in median on the 2nd day (range 1–7) of disease. Local complications comprised the development of intra-/extra-pancreatic necrosis and pancreatic infections, which were diagnosed on the basis of diagnostic imaging procedures and/or intraoperative findings as previously reported [20]. Thirty-one (46%) patients suffered from interstitial edematous (AIP) and 37 (54%) from necrotizing pancreatitis (NP), of which 21 (57%) developed pancreatic infections in terms of infected necrosis and pancreatic abscess. Pancreatic infections comprised primary pancreatic infections (n=13) and secondary/postoperative pancreatic infections occurring after surgery for sterile necrosis (n=8).
The biological data and etiology of pancreatitis in the morphological entities AIP and NP as well as in the total series of patients are summarized in Table 1. The extent of intra-pancreatic necrosis in the patient groups with sterile necrosis and pancreatic infections did not differ. Remote organ complications included pulmonary (arterial PO2 <60 mmHg at room air or mechanical ventilation), renal (serum creatinine >200 µmol/l or hemofiltration/dialysis) and cardiocirculatory insufficiency (need for inotropics); multiple organ dysfunction syndrome (MODS) was defined as failure of all three organ systems requiring mechanical ventilation, hemofiltration and inotropics. The overall severity of pancreatitis in terms of Ranson and APACHE II scores and the incidence of local and remote organ complications are presented in Table 2.
Initial treatment was conservative in all patients and included maximum intensive care support as well as the prophylactic administration of appropriate antibiotics in patients with pancreatic necrosis. Indications for surgery were: (1) the presence of documented infection of necrosis with systemic signs of sepsis and (2) persisting organ failure or abdominal symptoms despite maximum intensive care support in the absence of positive FNA results. Twelve of 37 patients (32%) with NP were treated by conservative means, 25 (68%) patients underwent necrosectomy and postoperative continuous closed lavage of the lesser sac. Cholecystectomy was performed in two conservatively treated patients with biliary NP and in 18 patients with biliary AIP. One patient with AIP was subjected to laparotomy due to persisting ileus.
Methods
The study was approved by the local ethics committee of the University of Ulm, Germany, and informed consent was obtained from all patients before study inclusion. Blood samples were drawn from central venous lines in 24-h intervals over 14 days. Thereafter, blood was immediately spun at 3,500 g at 4°C for 10 min, divided up and stored at −70°C until later assay. Peri-pancreatic exsudate was obtained by guided fine needle aspiration in patients with suspected pancreatic infection or during surgery on day 6 (median, range 2–15) of acute pancreatitis and was available for analysis in 14 patients. All local measurements were compared with the corresponding systemic chemokine concentrations of the same day the local sample was taken. Concentrations of MCP-1 (reference range 133–1245 pg/ml in healthy subjects), MIP-1α (reference range 0–48 pg/ml in healthy subjects) and MIP-1β (reference range 42–264 pg/ml in healthy subjects) were measured by commercially available enzyme-linked immunosorbent assays (ELISA) (Endogen, Woburn, MA, USA) according to the manufacturer's protocol. Values of the respective parameters were related to the onset of symptoms starting with day 1 as the first day of acute pancreatitis.
Statistics
All variables are presented as medians + upper/lower quartiles or ranges. For comparison of independent samples we used the Wilcoxon's rank sum test and the Fisher's exact test for comparison of proportions. Probability values less than 0.05 at an α less than 0.05 were considered significant. Receiver operating characteristic (ROC) curves and the respective areas under the curve (AUC) were calculated for the two highest values of each parameter reached during the whole observation period. Cut-off levels were determined as the value which optimized sensitivity (patients with local or systemic complications), specificity (patients without local or systemic complications) and likelihood ratio: LR = (probability of true positive + probability of true negative)/(probability of false positives + probability of false negatives). Multiple regression analysis was performed by using the two highest values of MCP-1, MIP-1α and MIP-1β reached within the whole observation period as dependent variables and the following complications as potential independent variables: necrosis, pancreatic infection, pulmonary, renal, cardiocirculatory failure, MODS and death. All statistical calculations were made with the MedCalc Software package [21].
Results
Monocyte chemoattractant protein-1 concentrations increased early in patients who developed local complications such as necrosis (Fig. 1, p<0.01–0.00001) or pancreatic infections (Fig. 2, p<0.05–0.002) during the course of the disease. In patients who did not develop necrosis or pancreatic infections MCP-1 levels remained within normal limits. In contrast, MIP-1α and MIP-1β concentrations did not show any significant elevation dependent on the presence of either of the local complications.

