
Abstract
Objective. The aim of the study was to investigate the effect of lung volume changes on end-expiratory lung impedance change (ELIC) in mechanically ventilated patients, since we hypothesized that ELIC may be a suitable parameter to monitor lung volume change at the bedside.
Design. Clinical trial on patients requiring mechanical ventilation.
Settings. Intensive care units of a university hospital.
Patients. Ten mechanically ventilated patients were included in the study.
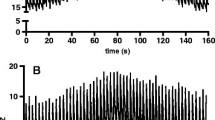
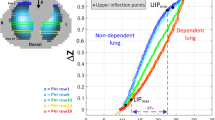
Intervention. Patients were ventilated in volume-controlled mode with constant flow and respiratory rate. In order to induce changes in the end-expiratory lung volume (EELV), PEEP levels were increased from 0 mbar to 5 mbar, 10 mbar, and 15 mbar. At each PEEP level EELV was measured by an open-circuit nitrogen washout manoeuvre and ELIC was measured simultaneously using Electrical Impedance Tomography (EIT) with sixteen electrodes placed on the circumference of the thorax and connected with an EIT device. Cross-sectional electro-tomographic measurements of the thorax were performed at each PEEP level, and a modified Sheffield back-projection was used to reconstruct images of the lung impedance. ELIC was calculated as the average of the end-expiratory lung impedance change.
Results. Increasing PEEP stepwise from 0 mbar to 15 mbar resulted in an linear increase of EELV and ELIC according to the equation: y =0.98 × –0.68, r 2 =0.95.
Conclusion. EIT is a simple bedside technique which enables monitor lung volume changes during ventilatory manoeuvres such as PEEP changes.
Article PDF
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Author information
Authors and Affiliations
Additional information
Electronic Publication
Rights and permissions
About this article
Cite this article
Hinz, .J., Hahn, .G., Neumann, .P. et al. End-expiratory lung impedance change enables bedside monitoring of end-expiratory lung volume change. Intensive Care Med 29, 37–43 (2003). https://doi.org/10.1007/s00134-002-1555-4
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s00134-002-1555-4