Course of monocyte chemoattractant protein-1 (MCP-1) (median ± upper/lower quartile) in patients with necrotizing (NP) and edematous (AIP) acute pancreatitis. MCP-1 concentrations were significantly higher in NP from day 2 of acute pancreatitis. In patients wit AIP MCP-1 remained within the reference range

Course of monocyte chemoattractant protein-1 (MCP-1) (median ± upper/lower quartile) in patients with pancreatic infections (PI) and sterile necrosis (SN). In patients developing pancreatic infections MCP-1 concentrations were significantly higher from day 4 of the disease, whereas in SN MCP-1 did not exceed the upper reference range
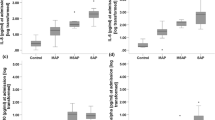
The occurrence of single or combined remote organ failure strongly influenced systemic MCP-1 release: patients with pulmonary failure revealed significantly higher MCP-1 levels from day 2 after the onset of symptoms compared to patients without this complication (Fig. 3, p<0.04–0.00001). Similar observations were made for the presence of renal failure/hemofiltration (p<0.01–0.00001) and for cardiocirculatory failure/inotropic treatment (p<0.02–0.00001) with significantly elevated MCP-1 levels from day 2 after the onset of symptoms. If MODS developed, MCP-1 concentrations were dramatically increased and remained this level following the first day of acute pancreatitis (Fig. 4, p<0.01–0,00001). MIP-1β levels remained unaffected by any single organ failure and MODS throughout the whole observation period (data not shown). MIP-1α levels significantly increased in patients with MODS during the second week of the disease only (Fig. 5, p<0.05–0.01), whereas single organ failure had no influence. However, even in patients with MODS the rise of MIP-1α was by far less marked than that of MCP-1. We did not observe a correlation between the patients' gender or the etiology of acute pancreatitis and the degree of MCP-1 or MIP-1α elevation. Local MCP-1 concentrations in ascites or peri-pancreatic exsudate were at least twice as high as the corresponding systemic levels, whereas local and systemic MIP-1α and MIP-1β levels did not differ (Table 3).

Course of monocyte chemoattractant protein-1 (MCP-1) in patients with (PI+) and without (PI−) pulmonary failure. If pulmonary failure was present, MCP-1 levels significantly exceeded the upper normal reference range from day 2 of the disease

Course of monocyte chemoattractant protein-1 (MCP-1) in patients with (MODS+) and without (MODS−) multiple organ dysfunction syndrome. A dramatic increase of MCP-1 levels was observed in patients with MODS from the 2nd day of acute pancreatitis

Course of macrophage inflammatory protein-1α (MIP-1α) in patients with (MODS+) and without (MODS−) multiple organ dysfunction syndrome. In patients developing MODS MIP–1α concentrations were significantly higher during the 2nd week of the disease
Receiver operating characteristics (ROC) analysis was based on the two highest MCP-1, MIP-1α and MIP-1β values reached within the total observation period of 14 days. The results confirmed the high correlation of MCP-1 levels with the development of pancreatic necrosis and infection, single or combined remote organ failure as well as the absence of any correlation of MIP-1β concentrations in this respect. Table 4 summarizes the results of ROC analysis including the optimum cut-off levels and areas under the curve (AUC) for the prediction of pancreatic necrosis, pancreatic infections, pulmonary, renal or cardiocirculatory failure, MODS and death, of MCP-1, MIP-1α and MIP-1β.
Multiple regression analysis revealed that only pancreatic infections (correlation coefficient: r=0.671, p=0.008) as well as renal (correlation coefficient: r=0.847, p=0.001) and cardiocirculatory failure (correlation coefficient: r=0.760, p=0.01) were independent variables associated with enhanced systemic MCP-1 release, whereas necrosis (correlation coefficient: r=0.564, p=n.s.), pulmonary insufficiency (correlation coefficient: r=0.683, p=n.s.), MODS (correlation coefficient: r=0.829, p=n.s.) and death (correlation coefficient: r=0.642, p=n.s.) were not.
Discussion
Since our knowledge about the pathophysiology of acute pancreatitis has evolved considerably, it is well known that leukocytes and leukocyte-derived products contribute to pancreatic damage and trigger systemic inflammatory response as well as remote organ failure. A number of experimental studies have shown that activation of the monocyte/macrophage system is an important step in the severity progression of acute pancreatitis [22, 23, 24, 25, 26]. Because monocytes/macrophages represent a major source of proinflammatory cytokine release [9, 27], the beneficial effects of an inhibited activation of this cellular system is believed to be the consequence of decreased cytokine production [24, 25]. Currently, there is no more doubt that proinflammatory cytokine activation is detrimental in terms of the development of local and systemic complications in acute pancreatitis [9, 28].
Our results demonstrate that both local and systemic levels of the CC-chemokine member MCP-1 are already dramatically increased early in the course of severe acute pancreatitis in humans. Herein, the degree of systemic MCP-1 elevation showed the closest correlation with the development of pancreatic infections and with remote organ failure affecting the kidneys and the cardiocirculatory system. In fact, the results of this observational study do not allow any firm pathophysiological conclusions, however, they are well in line with previous experimental studies in this field [14, 15, 16]. In vitro experiments in isolated pancreatic acinar cells have shown that acinar cells themselves are an important source of chemokine production within the first hours after induction of acute pancreatitis [14, 15, 16]. As chemokines are typically induced and released at the site of injury [11, 12], the early MCP-1 chemokine expression in both experimental and human acute pancreatitis supports the concept of a signal originating from the acinar cells to attract inflammatory cells to the site of acinar cell injury. As a consequence, chemokine activation may be considered as a potential link between the process of local pancreatic injury, via induction of leukocyte infiltration, and the subsequent release of various inflammatory mediators to a systemic process involving distant organ systems [29, 30, 31].
Although local MCP-1 concentrations were significantly elevated in our clinical series as well, the correlation between systemic MCP-1 release and the development of remote organ failure was far stronger. This observation is probably biased by the fact that local chemokine measurements were only possible in 14 patients who, in addition, all suffered from severe disease. On the other hand, multiple regression analysis revealed the closest correlation between renal and cardiocirculatory failure and the degree of circulating MCP-1 concentrations. On the basis of these findings it could be hypothesized that MCP-1 is more important for mediating systemic rather than local severity in acute pancreatitis. This clinical observation is again supported by recent experimental studies in which a predominance of chemokine-mediated systemic effects have been described [17, 18].
In mice carrying a genetic deletion of the CC-CKR-1 receptor, supramaximal cerulein stimulation resulted in a significant reduction of pancreatitis-associated lung injury, pulmonary myeloperoxidase activity and both pulmonary and systemic TNF-α expression. In contrast, intra-pancreatic edema formation and acinar cell damage remained completely unchanged [18]. A similar observation has been made for the neutrophil-inducing CXC-chemokine CINC: the application of a CINC-neutralizing antibody in rats with cerulein-induced pancreatitis was more effective in preventing pancreatitis-associated lung injury than ameliorating pancreatic necrosis [17].
Our data clearly demonstrate significantly different expression profiles of the CC-chemokine members MCP-1, MIP-1α and -1β in acute pancreatitis. In terms of MIP-1α, we found some correlation with the development of severe combined remote organ failure, however this was far less marked than this correlation observed for MCP-1. In terms of MIP-1β, no significant elevation was present, irrespective of whether any kind of local or systemic complication developed or not. In addition, local concentrations of both MIP-1α and MIP-1β in peri-pancreatic exudates and ascites remained within the normal reference ranges.
From these observational data it is hard to draw any conclusions as to whether this may be of pathophysiological relevance. However, a similar predominance of MCP-1 over MIP-1α and MIP-1β release has been described in other human inflammatory diseases. In chronic bronchitis bronchoalveolar concentrations of MCP-1 were significantly elevated but, in contrast to acute pancreatitis, an elevation of MIP-1β was also found and was associated with chronic obstructive disease, whereas MIP-1α levels were not detectable [32]. In alcoholic liver disease systemic concentrations of MCP-1 were markedly increased and correlated with the severity of hepatic inflammation; systemic MIP-1α levels remained within normal limits [33], however, both MCP-1 and MIP-1α secretion from peripheral blood mononuclear cells was increased in patients with severe alcoholic hepatitis. Enhanced expression of MCP-1, but not of MIP-1α, was found in colonic biopsies in patients with ulcerative colitis [34]. In chronic pancreatitis various CC-chemokines, especially MCP-1, were found to be differentially expressed depending on the severity of the structural changes [35]. Interestingly, in accordance with in vitro findings in experimental acute pancreatitis, pancreatic acinar cells and not the inflammatory infiltrate were found to be the main source of chemokine synthesis in this study [35]. Taken together, although no proof, these data imply a dominant role for the CC-chemokine MCP-1 in inflammatory disorders and are well in accordance with our findings in acute pancreatitis in humans.
In the absence of experimental studies employing a direct approach to MCP-1 inhibition by either neutralizing antibodies or the use of MCP-1-deficient mice, the definite role of this CC-chemokine in acute pancreatitis remains to be defined. Recent studies in MCP-1 knockout mice have revealed a uniquely essential role of this chemokine in different inflammatory models such as aseptic peritonitis, contact hypersensitivity, tuberculin–type hypersensitivity, pulmonary granulomatosis and tuberculosis [31]. Unfortunately, to date no studies are available which address the effects of CC-chemokine inhibition, especially of MCP-1 inhibition, on mortality in models of severe inflammation such as necrotizing pancreatitis or bacterial peritonitis/sepsis. This information will be of central importance as to whether anti-chemokine strategies in general could be of any therapeutic benefit in the clinical setting.
In summary, the CC-chemokine members MCP-1, MIP-1α and MIP-1β reveal different expression profiles in clinically severe acute pancreatitis. Whereas MIP-1β concentrations remained within normal ranges in the course of the disease, MIP-1α levels were increased in patients with multi-organ dysfunction only. In contrast, a marked and sustained elevation of MCP-1 concentrations was observed in patients with local complications as well as single and combined remote organ failure. Our results suggest that MCP-1 might play a dominant role in the pathological mechanism of complicated acute pancreatitis with specific regard to the development of systemic disease severity and distant organ failure. Based on the current experimental and clinical knowledge, further studies employing MCP-1-inhibiting strategies in inflammatory disorders, including acute pancreatitis, seem to be promising.
References
Beger HG, Bittner R, Block S, Büchler M (1986) Bacterial contamination of pancreatic necrosis. Gastroenterology 49:433–438
Isenmann R, Rau B, Beger HG (1999) Bacterial infection and extent of necrosis are determinants of organ failure in patients with acute necrotising pancreatitis. Br J Surg 86:1020–1024
Tran DD, Cuesta MA, Schneider AJ, Wesdorp RI (1993) Prevalence and prediction of multiple organ system failure and mortality in acute pancreatitis. J Crit Care 8:145–153
Tenner S, Sica G, Hughes M, Noordhoek E, Feng S, Zinner M, Banks PA (1997) Relationship of necrosis to organ failure in severe acute pancreatitis. Gastroenterology 113:899–903
Banerjee AK, Kaul A, Bache E, Doran J, Nicholson ML (1994) Multicentre audit of death from acute pancreatitis. Br J Surg 81:1541
Rinderknecht H (1994) Genetic determinants of mortality in acute necrotizing pancreatitis. Int J Pancreatol 16:11–15
Inoue S, Nakao A, Kishimoto W, Murakami H, Harada A, Nonami T, Takagi H (1996) LFA–1 (CD11a/CD18) and ICAM–1 (CD54) antibodies attenuate superoxide anion release from polymorphonuclear leukocytes in rats with experimental acute pancreatitis. Pancreas 12:183–188
Rau B, Poch B, Gansauge F, Bauer A, Nüssler AK, Nevalainen T, Schoenberg MH, Beger HG (2000) Pathophysiological role of oxygen free radicals in acute pancreatitis: initiating event or mediator of tissue damage? Ann Surg 231:352–360
Norman J (1998) The role of cytokines in the pathogenesis of acute pancreatitis. Am J Surg 175:76–83
Brady M, Christmas S, Sutton R, Neoptolemos J, Slavin J (1999) Cytokines and acute pancreatitis. Baillieres Clin Gastroenterol 13:265–289
Rollins BJ (1997) Chemokines. Blood 90:909–928
Premark BA, Schall TJ (1996) Chemokine receptors: gateway to inflammation and infection. Nat Med 11:1174–1178
Murphy PM (1994) The molecular biology of leukocyte chemoattractant receptors. Ann Rev Immunol 12:593–633
Grady T, Liang P, Ernst SA, Logsdon CD (1997) Chemokine gene expression in rat pancreatic acinar cells is an early event associated with acute pancreatitis. Gastroenterology 113:1966–1975
Bhatia M, Brady M, Christmas S, Neoptolemos JP, Slavin J (1999) Effect of caerulein on chemokine production from cultured rat pancreatic acini (abstract). Pancreas 19:415
Yang BM, Demaine AG, Kingsnorth A (2000) Chemokines MCP-1 and RANTES in isolated rat pancreatic acinar cells treated with CCK and ethanol in vitro. Pancreas 21:22–31
Bhatia M, Brady M, Zagorski J, Christmas SE, Campbell F, Neoptolemos JP, Slavin J (2000) Treatment with neutralizing antibody against cytokine-induced neutrophil chemoattractant (CINC) protects rats against acute pancreatitis associated lung injury. Gut 47:838–844
Gerard C, Frossard JL, Bhatia M, Saluja A, Gerard NP, Lu B, Steer ML (1997) Trageted disruption of the β–chemokine receptor CCR-1 protects against pancreatitis associated lung injury. J Clin Invest 100:2022–2027
Shokui S, Bhatia M, Brady M, Christmas S, Neoptolemos JP, Slavin J (2000) Plasma levels of the CXC-chemokines ENA-78 and GRO-α are elevated in severe pancreatitis (abstract). Digestion 61:284
Rau B, Steinbach G, Gansauge F, Mayer J, Grunert A, Beger HG (1997) The potential role of procalcitonin and interleukin-8 in the prediction of infected necrosis in acute pancreatitis. Gut 41:832–840
Schoonjans F, Zalata A, Depuydt CE, Comhaire FH (1995) MedCalc: a new computer program for medical statistics. Comp Meth Prog Biomed 48:257–262
Wang X, Andersson R, Soltesz V, Leveau P, Ihse I (1996) Gut origin sepsis, macrophage function and oxygen extraction associated with acute pancreatitis in the rat. World J Surg 20:299–307
Andersson R, Deng XM, Wang XD (1997) Role of macrophage overactivation in the development of acute pancreatitis injury in rats. Br J Surg 84:775–780
Yang J, Denham W, Tracey KJ, Wang H, Kramer AA, Salhab KF, Norman J (1998) The physiologic consequences of macrophage pacification during severe acute pancreatitis. Shock 10:169–175
Yang J, Denham W, Carter G, Tracey KJ, Norman J (1998) Macrophage pacification reduces rodent pancreatitis-induced hepatocellular injury through down-regulation of hepatic tumor necrosis factor α and interleukin-1β. Hepatology 28:1282–1288
Yamaguchi Y, Okabe K, Liang J, Matsumura F, Akizuki E, Matsuda T, Ohshiro H, Nakano S, Ishihara K, Ogawa M (1999) The novel carboxamide derivate IS–741 reduces neutrophil chemoattractant production by bronchoalveolar macrophages in rats with cerulein-induced pancreatitis complicated by sepsis. Digestion 60:152–160
Fink GW, Norman J (1996) Intrapancreatic interleukin-1 beta gene expression by specific leukocyte populations during acute pancreatitis. J Surg Res 63:369–373
Denham W, Norman J (1999) The potential role of therapeutic cytokine manipulations in acute pancreatitis. Surg Clin North Am 79:767–781
Jiang Y, Beller DI, Frendl G, Graves DT (1992) Monocyte chemoattractant protein-1 regulates adhesion molecule expression and cytokine production in human monocytes. J Immunol 148:2423–2428
Boring L, Gosling J, Chensue SW, Kunkel SL, Farese RV, Broxmeyer HE, Charo IF (1997) Impaired monocyte migration and reduced type 1 (Th1) cytokine responses in CC-chemokine receptor-2 knockout mice. J Clin Invest 100:2552–2561
Lu B, Rutledge BJ, Gu L, Fiorillo J, Lukacs NW, Kunkel SL, North R, Gerard C, Rollins BJ (1997) Abnormalities in monocyte recruitment and cytokine expression in monocyte chemoattractant protein 1 deficient mice. J Exp Med 187:601–608
Capelli A, Di Stefano A, Gnemmi I, Balbo P, Cerutti CG, Balbi B, Lusuardi M, Donner CF (1999) Increased MCP-1 and MIP-1β in bronchoalveolar lavage fluid of chronic bronchitis. Eur Respir J 14:160–165
Fisher NC, Neil DAH, Williams A, Adams DH (1999) Serum concentrations and peripheral secretion of the beta chemokines monocyte chemoattractant protein 1 and macrophage inflammatory protein 1α in alcoholic liver disease. Gut 45:416–420
Uguccioni M, Gionchetti P, Robbiani DF, Rizzello F, Peruzzo S, Campieri M, Baggiolini M (1999) Increased expression of IP-10, IL-8, MCP-1 and MCP-3 in ulcerative colitis. Am J Pathol 155:331–336
Saurer L, Reber P, Schaffner T, Büchler MW, Buri C, Kappeler A, Walz A, Friess H, Mueller C (2000) Differential expression of chemokines in normal pancreas and chronic pancreatitis. Gastroenterology 118:356–367
Acknowledgements
This work was, in part, supported by the Deutsche Forschungsgemeinschaft, grant SFB/A6 to B. Rau.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rau, B., Baumgart, K., Krüger, C.M. et al. CC-chemokine activation in acute pancreatitis: enhanced release of monocyte chemoattractant protein-1 in patients with local and systemic complications. Intensive Care Med 29, 622–629 (2003). https://doi.org/10.1007/s00134-003-1668-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-003-1668-4